Stool- and Blood-Associated Colorectal Cancer Biomarkers: A Systematic Review
Pumelela Hallom, Pragalathan Naidoo, Sibusiso Senzani, Sayed S. Kader, Zilungile L. Mkhize-Kwitshana

TL;DR
This study reviews non-invasive blood and stool biomarkers for early detection of colorectal cancer, aiming to improve accessibility and affordability of screening.
Contribution
The paper systematically evaluates the diagnostic potential of multi-marker panels for non-invasive colorectal cancer screening.
Findings
DNA methylation markers like SDC2 and SHOX2 achieved 91.35% stool sensitivity for CRC detection.
MicroRNA panels showed over 96% sensitivity and above 75% specificity for diagnosing colorectal cancer.
Multi-marker panels combining DNA methylation and microRNAs offer high diagnostic accuracy and scalability.
Abstract
Colorectal cancer is one of the most common and deadly cancers worldwide, but many people are diagnosed too late because current screening tests are expensive, invasive, or not easily available. Early detection greatly increases the chances of successful treatment. This research aims to find simple, accurate, and non-invasive ways to detect colorectal cancer using biological markers found in blood and stool. These markers can reveal early changes in the body that happen before cancer develops. By reviewing the most promising blood and stool markers, this study highlights potential tools that could make screening easier and more accessible for everyone. The findings may guide future research toward developing affordable tests that can detect colorectal cancer earlier, reduce deaths, and improve global health outcomes. Background/Objectives: Colorectal cancer (CRC) is a major contributor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
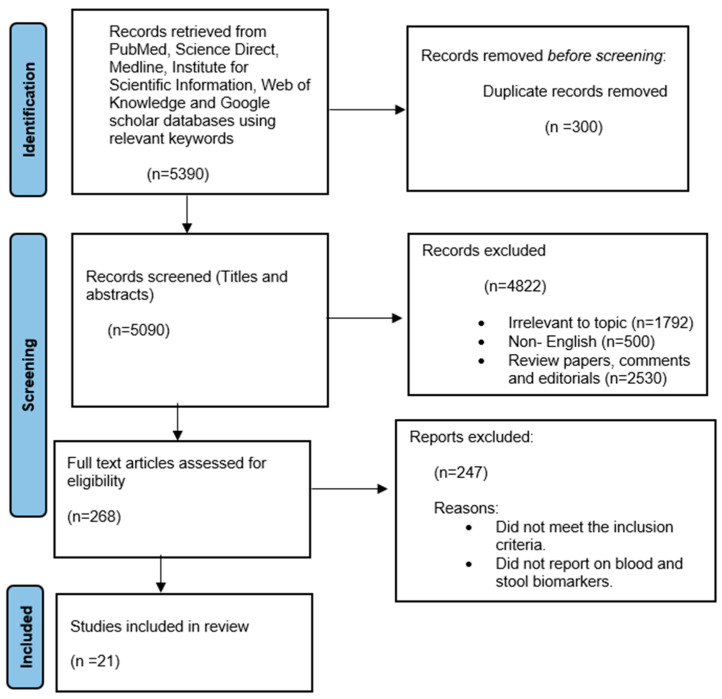 Figure 1
Figure 1- —South African Medical Research Council (SAMRC)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Screening and Detection · Ferroptosis and cancer prognosis · Cancer Cells and Metastasis
1. Introduction
Colorectal cancer is a significant global health burden, ranking as the third most diagnosed cancer and the second leading cause of cancer mortality [1]. It accounts for approximately 10.2% of new cancer cases and 9.2% of cancer-related deaths annually [1]. Early-stage CRC is frequently asymptomatic, leading to diagnosis at advanced stages when treatment efficacy declines. The 5-year survival rate exceeds 90% for stage I CRC but drops to 11–15% for stage IV disease [2,3], underscoring the critical importance of early detection and timely intervention.
Current CRC detection relies primarily on endoscopic techniques (colonoscopy, sigmoidoscopy), imaging modalities such as computed tomography (CT) colonography, and non-invasive fecal tests, including the guaiac-based fecal occult blood test (gFOBT) and fecal immunochemical test (FIT) [4,5,6]. While colonoscopy is highly sensitive and allows for both diagnosis and removal of precancerous lesions, it is invasive, costly, and requires bowel preparation, which may reduce patient compliance [5,6]. CT colonography provides a non-invasive imaging alternative, yet its availability is limited in many healthcare settings. Fecal-based tests like FIT are convenient and non-invasive but exhibit limited sensitivity, particularly for detecting precancerous lesions (27–29%) and right-sided tumors (65.8–75%) [7,8,9,10,11,12]. Collectively, these limitations highlight the need for more accurate, accessible, and patient-friendly diagnostic approaches.
