Atezolizumab Plus Bevacizumab for Advanced Hepatocellular Carcinoma with Macroscopic Vascular Invasion: An Inverse Probability of Treatment Weighted Analysis
Jihoon Kim, Jin-Hyoung Kim, Byung Soo Im, Gun Ha Kim, Hee Ho Chu, Dong Il Gwon, Ji Hoon Shin, Ju Hyun Shim, Sang Min Yoon, Sehee Kim

TL;DR
A drug combination delayed liver cancer growth as effectively as traditional treatments, with similar safety and survival rates in patients with advanced disease.
Contribution
This study provides real-world evidence comparing drug therapy and locoregional treatments for advanced liver cancer with vascular invasion.
Findings
The drug combination delayed cancer progression more effectively than locoregional therapy.
Overall survival and serious side effect rates were similar between the two treatment approaches.
Objective response rates and major adverse events were comparable across both treatment groups.
Abstract
Patients with liver cancer that grows into major blood vessels typically have a poor outlook and limited treatment options. Clinicians often choose between two very different approaches: a modern drug combination (atezolizumab plus bevacizumab) or locoregional treatments such as targeted chemotherapy delivered into the liver, sometimes combined with radiation. However, it has not been clear which option works better for these high-risk patients. In this study, we examined real-world outcomes from nearly 500 patients to compare these two strategies fairly. We found that the drug combination delayed cancer progression for a longer period, while overall survival and rates of serious side effects were similar between the two approaches. These findings provide practical evidence to help guide treatment decisions and support more personalized care for patients with advanced liver cancer…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
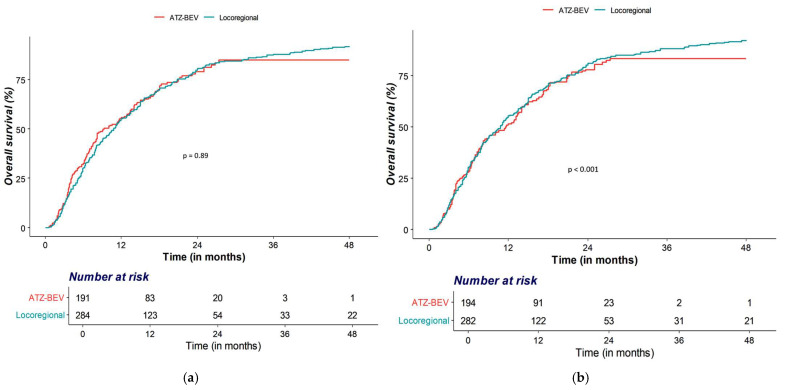 Figure 1
Figure 1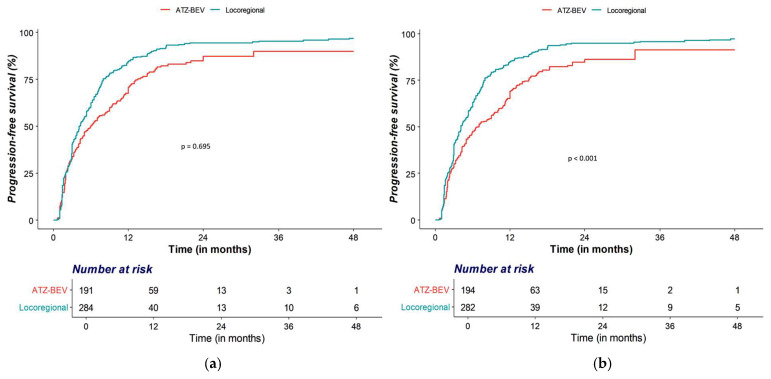 Figure 2
