Utilization of insecticide-treated bed nets and key factors among households in resource-limited settings, Northwest Ethiopia
Abraham Teym, Tirsit Ketsela Zeleke, Mestet Yibeltal Shiferaw, Gete Berihun, Mengistu Abebe Messelu, Temesgen Aynew, Ayenew Sisay Gebeyew, Bayou Tilahun Assaye, Almaw Genet Yeshiwas, Chalachew Yenew

TL;DR
This study examines how often households in Northwest Ethiopia use insecticide-treated bed nets and identifies factors influencing their use.
Contribution
The study provides new insights into ITN utilization and associated factors in a resource-limited setting in Ethiopia.
Findings
Approximately 71.3% of households used insecticide-treated bed nets, below the WHO-recommended 80%.
Key factors influencing ITN use include being female, higher income, and receiving information about ITN use.
Households with illiterate members were less likely to use ITNs compared to others.
Abstract
Insecticide-treated mosquito nets (ITNs) act as an essential tool in malaria prevention by serving as a physical barrier against the disease. In sub-Saharan Africa, the use of ITNs remains a cornerstone in efforts to reduce malaria transmission. Despite their importance, there is limited evidence on ITN utilization and the factors influencing their use in Ethiopia. The objective of this study was to assess utilization of insecticidal treated bed nets and its key factors among Households in resource-limited settings, Northwest, Ethiopia, in 2024. A community-based cross-sectional study was carried out from January 30 to March, 2024. A total of 492 randomly selected Households were included. Data were acquired using a pre-tested structured questionnaire and an observational checklist. Binary logistic regression was initially used to select variables associated with the use of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
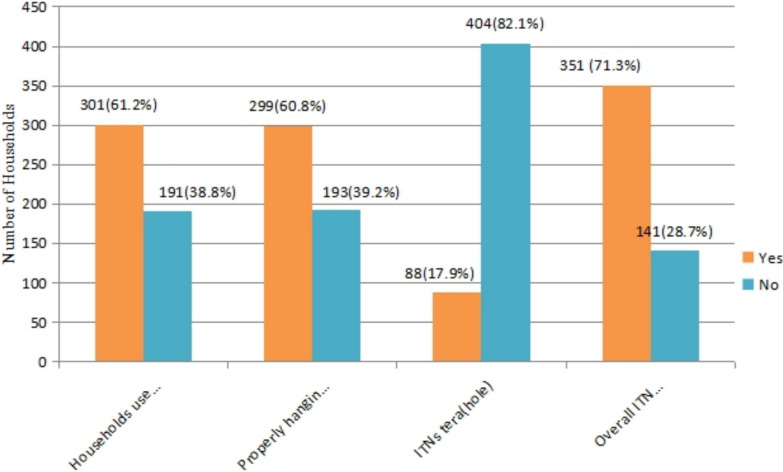 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMalaria Research and Control · Parasites and Host Interactions · Mosquito-borne diseases and control
Background
Insecticide-treated nets (ITNs) are designed to act as both a physical and chemical barrier against mosquitoes, offering a cost-effective approach to malaria prevention [1]. To maintain their efficacy, ITNs must be treated with insecticide regularly or replaced when necessary. Their use is particularly crucial in regions with high malaria transmission, as they are one of the most effective tools for controlling the disease [2–4]. Malaria remains a major public health problem, with almost half of the world's population at risk [5].
The World Health Organization (WHO) reported in 2020 that malaria remains a significant global health challenge, with an estimated 229 million cases recorded across 87 endemic countries. Tragically, nearly 409,000 deaths were attributed to malaria that year, the majority of which 67% occurred in children under five years old [6]. The WHO African Region bore the highest burden, accounting for approximately 94% of these cases, equating to 215 million infections [7, 8]. Malaria imposes a substantial burden on healthcare systems, particularly in sub-Saharan Africa. It is responsible for a significant proportion of healthcare utilization, contributing to 25–35% of outpatient consultations, 20–45% of hospital admissions, and 15–35% of hospital-related deaths [9]. This disease continues to strain the already limited healthcare resources in the region [10].