To address these challenges, attention has increasingly turned to molecular biomarkers detectable in stool or blood, which reflect the genetic and epigenetic alterations that occur during CRC development [13,14,15,16,17,18,19,20,21,22,23,24,25]. These biomarkers include DNA methylation markers, microRNAs (miRNAs), tumor suppressor genes, and inflammatory proteins [16,17,18,19,20,21,22,23]. DNA methylation, an epigenetic modification associated with early tumorigenesis, can be detected in exfoliated colonocytes in stool, providing a potential non-invasive avenue for early CRC detection. Stool-based DNA methylation markers such as Tissue Factor Pathway Inhibitor 2 (TFPI2), VIM, SFRP2, NDRG4, BMP3, and SDC2 have shown promising diagnostic performance in several studies [19,20,21,22]. Circulating miRNAs, including miR-21 and miR-223, are stable in blood and represent another non-invasive biomarker class, capable of reflecting tumor biology and disease progression [22,23]. The identification of effective biomarkers for early CRC detection or monitoring is important because it could enable the detection of precancerous adenomas, which are fully amenable to endoscopic removal, a critical step in preventing the development of invasive and metastatic colorectal cancer [24,25]. This systematic review aims to identify, summarize, and evaluate stool- and blood-based biomarkers associated with CRC, focusing on those with the highest potential for non-invasive early detection.
2. Materials and Methods
A systematic literature search was conducted to collect data regarding biomarkers in stool and blood samples that might be promising for early detection of CRC. A narrative approach was followed to review relevant and available data on this topic. This systematic review has been registered under International Prospective Register of Systematic Review (PROSPERO) with reference ID: CRD42024572827.
2.1. Literature Search Strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to analyze and report relevant data in this systematic review. A systematic literature search was performed in PubMed, ScienceDirect, Medline, Institute for Scientific Information (ISI) Web of Knowledge, and Google Scholar databases using the following search keywords: ‘Stool/fecal/faecal biomarkers’, ‘Blood biomarkers’, colorectal cancer/CRC/colon cancer/rectal cancer/intestinal cancer’, ‘Stool biomarker and colorectal cancer or CRC’, ‘Blood biomarkers and colorectal cancer or CRC’. All globally published studies in the English language between January 2000 and September 2025 were included in this study.
2.2. Study Selection, Quality of Studies, and Data Extraction
The selection of appropriate literature for this study followed a structured process. Initially, titles, abstracts, and full texts were reviewed based on predefined inclusion and exclusion criteria by the primary author (P.H.). The eligibility of the selected literature was subsequently verified and cross-checked for discrepancies and duplicates by three co-authors (P.N., S.S., and Z.L.M.K.). The quality of the extracted data was categorized into four levels: high, moderate, low, and very low quality, as evaluated using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach [26,27].
Data were extracted from the eligible studies in a pre-defined form, including the first author’s name and publication year, sample population, specimen type, detection method, and diagnostic performance characteristics (sensitivity (%) and specificity (%) of biomarkers in CRC. The studies were qualified for eligibility according to pre-specified inclusion criteria.
Upon searching the above-mentioned databases with the relevant search criteria, a total of 5390 articles were found. Further evaluation revealed a total of 300 articles were duplicates, leaving a total of 5090 articles to be further assessed, considering the qualifying requirements. Articles that were not relevant were excluded (4822), and 268 full articles were assessed for eligibility. Ultimately, 21 of the 268 articles were selected based on stool- and blood-associated CRC biomarkers. Figure 1 shows a systematic flow diagram for selecting the articles selected for this systematic review according to initial identification, screening, eligibility, and final selection.
2.3. Inclusion Criteria
Literature reporting on stool and blood biomarkers for CRC.Literature published in English in all countries from January 2000 to September 2025.Cross-sectional studies, case–control studies, and cohort-appropriate studies.Literature published in the five databases mentioned above.
2.4. Exclusion Criteria
Literature published before January 2000.Articles not published in English.Comments, editorials, and Reviews. Articles not relevant to stool and blood biomarkers for diagnosis of CRC.
3. Results
An overview of the studies included in the systematic review is highlighted in Table 1. Detailed information on the specific biomarkers analyzed, sample sources, and molecular techniques employed for CRC detection is summarized in Table 2. CRC. Table 3 summarizes the optimal stool and serum biomarkers identified in the review, along with their reported sensitivity and specificity.
4. Discussion
This systematic review evaluated 21 publications examining stool- and blood-based biomarkers for colorectal cancer, highlighting their potential for early detection and non-invasive screening. The findings underscore the promise of DNA methylation markers, microRNAs, protein biomarkers, and microbial signatures, particularly when used in combination, to improve diagnostic accuracy.