Figure 2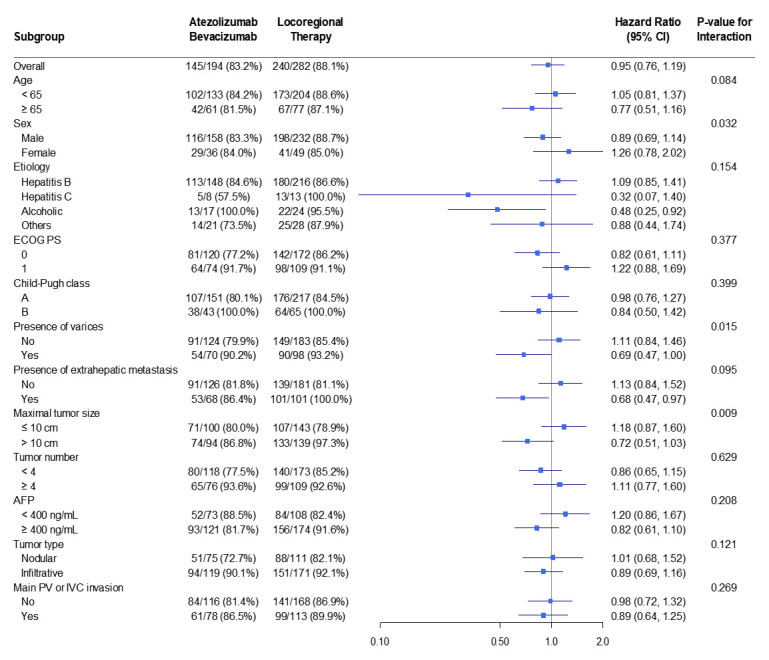 Figure 3
Figure 3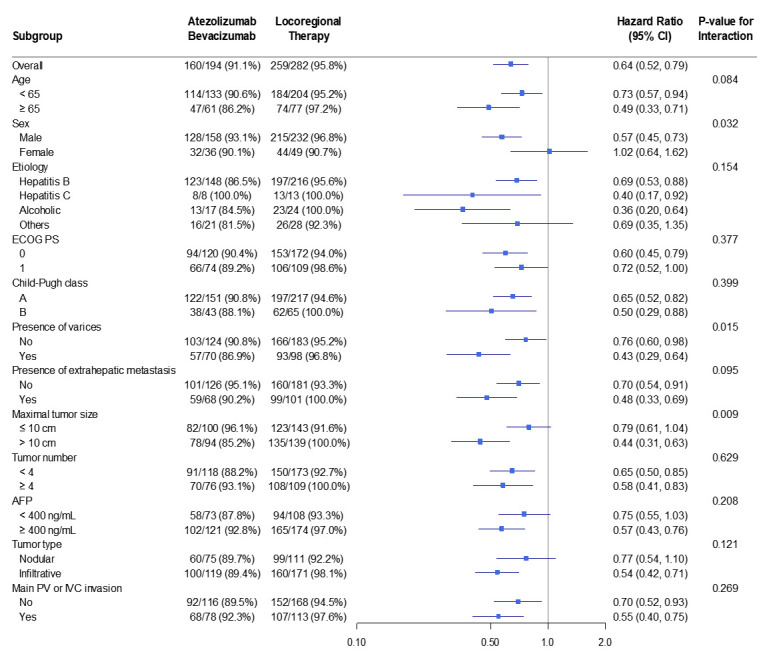 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Cholangiocarcinoma and Gallbladder Cancer Studies · Organ Transplantation Techniques and Outcomes
1. Introduction
Treatment of advanced hepatocellular carcinoma (HCC) remains a major clinical challenge. Despite advances in surveillance and imaging, more than half of patients are still diagnosed at intermediate or advanced stages, when curative options are rarely feasible and prognosis is poor. The presence of macrovascular invasion (MVI) further limits therapeutic choices and worsens outcomes [1,2,3]. Current international guidelines recommend systemic therapy as the standard of care for HCC with MVI, with the 2022 update of the Barcelona Clinic Liver Cancer (BCLC) strategy identifying immunotherapy-based regimens as first-line options [4,5].
Among available regimens, atezolizumab plus bevacizumab (Atezo–Bev) has become the preferred first-line therapy based on the IMbrave150 trial, which demonstrated significant improvements in overall survival (OS) and progression-free survival (PFS) compared with sorafenib, supported by updated subgroup analyses. This demonstrable clinical superiority led the BCLC 2022 staging system update to designate immunotherapy-based regimens as the new first-line standard for advanced HCC, fundamentally shifting the treatment paradigm away from solely tyrosine kinase inhibitors [4,5]. The robust efficacy of this regimen is attributed to a synergistic mechanism: bevacizumab’s inhibition of VEGF not only limits tumor angiogenesis but also re-models the immunosuppressive tumor microenvironment, thereby enhancing T-cell infiltration and the anti-tumor activity of atezolizumab’s PD-L1 blockade [6,7,8]. Subsequent studies have confirmed its efficacy and manageable safety profile across diverse populations [9,10,11].