Malaria causes millions of cases and hundreds of deaths in Ethiopia every year [11]. Malaria is a significant public health issue in Ethiopia [12]. Annually, up to 6 million clinical cases have been recorded. However, the estimated number of clinical malaria cases ranges from 8 to 10 million [13]. Malaria has been cited as the leading cause of illness and mortality. Malaria accounts for 16.6% of outpatient visits, 15% of hospitalisations, and 28.9% of inpatient mortality [13]. Approximately three-quarters of Ethiopia's total territory is malarial, and an estimated 48 million people, 68% of the population, reside in malaria-risk areas [14, 15]. Regardless of the fact that numerous malaria prevention mechanisms exist, the WHO suggested the use of insecticide-treated bed nets (ITNs) as one of the measures to reduce the deleterious effects of malaria [16].
One of the most prevalent and cost-effective vector control strategies for malaria prevention is insecticide-treated bed nets [16–18]. It is treated with insecticidal chemicals and requires continued treatment, and ITNs are also effective in malaria prevention in high-endemic areas [3, 19]. As a result, the distribution and usage of ITNs are key interventions for malaria infection prevention control in underdeveloped countries, such as Ethiopia [16, 17].
The World Health Organization (WHO), through its 2015 Roll Back Malaria (RBM) initiatives, set ambitious targets to significantly reduce the global malaria burden. These goals included achieving a 75% reduction in malaria cases and minimizing malaria-related deaths, with a focus on ensuring universal coverage and proper utilization of insecticide-treated nets (ITNs) [20]. To support this aspect of malaria prevention, significant efforts and resources have been allocated by donors [21]. However, the proper utilization and coverage of insecticide-treated bed nets (ITNs) among priority and high-risk groups remain very low [22]. For instance, studies indicate that only 19% of these groups adequately use ITNs [23]. Several factors contribute to this low utilization, including discomfort, lack of experience in hanging nets, ineffective educational campaigns, and a scarcity of ITNs [24–26].
A study supported by the United States Agency for International Development (USAID), conducted through the Newmark Project in partnership with the Academy for Educational Development (AED), reported varying levels of ITN utilization the night before the survey. Findings revealed that 73% of households in the Oromia region and 60% in the Amhara region used ITNs [27]. Bibugn District, located in Northwest Ethiopia, has distinct topographical features, malaria transmission patterns, and socio-demographic characteristics that may uniquely influence the utilization of insecticide-treated bed nets (ITNs) [28]. Although several studies on ITN use have been conducted across Ethiopia, most have focused primarily on utilization rates, with limited attention given to the factors influencing usage, especially in context-specific settings like Bibugn. Therefore, this study aimed to assess ITN utilization and its associated factors among households in Bibugn District, providing locally relevant evidence to inform targeted malaria prevention strategies.
Methods
Study area and periods
The study was conducted in Bibugn district, North West Ethiopia; located 81 km from Debra Markos which is east Gojjam zone town 211 km from Bahirdar which is capital city of Amhara region and 381 km from Addis Ababa, the capital city of Ethiopia. According to 2007 census projection, The total population of the woreda was estimated to be 82,002, of which 40,190 are males and 41,812 are females [28].This study was conducted from January 30, up to March 30, 2024.
Study design
Community based cross-sectional study design was used.
Study population
All households living in the selected Kebeles of Bibugn district that owned at least one insecticide-treated net (ITN) were considered the study population. Households that had resided in the selected Kebeles for six months or more were included in the study. However, households were excluded if the respondent was severely or critically ill during the study period.
Sample size calculation and sampling procedure
The sample size for the survey was calculated using the formula for a single population proportion, with assumptions of a 95% confidence interval, 5% margin of error, and an estimated 73% of households using ITNs based on a prior study in Ethiopia [29]. With 95% confidence interval, the marginal error of 5% (0.05), design effect (1.5) and non-response rate 10%, the resulting calculation for a total sample size was 500 households.