4.1. DNA Methylation Biomarkers
DNA methylation remains one of the most studied approaches for non-invasive CRC detection. Markers such as Syndecan-2 (SDC2), Short Stature Homeobox 2 (SHOX2), N-Myc downstream-regulated gene 4 (NDRG4), Septin9 (SEPT9), and Branched-Chain Amino Acid Transaminase 1 (BCAT1) showed high sensitivity and specificity, especially in stool samples. For instance, SDC2 and SHOX2 methylation in stool achieved sensitivity of 91.35% and 89.5%, respectively, and 93.35% when combined, with specificities exceeding 85% [28]. Similarly, NDRG4 methylation in stool showed promising sensitivity (76.2%) and specificity (89.1%), though its performance in blood was lower, highlighting the superiority of stool-based detection for some methylation biomarkers [32,42]. Several studies demonstrated that methylation patterns of SEPT9, SDC2, and BCAT1 in plasma (circulating tumor DNA) could distinguish CRC from benign polyps with high diagnostic accuracy (AUC = 0.914) [33]. Multi-gene panels further improved performance, emphasizing the value of combining targets to capture tumor heterogeneity and enhance early detection [31,48]. These findings suggest that DNA methylation biomarkers, particularly when assessed in stool or as part of composite panels, can reliably detect early-stage CRC and even precancerous lesions [28,29,34].
4.2. MicroRNAs (miRNAs)
miRNAs have emerged as powerful biomarkers due to their stability in biofluids and their role in tumor biology. miR-21, miR-92a, miR-223, and miR-182 were consistently upregulated in CRC patients in both stool and plasma samples. Individually, these miRNAs showed good sensitivity and specificity, but combination analysis (e.g., miR-223 + miR-92a) yielded the highest diagnostic accuracy (sensitivity 96.8%, specificity 75%, AUC 0.907) [31,35,40]. The oncogenic role of miRNAs, particularly miR-223 and miR-182, also provides mechanistic insight; their upregulation promotes cell proliferation, invasion, and survival, linking biomarker detection to tumor biology [48,49,50]. These data suggest that miRNAs can serve as complementary diagnostic tools alongside DNA methylation, enhancing non-invasive CRC detection and potentially informing prognosis [30,39,46].
4.3. Protein Biomarkers
Protein-based biomarkers, including matrix metalloproteinases (MMP-2, MMP-9), Insulin-Like Growth Factor Binding Protein 2 (IGFBP2), Dickkopf-related protein 3 (DKK3), and Pyruvate Kinase M2 (PKM2), showed variable but clinically relevant performance. Fecal MMP-9 demonstrated sensitivity ranging from 72.2% to 89.3% and specificities from 91.2% to 95%, although some studies reported inconsistent results [51,52,53]. Serum levels of IGFBP2 and PKM2 were elevated in CRC patients, with a combined sensitivity and specificity of 73% and 95%, respectively [54]. These protein biomarkers reflect tumor-associated inflammation, extracellular matrix remodeling, and metabolic dysregulation, providing functional insights that complement genetic and epigenetic markers [21,55,56]. However, variability across studies highlights the need for standardized assays and validation in larger cohorts [52,53].
4.4. Microbial Biomarkers
The gut microbiome, particularly Fusobacterium nucleatum (F. nucleatum), has emerged as a promising CRC biomarker. Significantly higher levels of F. nucleatum were observed in CRC tissues and stool, and combining microbial detection with clinical parameters (e.g., fecal occult blood, CEA, CA19-9) improved diagnostic performance (AUC = 0.87) [38,45]. These findings suggest that microbial biomarkers can enhance non-invasive CRC detection when integrated into multi-parameter screening strategies.
4.5. Multi-Marker and Combination Panels
Several studies emphasized the superior performance of multi-marker panels over single biomarkers. For example, combining DNA methylation markers such as Secreted frizzled-related protein 2 and Wnt inhibitory factor 1 (SFRP2 + WIF-1), miRNAs (miR-21 + miR-29a + miR-92a), or ctDNA methylation with protein markers and fecal tests improved both sensitivity and specificity [31,39,41,48]. This approach addresses the inherent heterogeneity of CRC and increases the likelihood of detecting early-stage and precancerous lesions.
4.6. Limitations and Future Directions
A notable limitation of the current evidence is that many studies were conducted on small or ethnically homogeneous cohorts, which may restrict the generalizability of the findings. The diagnostic performance of several stool- and blood-based biomarkers has not been validated across diverse populations, and differences in genetic background, environmental exposures, and lifestyle factors may influence biomarker expression and methylation patterns.
Many studies were also limited by small sample sizes, single-center designs, and methodological variability (e.g., assay type, sample handling, cut-offs), which introduce potential bias and may affect reported sensitivity and specificity. Potential publication bias could further overestimate the diagnostic performance of some biomarkers. In addition, there is significant methodological heterogeneity among studies, including differences in DNA extraction kits, PCR protocols, methylation detection assays, and sample processing methods, which complicate comparisons and reduce reproducibility, representing a significant barrier to clinical translation.