In real-world practice, locoregional therapy—defined as transarterial chemoembolization (TACE) with or without external-beam radiotherapy (RT)—continues to play a major role for patients with MVI, particularly in East Asia [12,13]. A randomized clinical trial showed that TACE combined with RT (TACE + RT) achieved superior OS and PFS compared with sorafenib, underscoring its potential benefit in selected patients [14]. These results have influenced regional guidelines, which now recommend both systemic immunotherapy and selected locoregional combinations for patients with vascular invasion [15].
However, direct comparative data between Atezo–Bev and contemporary locoregional therapy for HCC with MVI remain limited. A recent multicenter study compared outcomes of Atezo–Bev with TACE + RT in patients with portal vein tumor thrombosis (PVTT); however, its scope was restricted to that subgroup and did not address the broader MVI spectrum. Therefore, this study aimed to evaluate whether Atezo–Bev provides superior survival and disease control compared with locoregional therapy in treatment-naïve patients with unresectable HCC and MVI, using propensity score weighting to minimize baseline imbalance [16].
2. Materials and Methods
2.1. Study Eligibility
This study was approved by the Institutional Review Board of Asan Medical Center (approval No. 2024-1408) on 25 November 2024, which waived the requirement for patient consent due to its retrospective design. Inclusion criteria were image- or biopsy-confirmed HCC based on recent international guidelines [17,18], HCC with MVI, Child–Pugh class A or B liver function, and an Eastern Cooperative Oncology Group (ECOG) performance status of 0–1. Exclusion criteria were applied to ensure patient safety and to minimize confounding variables in this comparative retrospective analysis. These included Child–Pugh class C liver function (due to the heightened risk of drug-related toxicity and poor prognosis), total serum bilirubin ≥ 3 mg/dL (indicating severe hepatic dysfunction), tumor involvement of more than half of the liver (due to extremely poor prognosis and high risk of hepatic failure), or ECOG performance status 3–4 (as these patients are generally unable to tolerate aggressive first-line therapies and poor performance status is a strong confounding factor for survival outcomes). Patients who received Atezo–Bev or locoregional therapy (cisplatin-based TACE delivered through the hepatic artery, with or without external-beam RT directed to the MVI) as first-line treatment for treatment-naïve HCC with MVI were included. Between November 2020 and June 2024, 191 treatment-naïve patients with HCC were among 284 treatment-naïve patients with HCC and MVI who received first-line TACE + RT or TACE alone between January 2018 and October 2020.
2.2. Atezo–Bev Treatment
Patients received bevacizumab 15 mg/kg and atezolizumab 1200 mg intravenously every 3 weeks, following the IMbrave150 trial protocol [6,8]. Dose adjustments or permanent discontinuation of either agent were performed primarily based on the occurrence of adverse events graded according to the Society of Interventional Radiology (SIR) Classification System for Complications. Specifically, treatment was interrupted or permanently discontinued for Grade 3 or higher adverse events that were considered treatment-related and clinically unmanageable, following institutional guidelines [19,20]. Therapy continued until patients experienced unacceptable toxicity or disease progression [12].
2.3. TACE
Cisplatin-based TACE was performed using a cisplatin dose of 2 mg/kg. Through a microcatheter, 4–20 mL of a 1:1 emulsion of cisplatin and iodized oil (Lipiodol^®^, Guerbet, Roissy, France) was infused into the lobar, segmental, or subsegmental feeding artery, followed by embolization with Gelfoam slurry (Upjohn, Kalamazoo, MI, USA) until arterial flow was nearly stagnant [20]. In patients with significant arteriovenous or arterioportal shunts, initial embolization with Gelfoam slurry was performed to occlude the shunt, followed by infusion of the iodized oil/cisplatin emulsion and additional Gelfoam embolization [21]. For patients with main PVTT and poorly developed collaterals, transarterial chemotherapeutic infusion without Gelfoam was performed [22].
