Multicenter real-life evaluation of the Post-CAR prognostic index for patients with large B-cell lymphoma after CAR-T failure
Mirko Farina, Elena Maiolo, Chiara Ghiggi, Piera Angelillo, Mattia Novo, Francesca Maria Quaglia, Luana Schiattone, Marta Lisa Battista, Lara Mannelli, Valeria Tomarchio, Elisa Lucchini, Luca Pagliaro, Greta Scapinello, Miriam Marangon, Sabrina Pelliccia, Roberta Sciarra

TL;DR
This study confirms the usefulness of a new tool called the Post-CAR Prognostic Index to predict outcomes for lymphoma patients who relapse after CAR-T therapy.
Contribution
The study validates the Post-CAR Prognostic Index in a multicenter real-world setting for patients with large B-cell lymphoma after CAR-T failure.
Findings
The PC-PI effectively stratified patients into risk groups with significantly different survival outcomes.
Patients receiving active post-progression therapy had much better survival than those without further treatment.
Bispecific antibodies were associated with the best survival outcomes among post-CAR-T patients.
Abstract
Most patients with large B-cell lymphoma (LBCL) progressing after CAR-T therapy experience poor survival and lack standardized treatment strategies. Prognostic tools are needed to guide decision-making at relapse. The Post-CAR Prognostic Index (PC-PI), recently proposed by Iacoboni et al., combines five routine clinical variables to stratify outcomes after CAR-T failure: ECOG (> 0), hemoglobin (< 10 g/dL), LDH (≥ 2xULN), number of extranodal sites (> 1) and time from CAR-T to progression (< 4 months). We evaluated the PC-PI in a retrospective multicenter study including 125 LBCL patients relapsing or refractory after axicabtagene-ciloleucel or tisagenlecleucel, treated between 2019 and 2023 across 16 Italian centers belonging to the Fondazione Italiana Linfomi network. Median overall survival (OS) was 4.9 months, with 6- and 12-month OS rates of 44.9% and 28.5%, respectively. The PC-PI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
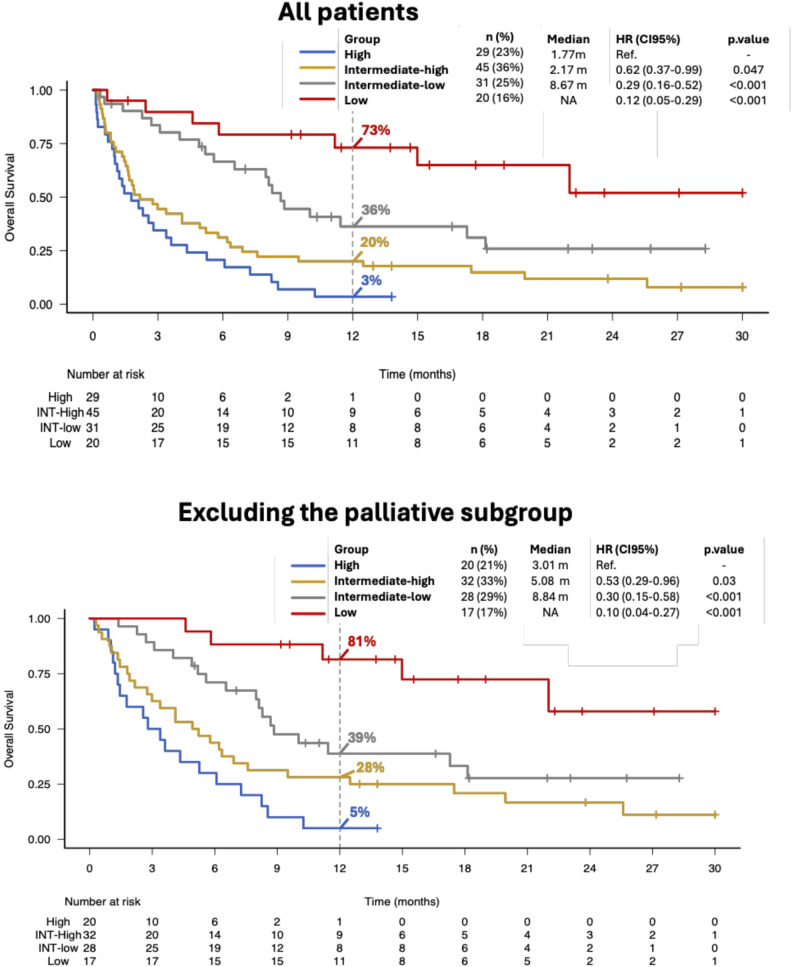 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCAR-T cell therapy research · Lymphoma Diagnosis and Treatment · Acute Lymphoblastic Leukemia research
To the editor,
Chimeric antigen receptor (CAR) T-cell therapy has transformed the treatment of relapsed/refractory large B-cell lymphoma (LBCL) [1–3]. Nonetheless, approximately 60% relapse or progress, a condition associated with limited survival and scarce evidence-based guidance [4–6]. In this scenario, clinicians must weigh aggressive salvage options against toxicity, while considering timely palliative care. Identifying prognostic factors for post-CAR-T progression is crucial to guide treatment intensity and improve quality of life [7–9]. The Post-CAR Prognostic Index (PC-PI) by Iacoboni et al. [10], represents a relevant and pragmatic step toward risk-adapted decision-making. The PC-PI combines five routine clinical variables at CAR-T progression or relapse—ECOG performance status, lactate dehydrogenase (LDH), hemoglobin < 10 g/dL, number of extranodal sites, and time from CAR-T infusion to progression—to classify patients into distinct risk groups with markedly different outcomes.