A two-stage sampling technique was employed. In the first stage, 10 kebeles (2 urban and 8 rural) were randomly selected from a total of 20. In the second stage, households were allocated proportionally across the selected kebeles based on a total of 1,489 registered households. Systematic random sampling was then applied, using a sampling interval of 3 (1489/500 ≈ 3). The first household was selected by lottery, and subsequent households were identified at regular intervals. For households where no eligible respondent was available, up to three revisits were conducted before being classified as non-respondents, confirmed through neighbors.
Variables
Dependent variables: ITN utilization among Households.
Independent variables: Socio-demographic characteristics of Households (such as Age, educational status. Marital status, Religion, Occupation, monthly income, residence, and family size), Health information (Health worker, media), Personal factors such as (knowledge, practice), Housing condition such as (number of room, number of bed).
Data collection tool
An interviewer-administered questionnaire was used to collect data. The questionnaire included sections on sociodemographic characteristics, knowledge, and health-related information relevant to insecticide-treated net (ITN) use. Eligible respondents were adult household members, preferably the household head or spouse, who had resided in the household for at least six months and were knowledgeable about household practices related to ITN ownership and use. These individuals were selected to ensure they could provide reliable and accurate information on behalf of the household.
Data collection was conducted by eight trained data collectors and supervised by two field supervisors. Prior to data collection, all personnel participated in a one-day training session covering the study objectives, interview techniques, ethical considerations including confidentiality, and procedures for obtaining informed consent. Data collectors were selected based on their language proficiency, willingness to participate, and demonstrated professionalism. Data were collected using a standardized questionnaire format. To ensure accuracy and reliability, trained interviewers administered the tool and completed each questionnaire based on direct responses from the eligible respondents.
Data quality management
The questionnaire was developed in English, translated into Amharic, and back-translated to ensure accuracy and consistency. It was pretested on 5% of the sample in a non-selected area of Bibugn district to assess clarity, relevance, and flow. Data collectors and supervisors received one day of training on the study objectives, ethical considerations, and data collection procedures to ensure quality. During data collection, completed questionnaires were reviewed daily by data collectors, supervisors, and the principal investigator to check for completeness and internal consistency. After data entry, data cleaning was conducted to ensure accuracy and prepare the dataset for analysis.
Data processing and analysis
Data were entered, cleaned, and coded using EpiData version 3.1 and then exported to SPSS version 25 for analysis. Descriptive statistics were presented in text, tables, and graphs. Binary logistic regression was used to identify factors associated with ITN utilization. Variables with a p-value of less than 0.25 in bivariable analysis were considered for inclusion in the multivariable logistic regression model. The 0.25 threshold was selected to avoid excluding potentially important variables too early, as recommended in epidemiologic literature to minimize residual confounding. Final associations were considered statistically significant at a p-value less than 0.05 with 95% confidence intervals. Model fitness was assessed using the Hosmer–Lemeshow goodness-of-fit test (p = 0.56), indicating adequate model fit. The maximum likelihood ratio test was also used to check model assumptions.