TACE was repeated every 4–6 weeks if residual viable tumor tissue was detected on follow-up CT without deterioration of hepatic function. In some patients (n = 29), only TACE was performed because of limited tumor thrombus extent or refusal of additional RT. TACE alone was also performed when EBRT was not feasible because of liver reserve, anatomic limitations, prior radiation, or patient refusal. These indications reflect institutional practice standards during the study period.
2.4. External-Beam RT
RT methods at our institution have been described previously [22,23]. Patients began RT for vascular invasion within 3 weeks of the initial TACE. Four-dimensional CT simulation (GE Healthcare, Waukesha, WI, USA) was performed during free breathing in all patients. The synchronized four-dimensional CT images were divided into 10 series according to respiratory phase (Advantage 4D version 4.2; GE Healthcare, Waukesha, WI, USA). Respiratory motion was tracked using a real-time position management gating system (Varian Medical Systems, Palo Alto, CA, USA).
Gross tumor volume (GTV) for large, multiple, or infiltrative HCCs included the tumor thrombus and a 2 cm margin into contiguous HCC at end-expiration. For small HCCs encompassed within a single radiation port, GTV included the entire tumor and thrombus [22,23]. The internal target volume (ITV) was defined as the sum of all GTVs across gated respiratory phases, and the planning target volume (PTV) was defined as the ITV plus 0.7 cm margins [22,23].
Target volumes, radiation ports, and doses were determined using a three-dimensional conformal planning system (Eclipse version 10.0, Varian Medical Systems, Palo Alto, CA, USA). Radiation was delivered via a respiratory-gated beam technique, with a total dose of 45 Gy in 2–5 Gy fractions, five times per week, using 6-, 10-, or 15-MV X-rays on a linear accelerator (Varian Medical Systems, Palo Alto, CA, USA) [22,23].
2.5. Radiologic Response Assessment
Radiologic responses were assessed every 4–6 weeks using dynamic CT or MRI according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST) guidelines [24]. Responses were classified as objective response (complete response [CR] or partial response [PR]) or non-regression (stable disease [SD] or progressive disease [PD]) [25]. The best overall response observed during treatment was recorded as the final response [26].
2.6. Evaluation of Adverse Events
Major adverse events following Atezo–Bev or locoregional therapy were evaluated according to the SIR reporting standards [20]. Adverse events were considered treatment-related if they occurred during or within 90 days after the end of treatment and were deemed by the treating physician to be potentially attributable to the administered agent or procedure. The SIR defines major adverse events as those requiring additional treatment, prolonged hospitalization, increased level of care, substantial morbidity, or resulting in death (SIR classifications grade 3–5).
2.7. Definitions and Data Analysis
Comparisons between the two treatment groups were performed using the independent t-test for continuous variables and the χ^2^ test for categorical variables. PFS and OS were calculated using the Kaplan–Meier method and compared using log-rank tests. PFS was defined as the interval from treatment initiation to tumor progression or death from any cause. OS was defined as the interval from initial treatment to death from any cause.
Survival data were censored when patients underwent surgical resection or liver transplantation after receiving Atezo–Bev or locoregional therapy, who achieved successful tumor downstaging following the initial treatment, making them eligible for curative therapy despite initial MVI, as these interventions could substantially alter outcomes. Timepoint-specific Kaplan–Meier estimates are provided in Table S1.
2.8. Propensity Score Weighting
To minimize confounding by indication between treatment groups, inverse probability of treatment weighting (IPTW) was applied. Propensity scores—representing the probability of receiving Atezo–Bev—were estimated using multivariable logistic regression incorporating clinically relevant covariates: age, etiology of liver disease, Child–Pugh class, MVI, extrahepatic metastasis, maximum tumor size, tumor multiplicity, and serum alpha-fetoprotein (≥400 ng/mL).
Stabilized weights were computed and truncated to reduce the influence of extreme 10.8 differences, with <0.10 indicating adequate balance. Time-to-event outcomes were analyzed using IPTW-weighted Cox proportional hazards models, and hazard ratios (HRs) with 95% confidence intervals (CIs) were reported.