We qualitatively validated the PC-PI in a retrospective multicenter study including 125 LBCL patients progressing after axicabtagene ciloleucel (axi-cel) or tisagenlecleucel (tisa-cel) received in their third or later line of therapy between 2019 and December 31, 2023, across 16 Italian centers of the Fondazione Italiana Linfomi network. Institutional review board approval was obtained before data collection, and all procedures were conducted in accordance with the Declaration of Helsinki; written informed consent was available for all participants.
Of the 255 patients who received CAR-T therapy, 125 (49%) [65 axi-cel, 60 tisa-cel] subsequently relapsed or were refractory (Table 1). At the time of progression, the median age was 60.2 years (IQR 57.8–67.8). Most patients had advanced-stage disease (stage III–IV in 76%), with a median of 1 extranodal site (IQR 0–2). Median time from CAR T-cell infusion to relapse/progression was 2.2 months (IQR 1.2–4.2) and median follow-up from CAR-T failure was 20.4 months (95%CI, 14.0–24.1). Relapse or progression was histologically confirmed in 50% of cases, with CD19 loss detected by immunohistochemistry in 26 of 51 (51%) patients tested. The first subsequent treatment included immunotherapy or targeted agents in 57% of patients (20/125 with bispecific antibodies [BiABs]), chemotherapy or radiotherapy in 21%, and palliative care in 22% (Supplementary Material).
Our data confirm the prognostic value of the PC-PI [10] to effectively stratify outcomes in patients following CAR-T therapy failure. Median overall survival (OS) of the entire cohort was 4.9 months (95%CI 2.99–6.89), with a 6- and 12-month OS of 44.9% and 28.5%, respectively. Outcomes varied significantly by PC-PI groups: high-risk patients had a median OS of 1.8 months (95%CI, 0.99–3.38), intermediate-high risk 2.2 months (95%CI, 1.51–4.93), intermediate-low 8.7 months (95%CI, 5.59–17.28), while in the low-risk group the median OS was not reached (95%CI, 11.17–NA) (p < 0.0001, Fig. 1). Post-progression therapy had a major impact on survival, with patients receiving active treatment achieving a median OS of 7.3 months (95%CI, 5.2–9.5) versus 0.7 months (95%CI, 0.4–1.5) in those receiving no further therapy (p < 0.0001). The predictive performance of the PC-PI remained robust even after excluding patients who received only palliative care (Fig. 1B), and the score retained its ability to distinguish high- and low-risk patients irrespective of the CAR-T product used (Supplementary Material).
Patients treated after CAR-T failure with BiABs had significantly improved outcomes compared with those receiving other therapies (HR, 0.44; 95% CI, 0.21–0.88; p = 0.02), with 6- and 12-month OS rates of 90% and 55%, respectively. The PC-PI also effectively stratified high- vs. low-risk patients among those treated with BiABs or other immunotherapies (Supplementary Material).
A main strength of our analysis is its multicenter design, involving a larger number of centers than the study by Iacoboni et al. [10] and including both high- and low-volume CAR-T institutions. This confirms that the PC-PI is reproducible and applicable across heterogeneous real-world settings. Importantly, we show that the PC-PI retains its prognostic value regardless of the CAR-T product used and remains predictive among patients treated with BiABs or other immunotherapies after CAR-T failure. We acknowledge the retrospective design and treatment heterogeneity as limitations; however, the consistent prognostic discrimination across all subgroups supports the reliability and applicability of the PC-PI.
In conclusion, this multicenter real-world evaluation supports the PC-PI as a robust and clinically useful tool for risk stratification after CAR-T failure. Its reproducibility across diverse centers and therapeutic settings underlines its potential for integration into future risk-adapted post–CAR-T management strategies.