Results
Sociodemographic characteristics of the respondents
A total of 492 households participated in the study, yielding a response rate of 98.40%. Among the respondents, 280 (56.91%) were male. The mean age of respondents was 31.4 years (SD ± 5.77). Most respondents, 4 (89.02%), were married, and 393 (79.88%) resided in rural areas. Regarding religion, 402 (81.70%) identified as Orthodox Christians. Educationally, 199 (40.45%) of the respondents were illiterate, and the primary occupation was farming, with 292 (59.35%) engaged in agricultural activities. The majority of households (243, 49.39%) had a family size of 1–3 members. The mean monthly income of the respondents was 3,273.48 Ethiopian Birr, with an SD of ± 2,457.81. Most households had fewer than two rooms (386, 78.46%) and fewer than two beds (437, 88.82%) (Table 1). Table 1. Socio-demographic characteristics of the respondents in Bibugn district, Northwest Ethiopia, 2024 (n = 492)CharacteristicsCategoriesFrequency(%)Sex of the respondentMale28056.91Female21243.09Age group18–248717.6825–4423046.7545–6416934.35> 6461.22ResidenceUrban9920.12Rural39379.88ReligionOrthodox40281.70Muslim7415.04Protestant162.90Marital statusMarried43889.02Single275.48Divorced193.86Widowed81.64Education statusCan’t read and write19940.45Can read and write (had not formal education)9519.30Elementary education12024.30Secondary education489.75College and above306.20OccupationFarmer29259.35House wife8918.09Merchant346.91Government employee5410.98Daily labor173.45Others61.22Family size1–324349.394–521944.51> 5306.10Monthly income< 500459.15500–10007715.65> 100037075.20Number of rooms< 238678.46> 310621.54Number of beds< 243788.82> 35511.18
Magnitude of insecticide treated bed net utilization and distribution
In the study area, 489 (99.39%) households received ITNs, with 50.61% owning one. Health workers provided ITN information to 63.61% of respondents, and 301 (61.18%) households used ITNs the previous night. Properly mounted ITNs were observed in 299 (60.77%) households. Most ITNs (67.48%) were under three years old. While 214 (43.49%) households had two beds, 50.61% had only one ITN per bed (Table 2). Table 2ITN utilization and related condition in Bibugn district, Northwest Ethiopia, 2024CharacteristicsCategoriesFrequencyPercent (%)Received information about ITNs and its benefitsYes38377.84No10922.16From whom you received informationMedia5911.99Health worker31363.61NGOs91.83Others30.41Accesses to ITNsYes48999.39No30.61Households used ITN previous nightYes30161.18No19138.82ITN properly mounted over sleeping areaYes29960.77No19339.23ITN tear (hole)Yes8817.88No40482.12Number of beds or places of sleepOne21443.49Two24048.78Three & above387.73Number of bed nets observed in householdOne24950.61Two18236.99Three & above6112.40Number of beds (places) observed with bed netsOne30561.99Two15631.70Three & above316.31The age of ITNs present in the household< 3 years33267.483–5 years15731.91> 5 years30.61
Utilization of ITNs was defined as the use of at least one insecticide-treated net by any household member on the night preceding the survey. Based on this definition, 351 (71.3%) households reported ITN utilization. This indicates that the majority of households effectively used ITNs, demonstrating a relatively high level of adherence to recommended malaria prevention practices (Fig. 1).Fig. 1. Proportion of ITNs utilization among Households in Bibugn District, North west Ethiopia, 2024
Knowledge of Households about malaria and insecticide treated bed nets
About 473 (96.14%) respondents knew about malaria, and 318 (64.63%) of them identified mosquito bites as the cause of malaria transmission, while others mentioned alternative modes of transmission. Two hundred eighty-eight (58.54%) of the respondents were able to identify children under 5 years of age as the priority group for malaria prevention within households.
A total of 327 respondents (66.46%) reported using insecticide-treated nets (ITNs) as a priority measure for malaria prevention at the household level. Regarding malaria symptoms, chilliness was mentioned by 365 respondents (74.19%), fever by 256 (52.03%), headache by 137 (27.87%), vomiting by 45 (9.15%), and loss of appetite by 42 (7.80%). One respondent reported no knowledge of any symptoms.