All tests were two-sided, with statistical significance set at p < 0.05. Analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA) and R version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. Patient Characteristics
Table 1 presents the baseline demographic and clinical characteristics of both groups. All patients had radiologically confirmed MVI on contrast-enhanced CT or MRI and were therefore classified as BCLC stage C according to the 2022 BCLC guidelines. The median size of the largest tumor was 10 cm (interquartile range [IQR], 7–14 cm). Most patients in both groups were male and had chronic hepatitis B virus infection. No significant differences were observed between the groups regarding age, sex, etiology, Child–Pugh class, tumor burden (maximum tumor size and tumor number), elevated serum alpha-fetoprotein levels, tumor type (nodular or infiltrative), or extent of vascular invasion. The presence of a numerical imbalance in the most prognostically adverse factor, Main PV or IVC invasion (Atezo–Bev: 56.0% vs. LRT: 62.3%; p = 0.17), a clinically critical variable, was specifically addressed by the IPTW adjustment, which achieved adequate covariate balance for this factor (ASD < 0.1). In addition, significant differences were noted in ECOG performance status (p = 0.001), presence of varices (p < 0.001), and extrahepatic metastasis (p = 0.003). After IPTW adjustment, covariate balance was achieved, with all absolute standardized mean differences < 0.1.
3.2. OS and PFS Analyses
By the end of follow-up, 146 patients (76%) in the Atezo–Bev group and 261 (92%) in the locoregional therapy group had died. No patients in the Atezo–Bev group and 18 patients in the locoregional therapy group were censored at the time of surgical resection or liver transplantation.
The OS rates at 6 months and at 1, 2, 3, and 4 years were 68%, 44%, 21%, 15%, and 15%, respectively, in the Atezo–Bev group, and 70%, 45%, 19%, 12%, and 8%, respectively, in the locoregional therapy group. Median OS did not differ significantly between the Atezo–Bev group (9.3 months) and the locoregional therapy group (10.8 months) (p = 0.89) (Figure 1a).
During follow-up, 160 patients (84%) in the Atezo–Bev group and 265 (93%) in the locoregional therapy group experienced disease progression or death. The PFS rates at 6 months and at 1, 2, 3, and 4 years were 50%, 29%, 15%, 10%, and 10%, respectively, for Atezo–Bev, and 40%, 16%, 6%, 5%, and 3%, respectively, for locoregional therapy. Median PFS was significantly longer with Atezo–Bev (6.0 months) than with locoregional therapy (4.1 months; p < 0.001) (Figure 1b).
After IPTW, the OS difference remained non-significant (HR 0.95; 95% CI 0.76–1.19; p = 0.635) (Figure 2a), whereas PFS consistently favored Atezo–Bev (HR 0.64; 95% CI 0.52–0.79; p < 0.001) (Figure 2b) (Table 2).
3.3. Subgroup Analyses
In prespecified subgroup analyses, the treatment effect on 3-year OS (Figure 3) was consistent with the primary analysis. Stratification by age, etiology of liver disease, Child–Pugh class, MVI, extrahepatic metastasis, maximum tumor size, and tumor multiplicity produced HRs clustering around unity, with no subgroup-specific differences. These findings were similar in both unadjusted and IPTW-weighted models, reinforcing the robustness of the null OS result.
Conversely, in the 3-year PFS analysis (Figure 4), Atezo–Bev demonstrated a consistent advantage over locoregional therapy across subgroups. Point estimates favored Atezo–Bev-weighted result. Unadjusted analyses showed similar trends, indicating that the PFS benefit was broadly applicable rather than confined to a specific subgroup.
3.4. Radiologic Response After Treatment
During follow-up, 16 patients (8%) in the Atezo–Bev group achieved CR, 70 (37%) achieved PR, 55 (29%) showed PD, and 50 (26%) had SD. In the locoregional therapy group, 43 (15%) and 94 (33%) achieved CR and PR, respectively, while 81 (28%) showed PD and 66 (23%) had SD. The objective tumor response rate (CR or PR) did not differ significantly between the Atezo–Bev and locoregional therapy groups (45% vs. 48%) (p = 0.49) (Table 3). After IPTW adjustment, the incidence of objective tumor response remained similar (48% vs. 48%, p = 0.96).