While high specificity (>90%) was frequently reported, most studies employed case–control designs with healthy participants as controls. This may overestimate real-world specificity, as it does not fully account for common gastrointestinal conditions such as inflammatory bowel disease, diverticulitis, or benign polyps, which are important for clinical decision-making. Future studies should therefore include disease control groups with common benign gastrointestinal pathologies to provide a more realistic assessment of diagnostic specificity in a true screening population.
A further important limitation, which precluded quantitative meta-analysis, is the extensive heterogeneity observed across the studies included. This heterogeneity is clinical (diverse populations, disease stages), methodological (varying assay protocols, sample processing techniques, and positivity thresholds), and statistical (inconsistent reporting of essential data for pooling). The biomarker field for CRC is also characterized by rapid evolution, with many studies investigating novel, distinct targets or unique multi-marker panels. Consequently, there were insufficient homogeneous studies for any single biomarker to perform a statistically robust and clinically meaningful meta-analysis. Attempting to pool data under these circumstances would violate the core assumptions of meta-analytic models and generate unreliable summary estimates. Therefore, this review provides a comprehensive qualitative and comparative synthesis. We emphasize that the reported sensitivities and specificities must be interpreted within the specific context of each primary study.
Taken together, these factors suggest that while some biomarkers show promising results, the overall certainty of the evidence is limited, and conclusions should be interpreted with caution. There is an urgent need for standardized, universally accepted protocols, as well as large, multi-ethnic, population-based validation studies, to ensure the reliability, reproducibility, and clinical applicability of stool- and blood-based CRC biomarkers. Future research should prioritize standardized protocols and comprehensive data reporting to facilitate definitive quantitative synthesis.
5. Conclusions
This systematic review highlights the potential of stool- and blood-based biomarkers, including DNA methylation markers, microRNAs, protein biomarkers, and microbial signatures, for non-invasive early detection of colorectal cancer. While several biomarkers demonstrated high sensitivity and specificity, the overall certainty of evidence is limited due to small, ethnically homogeneous cohorts; methodological heterogeneity; and the reliance on healthy controls, which may overestimate real-world diagnostic performance. The findings underscore the critical need for standardized protocols, multi-marker panels, and validation in large, multi-ethnic, population-based studies, including participants with other gastrointestinal conditions, to confirm clinical utility. These efforts are essential to translate promising biomarkers into reliable, broadly applicable screening tools for early CRC detection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Ferlay J. Soerjomataram I. Siegel R.L. Torre L.A. Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.20186839442410.3322/caac.2149230207593 · doi ↗ · pubmed ↗
- 2Brenner H. Kloor M. Pox c P. colorectal cancer Lancet 20143831490150210.1016/S 0140-6736(13)61649-924225001 · doi ↗ · pubmed ↗
- 3Miller K.D. Nogueira L. Devasia T. Mariotto A.B. Yabroff K.R. Jemal A. Kramer J. Siegel R.L. Cancer treatment and survivorship statistics, 2022 CA Cancer J. Clin.20227240943610.3322/caac.2173135736631 · doi ↗ · pubmed ↗
- 4Kuipers E.J. Rösch T. Bretthauer M. Colorectal cancer screening—Optimizing current strategies and new directions Nat. Rev. Clin. Oncol.20131013014210.1038/nrclinonc.2013.1223381005 · doi ↗ · pubmed ↗
- 5Simon K. Colorectal cancer development and advances in screening Clin. Interv. Aging 20161196797610.2147/cia.s 10928527486317 PMC 4958365 · doi ↗ · pubmed ↗
- 6Loktionov A. Biomarkers for detecting colorectal cancer non-invasively: DNA, RNA or proteins?World J. Gastrointest. Oncol.20201212410.4251/wjgo.v 12.i 2.12432104546 PMC 7031146 · doi ↗ · pubmed ↗
- 7Morikawa T. Kato J. Yamaji Y. Wada R. Mitsushima T. Shiratori Y. A comparison of the immunochemical fecal occult blood test and total colonoscopy in the asymptomatic population Gastroenterology 200512942242810.1016/j.gastro.2005.05.05616083699 · doi ↗ · pubmed ↗
- 8de Wijkerslooth T.R. Stoop E.M. Bossuyt P.M. A Meijer G. van Ballegooijen M. van Roon A.H.C. Stegeman I. A Kraaijenhagen R. Fockens P. E van Leerdam M. Immunochemical fecal occult blood testing is equally sensitive for proximal and distal advanced neoplasia Off. J. Am. Coll. Gastroenterol. ACG 20121071570157810.1038/ajg.2012.24922850431 · doi ↗ · pubmed ↗