Concerning respondents' knowledge about ITN prevention mechanisms, 293 (59.55%) reported that ITNs act as a physical barrier to prevent mosquito bites. Additionally, more than half of the respondents (70.12%) identified that ITNs should be used every night. The majority (90.04%) of respondents believed that ITN use does not pose any problems. Of the total participants, 34 respondents (7.2%) reported discomfort caused by heat when using ITNs (Table 3). Table 3. Knowledge of households about malaria and insecticide treated bed net in Bibugn district, Northwest Ethiopia, 2024 (n = 492)CharacteristicsCategoriesFrequencyPercent (%)Know malaria diseaseYes47396.14No193.86Transmission of malariaMosquito bite31864.63By flies214.27Due to water275.49Not known193.86Priority given for malaria prevention within the household< 5 children28858.54Pregnant women25752.23Adult132.64Old age153.05Malaria prevention mechanismChemical spray13026.42Draining stagnant water11623.58Environment management10421.14ITN utilization32766.46Not known173.45Symptom of malariaFever25652.03Headache13727.85Chills36574.19Loss of appetite428.53Vomiting459.15Not known91.83ITN mechanism of actionPhysical barriers29359.55Kills mosquito16733.49Not known193.86When to utilize ITNEvery night34570.12Sometimes387.72Seasonally8717.68Not known204.06Any problem if ITN utilizedYes499.96No44390.04List of problems if ITN utilizedNo comfort204.10Cause heat347.20Air hanger40.80Not known20.40
Of the total participants, 269 (54.67%) respondents had good knowledge about ITNs and malaria, while 223 (45.33%) had poor knowledge. Among the respondents with good knowledge, 209 (59.54%) properly utilized ITNs. In contrast, among those with poor knowledge, 142 (40.46%) properly utilized ITNs (Supplementary file 1).
Reasons for not using ITN by households
According to the response obtained from the respondents, old and worn out nets (12.81%), Lack of sufficient space to hang the net (8.73%), Suffocation/ too hot (4.24%), and not others (2.92%) were the reasons that were mentioned for not utilizing ITN (Supplementary file 2).
Factors associated with ITN utilization among households
Bivariate analysis showed that variables such as sex, age, residence, educational status, monthly income, access to information about ITNs and their benefits, and knowledge were associated with ITN utilization (p ≤ 0.25). These variables were included in the multivariable analysis. In the multivariable logistic regression model, sex, access to information, monthly income, and educational status remained significantly associated with household ITN utilization (p < 0.05). The results of the multivariable logistic regression analysis indicated that women were 1.54 times less likely to use ITNs compared to men (AOR = 1.538; 95% CI 1.157, 3.135). This study also revealed that households with information about ITNs and their benefits had a 1.3 fold higher likelihood of utilizing ITNs compared to those without such information (AOR = 1.310; 95% CI 1.125, 3.229). Additionally, households earning more than 1,000 Ethiopian Birr in monthly income had 1.37 times higher odds of utilizing ITNs compared to those earning less than 500 Ethiopian Birr (AOR = 1.372; 95% CI 1.038, 3.184). Furthermore, the study found that households in which the respondant was unable to read and write had a 76.3% lower likelihood of ITN utilization compared to those with a college-level education or higher (AOR = 0.223; 95% CI 0.026, 0.871) (Table 4). Table 4. Bivariable and multivariable analysis factors associated with ITN utilization in Bibugn district, Northwest Ethiopia, 2024 (n = 492)VariablesITN utilizationYesNoCOR (95%CI)AOR (95% CI)p valueSex of the respondent Male21367110.003 Female13874**1.704 (1.239, 3.613)****1.538 (1.157, 3.135)Age group 18–2466211.571 (0.263, 2.639)0.618 (0.278, 1.998)0.653 25–44175551.591 (1.104, 2.794)0.762 (0.364, 1.873)0.714 45–64106630.841 (0.396, 1.948)0.857 (0.389, 1.887)0.097 > 644211Residence Urban72271.089 (0.673, 3.108)1.179 (0.541, 2.798)0.543 Rural27911411Educational status Can’t read and write127720.057 (0.014, 0.581)****0.237 (0.026, 0.871)0.001 Able to read and write68270.387 (0.127, 1.24)0.583 (0.142, 1.891)0.182 Elementary education92280.505 (0.132, 0.952)0.633 (0.131, 1.362)0.215 Secondary education38100.584 (0.128, 2.112)0.785 (0.135, 1.993)0.411 College and above26411Monthly income < 50041360.342 (0.043, 0.649)****1.372 (1.038, 3.184)0.002 500–100026190.414 (0.162, 1.342)1.231 (0.594, 2.854)0.274 > 10002848611Having information about ITNs and its benefits Yes2711120.877 (0.428, 0.994)****1.310 (1.125, 3.229)**0.000 No802911Knowledge of the respondents Good209601.986 (1.1361, 3.145)1.178 (0.642, 1.681)0.543 Poor1428111Bold values indicate statistically significant results, meaning the association is unlikely to be due to chance (p 0.05)(p < 0.05) statistically significant