3.5. Major Adverse Events
Major adverse events occurred in 21 (11%) of the 191 patients receiving Atezo–Bev and in 32 (11%) of the 284 patients receiving locoregional therapy (p = 0.93) (Table 3). In the Atezo–Bev group, major adverse events included proteinuria (n = 4), bleeding (n = 4), drug-related hepatitis (n = 3), skin rash (n = 3), drug-related pneumonitis (n = 2), severe diarrhea (n = 2), drug-related pancreatitis (n = 1), drug-induced adrenal insufficiency (n = 1), and toxic epidermal necrolysis (n = 1). In the locoregional therapy group, adverse events included acute kidney injury (n = 9), hepatic failure (n = 6), ischemic cholangiopathy with biloma (n = 5), liver abscess (n = 3), cisplatin-related allergic reaction (n = 3), cisplatin-induced neuropathy (n = 2), tumor lysis syndrome (n = 1), spinal cord infarction (n = 1), pneumonia (n = 1), and RT-related colitis (n = 1). After IPTW adjustment, the incidence of major adverse events remained comparable between the groups (11.4% vs. 11.4%; p = 0.99).
4. Discussion
To our knowledge, this is the first propensity score–weighted comparative analysis of Atezo–Bev versus locoregional therapy in patients with HCC and MVI. PFS was significantly longer with Atezo–Bev, whereas OS was comparable between groups. These findings were reproduced in inverse probability weighting analyses, underscoring robustness against selection bias. Major adverse events occurred at similar frequencies for both treatment strategies according to SIR criteria, before and after IPTW adjustment.
Although current guidelines recommend Atezo–Bev as the first-line regimen for advanced HCC [4,18], real-world management remains heterogeneous, particularly among patients with MVI, in whom locoregional therapy continues to be used in selected candidates [27,28]. In this study, Atezo–Bev yielded longer PFS than locoregional therapy, while OS did not differ significantly. The observed PFS benefit likely reflects improved disease control during active therapy, whereas OS convergence may result from subsequent treatments and post-progression crossover, which often obscure survival differences between regimens. Moreover, competing risks and extended post-progression survival can reduce the sensitivity of OS to on-treatment effects within a limited follow-up period [6,13,29,30]. In addition, post-progression and crossover treatments were heterogeneous and not recorded in sufficient detail to permit formal adjustment. This incomplete characterization of subsequent therapies likely contributed to OS convergence between groups and may partly explain the divergence between PFS and OS observed in the present study. Although the absolute median PFS gain of 1.9 months may appear modest, in patients with advanced HCC with MVI, this corresponds to a substantial relative reduction in the risk of progression or death and was generally accompanied by delayed clinical deterioration, including worsening liver function and performance status. Thus, we interpret the PFS benefit of Atezo–Bev as reflecting improved on-treatment disease control rather than a purely radiographic delay. Nevertheless, the lack of a demonstrable OS advantage indicates that the ultimate clinical impact of this PFS prolongation is attenuated by complex post-progression management and era-related factors.
Therefore, PFS may serve as a more responsive indicator of sustained disease control. The consistent PFS advantage with Atezo–Bev represents a clinically meaningful benefit, even in the absence of OS separation. This interpretation aligns with prior evidence showing weaker correlations between progression-based endpoints and OS in modern multi-line treatment settings, as well as randomized data confirming the disease-control capacity of Atezo–Bev [5,8]. Nonetheless, the lack of a detectable OS advantage indicates that the clinical impact of Atezo–Bev should be interpreted with caution. In this context, the PFS benefit is best viewed as enhanced on-treatment disease control, potentially translating into delayed symptomatic progression, prolonged maintenance of liver function, and more opportunities for subsequent therapies rather than as evidence of a clearly superior survival strategy. Thus, Atezo–Bev should be regarded as one of several viable first-line options, with locoregional therapy remaining an important alternative in appropriately selected patients. The comparable OS result also suggests that the locoregional therapy provided a robust survival benefit in this selected high-risk population. This observation aligns with existing regional data supporting the efficacy of TACE + RT combinations, which may effectively downstage or control local disease, thereby providing a durable OS foundation that is not easily surpassed by systemic therapy alone. Furthermore, the aggressive tumor biology inherently linked to macrovascular invasion represents a major confounding factor. This inherent aggressiveness may significantly limit the long-term survival window, causing OS convergence despite initial superior disease control achieved with Atezo–Bev.