Discussion
This study was designed to assess the prevalence and associated factors influencing insecticide-treated net (ITN) utilization among households in Bibugn District, Northwest Ethiopia. In addition to identifying the associated factors, the study also aimed to examine the actual utilization of ITNs among the households. The findings indicated that 71.3% of households used ITNs the night before the data collection day. This result is consistent with findings from Ilu Galan District in the Oromia Region of Ethiopia, where 72.2% of households reported ITN utilization [30], Arbaminch town in southern Ethiopia (71%) [29], Alamata district in northern Ethiopia (73%) [10], Harari regional state, Ethiopia (73.3%) [31], Burkina Faso (70%) [32], and Nigeria (75.4%) [32]. This may be because all of the above studies, including the present one, were conducted in malaria-endemic areas, where the risk of infection might have compelled households to use ITNs out of fear of contracting malaria.
However, the finding of this study is higher than that of the 2016 Ethiopian Demographic and Health Survey (EDHS), which reported that only 16.6% of households utilized ITNs [33], Northern Ethiopia (58.4%) [34], Sodo zuria woreda Southern Ethiopia (56.89%) [35], Mesekan District, Gurage Zone, Southern Ethiopia (58.2%) [36], Dawo district, Southwest Shoa Zone, Oromia, Ethiopia (55.5%) [37], Asgede Tsimbla District, Northern Ethiopia (63.1%), at a tertiary hospital in Nigeria 43.7% [4, 38]. This discrepancy may be attributed to differences in study settings, periods, and awareness levels. The higher utilization rate in the present study could be due to intensified malaria prevention campaigns, better access to health information, increased availability and distribution of ITNs in recent years, or heightened perceived risk of malaria in the study area [39].
The finding of this study is less than the result obtained from a study conducted among settlers in southwest Ethiopia [40] which found 80% of households used a bed net the night before the study, Afar (79.1%) [41], and WHO recommendation of ITN utilization to be in Ethiopia (80%) [42]. The disparity between this study and that of southwest Ethiopia study might be explained by the time gap between this study and the southwest Ethiopia study during which ITN distribution took place before the study was conducted. Others reason for the discrepancy of the 2 studies might be due to differences in the sociodemographic and socio-economic profiles of the study populations [43].
In this study, sex, educational status, monthly income, and having information about ITNs and their benefits were found to be statistically significant predictors of household ITN utilization. According to the findings of this study, being female was identified as a predictor of ITN utilization. This finding is consistent with a study conducted at Addis Zemen Hospital in Northern Ethiopia [44], Raya Alamata districts of Ethiopia [10], Ilu Galan District, Oromia Region, Ethiopia [30], and Arbaminch, Ethiopia [29] that found that females were less likely to utilize ITN than males. This might be also due to sociocultural background in which men are given priority over women in Ethiopia [45]. Moreover, this study was conducted in rural areas where males were more educated than females that lead males to have more awareness about ITN utilization [30]. This result is inconsistent with a study conducted in in Kersa Woreda, Jimma Zone, Southwest Ethiopia [46], in 7 sub-Saharan African countries [47] that showed females were identified as more likely utilized ITNs than males. The reason for this disparity might be due to difference in study setting and socio-cultural back ground of the communities.