Lee et al. reported superior PFS and OS with Atezo–Bev compared with TACE + RT in patients with PVTT without extrahepatic metastasis [16]. The modest discrepancies between their findings and the present results may reflect this study’s inclusion of a broader and more adverse disease spectrum, encompassing vascular invasion beyond the portal vein, such as hepatic venous and inferior vena caval involvement, and cases with multiple vascular territories affected [31,32]. Another contributing factor may be differences in intra-arterial chemotherapy protocols. In the current cohort, cisplatin was predominantly used, with limited application of doxorubicin. Cisplatin acts as a radiosensitizer by inhibiting DNA-dependent protein kinase–mediated nonhomologous end joining, thereby enhancing radiation-induced cytotoxicity, and has long served as a concurrent agent in definitive chemoradiation across tumor types [33,34]. These protocol-level variations may influence radiosensitization and intrahepatic cytoreduction, altering synergy with RT and potentially affecting OS. While the findings of Lee et al. provide important context, both their study and ours have inherent limitations, and therefore any cross-study comparison should be interpreted with caution.
The rate of major adverse events was 11.0% with Atezo–Bev and 11.3% with locoregional therapy, indicating comparable safety (p = 0.93). These rates align with published data reporting major adverse events in approximately 3–10% of patients receiving Atezo–Bev and 2–12% after locoregional therapy [6,7,8,14,35]. Given the similar safety profiles, locoregional therapy may remain a viable option in selected patients with HCC and MVI, particularly before systemic therapy initiation [18,36]. Moreover, strategically combining modalities may provide synergistic or additive disease-control benefits in appropriately selected candidates [14,34].
In the prespecified subgroup analyses, the treatment effect on OS was broadly consistent across clinical strata. HRs for age, etiology, liver function, tumor burden, and vascular invasion centered near unity, with substantial overlap of CIs, indicating similar survival between treatment strategies across patient groups. In contrast, for PFS, Atezo–Bev showed a reproducible advantage across nearly all subgroups. Most point estimates fell to the left of unity on the forest plot, suggesting a reduced risk of progression with Atezo–Bev. The direction and magnitude of benefit closely matched the overall treatment effect. Although CIs were wider in smaller subgroups, this reflected limited sample size rather than true heterogeneity. Collectively, the forest plots demonstrate that disease control with Atezo–Bev was consistently superior, while long-term survival remained comparable—reflecting both the biological activity of Atezo–Bev and the mitigating impact of effective locoregional therapy on mortality.
To improve outcomes beyond those achieved with Atezo–Bev in patients with HCC and MVI, ongoing research is exploring alternative strategies, particularly TARE. Observational studies comparing TARE with Atezo–Bev monotherapy have shown similar efficacy in some contexts. However, emerging analyses in PVTT suggest that, with optimized patient selection and dosimetry, TARE may outperform tyrosine kinase inhibitors and warrants direct comparison with Atezo–Bev in contemporary trials [37,38,39,40,41]. Kim et al. [38] proposed that earlier studies were limited by suboptimal selection—such as inclusion of main-trunk PVTT—and nonpersonalized, low-dose delivery. They advocated individualized high-dose TARE restricted to segmental or lobar portal vein involvement.
This study has some limitations. First, its retrospective design introduces potential selection bias and residual confounding despite statistical adjustment. To mitigate these risks, IPTW was applied, and balance diagnostics confirmed improved comparability of key baseline covariates between groups. Second, the comparison was partly historical, as Atezo–Bev was established as the first-line standard for advanced HCC only in 2020 [6,7,42]. Consequently, we acknowledge the inherent limitation that IPTW cannot fully adjust for unmeasured, time-varying confounders such as calendar-time effects, differences in follow-up, advances in supportive care or imaging, and critically, improvements in post-progression systemic treatments over the study period. These factors may have specifically influenced the survival outcome. Third, the locoregional therapy cohort was heterogeneous, including TACE alone and TACE combined with external-beam RT, with variations in intra-arterial chemotherapy and radiation delivery. This variability limits the ability to attribute observed effects to specific components of locoregional therapy and precludes detailed mechanistic interpretation of whether intra-arterial chemotherapy, embolization, radiotherapy, or their interaction primarily drives the observed outcomes. Accordingly, our findings should not be overinterpreted as comparative evidence for or against any specific TACE or TACE + RT protocol. Fourth, our cohort predominantly comprised patients with advanced disease characterized by extensive and heterogeneous MVI, including hepatic vein and inferior vena cava involvement, and frequent extrahepatic metastases. As a result, the external validity of our findings is limited, and they should not be directly extrapolated to more selected or earlier-stage patients with less extensive vascular involvement. Furthermore, we did not systematically capture detailed patterns of progression or time-to-response beyond standard mRECIST assessments in this retrospective cohort. As a result, we cannot fully delineate whether the PFS advantage of Atezo–Bev arose primarily from more durable intrahepatic control, delayed extrahepatic spread, or a reduction in early progression events. Future prospective multicenter randomized trials using standardized locoregional therapy protocols, predefined sequencing of systemic and locoregional modalities, and prespecified stratification by vascular invasion subtype and liver function, together with liver function preserving endpoints and optimized dosimetry, are needed to confirm these findings and to refine the optimal integration of Atezo–Bev and locoregional strategies.
5. Conclusions
In this IPTW-weighted analysis, Atezo–Bev demonstrated a clinically meaningful advantage in on-treatment disease control compared with locoregional therapy in patients with HCC and MVI. Nonetheless, locoregional therapy remains a relevant component of multidisciplinary care and may be incorporated into a staged treatment plan alongside Atezo–Bev for appropriately selected candidates. However, its precise role as a first-line option relative to Atezo–Bev remains to be defined and will ultimately need to be established in prospective randomized trials directly comparing systemic and locoregional strategies in well-stratified cohorts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H. Ferlay J. Siegel R.L. Laversanne M. Soerjomataram I. Jemal A. Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J. Clin.20217120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Villanueva A. Hepatocellular Carcinoma N. Engl. J. Med.20193801450146210.1056/NEJ Mra 171326330970190 · doi ↗ · pubmed ↗
- 3Vogel A. Rimassa L. Sun H.C. Abou-Alfa G.K. El-Khoueiry A. Pinato D.J. Sanchez Alvarez J. Daigl M. Orfanos P. Leibfried M. Comparative Efficacy of Atezolizumab plus Bevacizumab and Other Treatment Options for Patients with Unresectable Hepatocellular Carcinoma: A Network Meta-Analysis Liver Cancer 20211024024810.1159/00051530234239810 PMC 8237801 · doi ↗ · pubmed ↗
- 4Reig M. Forner A. Rimola J. Ferrer-Fàbrega J. Burrel M. Garcia-CriadoÁ. Kelley R.K. Galle P.R. Mazzaferro V. Salem R. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update J. Hepatol.20227668169310.1016/j.jhep.2021.11.01834801630 PMC 8866082 · doi ↗ · pubmed ↗
- 5Heimbach J.K. Kulik L.M. Finn R.S. Sirlin C.B. Abecassis M.M. Roberts L.R. Zhu A.X. Murad M.H. Marrero J.A. AASLD guidelines for the treatment of hepatocellular carcinoma Hepatology 20186735838010.1002/hep.2908628130846 · doi ↗ · pubmed ↗
- 6Finn R.S. Qin S. Ikeda M. Galle P.R. Ducreux M. Kim T.Y. Kudo M. Breder V. Merle P. Kaseb A.O. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma N. Engl. J. Med.20203821894190510.1056/NEJ Moa 191574532402160 · doi ↗ · pubmed ↗
- 7Kudo M. Finn R.S. Galle P.R. Zhu A.X. Ducreux M. Cheng A.L. Ikeda M. Tsuchiya K. Aoki K.I. Jia J. I Mbrave 150: Efficacy and Safety of Atezolizumab plus Bevacizumab versus Sorafenib in Patients with Barcelona Clinic Liver Cancer Stage B Unresectable Hepatocellular Carcinoma: An Exploratory Analysis of the Phase III Study Liver Cancer 20231223825010.1159/00052827237767068 PMC 10521324 · doi ↗ · pubmed ↗
- 8Cheng A.L. Qin S. Ikeda M. Galle P.R. Ducreux M. Kim T.Y. Lim H.Y. Kudo M. Breder V. Merle P. Updated efficacy and safety data from I Mbrave 150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma J. Hepatol.20227686287310.1016/j.jhep.2021.11.03034902530 · doi ↗ · pubmed ↗