Households in which the respondant was unable to read and write were significantly less likely to utilize ITNs compared to those with a college-level education or higher. This finding underscores the critical role of education in promoting health-protective behaviors. It is consistent with the results of a study conducted at Addis Zemen Hospital in Northwest Ethiopia, which also highlighted lower ITN utilization among individuals with limited or no formal education [48] and Damot pulasa district, Southern Ethiopia [49]. This difference might be due to educated Households may know the consequences of malaria if they did not use ITNs. Another possible explanation might be due to the fact that educated population can easily read and understand the information regarding malaria prevention mechanisms including ITNs.
In this study, earning more than 1,000 Ethiopian Birr per month was positively associated with ITN utilization. Households with higher monthly income were more likely to use ITNs compared to those with lower income, possibly due to better access to health information, improved living conditions, and increased health awareness. This finding is consistent with a study conducted in Southwest Ethiopia, which also reported a positive relationship between household income and the utilization of ITNs [50] and Ilu Galan District, Oromia Region, Ethiopia [30] where households with higher wealth indexes were more likely to utilize ITN. This is because those households that have better income can afford ITNs and utilize than those with low monthly income. This result is inconsistent with a study conducted in Ghana [51]. This could be due to the reason that rich families may consider other prevention methods and this might have affected the LLIN utilization [52].
In this study, households that had received information about ITNs and their benefits were 1.3 times more likely to utilize ITNs compared to their counterparts. Access to information likely improved awareness of the importance of ITNs in preventing malaria, which in turn promoted their usage. This finding is consistent with a study conducted in Fogera, Northwest Ethiopia, where exposure to health education was also found to significantly influence ITN utilization [53], Mihrab Abaya Gamo Gofa [54], Gambelia [44], Awabel District [55], and Jawi Northwest Ethiopia [56]. This could be attributed to the fact that Households who had received health education about insecticide treated bed nets were better aware of the importance ITNs to prevent malaria [57].
Efforts to increase ITN use should ensure that education and awareness activities are inclusive and accessible to underserved groups, including low-literacy households, poorer families, and men. Messages must use local languages and culturally relevant approaches that reflect community realities. Segmenting audiences, monitoring progress, and adapting communication strategies are crucial for effective and sustainable behavior change. Addressing social and gender norms will further enhance the equity and impact of awareness efforts.
Strengths and limitation of study
A key strength of this study was the use of direct observation to validate ITN utilization, enhancing data accuracy. However, this study had some limitations. The use of logistic regression may have overestimated associations for common outcomes, as alternative models like modified Poisson regression were not feasible. Self-reporting and recall bias might also have affected responses. Moreover, the cross-sectional design limits causal inference and generalizability to all malaria-endemic areas.
Conclusion
In this study, the utilization of insecticide-treated bed nets (ITNs) among households was 71.3%, below the WHO recommendation of at least 80% [58] household coverage and use for effective malaria prevention. Sex, educational status, monthly income, and access to information about ITNs and their benefits were identified as significant predictors of utilization. Specifically, being male, having a college-level education or higher, earning a higher monthly income, and receiving health information were positively associated with ITN use. To achieve and maintain the WHO-recommended coverage, interventions must go beyond traditional education campaigns to incorporate inclusive, gender-responsive, and literacy-sensitive communication strategies. Community engagement, audience segmentation, and continuous evaluation of education programs are vital to ensure that interventions effectively reach all segments of the population and reduce the malaria burden.
Supplementary Information
Additional file1 (DOCX 39 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Khan S, Arnold F, Eckert E. Who uses insecticide-treated mosquito nets? A comparison of seven countries in Sub-Saharan Africa. DHS Program. Working Papers. 2008. Available from: https://dhsprogram.com/pubs/pdf/WP 58/WP 58.pdf