Fig. 1. Overall survival in the entire cohort and in the subset excluding patients receiving palliative treatment
Table 1. Patient characteristics overall and according to PC-PI risk classVariablesAll patientsN = 125HighN = 29Int-highN = 45Int-lowN = 31LowN = 20Age, *median years (range)*60.2 (18–75)59.1 (18–75)63 (38–75)61(22–74)61 (18–73)Male sex, *n (%)*76 (61)20 (69)29 (64)13 (42)14 (70)Histology, n (%)- DLBCL- HGBL- tFL- PMBL76 (61)24 (19)17 (14)8 (6)15 (52)7 (24)3 (10)4 (14)28 (62)9 (20)7 (16)1 (2)20 (65)7 (22)4 (13)0 (0)13 (65)1 (5)3 (15)3 (15)Prior lines > 2, *n (%)#*34 (27)8 (28)13 (29)8 (26)5 (25)Primary refractory, *n (%)#**89 (64)17 (59)31 (69)18 (58)14 (70)Previous HCT, *n (%)#*22 (18)3 (10)7 (16)4 (13)8 (40)Construct, n (%)- Axi-cel- Tisa-cel65 (52)60 (48)15 (52)14 (48)21 (47)24 (53)19 (61)12 (39)10 (50)10 (50)Best response to CART, n (%)- CR- PR- SD- PD28 (22)36 (29)12 (10)49 (39)2 (7)5 (17)2 (7)20 (69)5 (11)13 (29)4 (9)23 (51)13 (42)9 (29)4 (13)5 (16)8 (40)9 (45)2 (10)1 (5) CAR T-cell infusion to PD
- Median months (IQR)- < 4 months, n (%)2.2 (1.23–4.17)92 (74)1.2 (0.87–2.1)28 (97)2 (1.23–3.23)40 (89)3 (1.85–5.73)19 (61)6 (4.3–9.7)5 (25)ECOG, n (%)- 0- 1- > 126 (21)39 (31)60 (48)2 (7)7 (24)20 (69)4 (9)12 (27)29 (64)4 (13)17 (55)10 (32)16 (80)3 (15)1 (5)Stage, n(%)- I- II- III- IV11 (9)19 (15)26 (21)69 (55)1 (3)1 (3)5 (17)22 (76)3 (7)9 (20)9 (20)24 (53)3 (10)6 (19)6 (19)16 (52)4 (20)3 (15)6 (30)7 (35) Extranodal sites
- Median (IQR)- ≥ 2, *n (%)*2 (0–2)38 (31)2 (2–4)21 (72)1 (0.25–2.25)14 (31)1 (0–1)1 (3)1 (0–1)0 (0) Hemoglobin
- Median g/dL (IQR)- < 10 g/dL, *n (%)*10.9 (9.4–12)33 (29)10.7(10–11.4.4)7 (24)11 (9.1–12)13 (29)11(9.5–11.8)8 (26)12 (9.8–12.9)5 (25) Neutrophils
- Median x10^9^/L (IQR)- < 1.0 × 10^9^/L, *n (%)*1,95 (1.1–3.4)22 (20)1.65 (1.2–2.7)4 (14)3 (1.59–4.18)6 (13)1 (0.9–2.3)7 (23)2 (1.1–3.3)5 (25) Platelets
- Median x10^9^/L (IQR)- < 50 × 10^9^/L, *n (%)*116 (72.5–175)23 (21)142 (47–190)7 (25)125 (84–151)7 (16)113 (67–165)6 (19)127 (81–179)3 (15)LDH, n (%)- > 1 xULN- ≥ 2 xULN85 (68)33 (26)26 (90)18 (62)31 (69)13 (29)17 (55)1 (3)11 (55)1 (5)Subsequent strategy, n (%)- Immuno/Targeted- Chemo/Radiotherapy- Palliative care47 (38)51 (40)27 (22)6 (21)14 (48)9 (31)17 (38)16 (35)12 (27)15 (48)13 (42)3 (10)9 (45)8 (40)3 (15)Allo-HCT, *n (%)*19 (15)0 (0)5 (11)10 (32)4 (20)DLBCL, diffuse large B-cell lymphoma; HGBL, high-grade B-cell lymphoma; tFL, transformed follicular lymphoma; PMBL, primary mediastinal B-cell lymphoma; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; Allo-HCT, allogeneic hematopoietic cell transplantation; IQR, interquartile range; LDH, lactate dehydrogenase; Int-high, intermediate-high risk; Int-low, intermediate-low risk
Supplementary Information
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schuster SJ, Tam CS, Borchmann P, Worel N, Mc Guirk JP, Holte H et al. Long-term clinical outcomes of tisagenlecleucel in patients with relapsed or refractory aggressive B-cell lymphomas (JULIET): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol [Internet]. 2021 [cited 2022 Mar 22];22:1403–15. Available from: https://pubmed.ncbi.nlm.nih.gov/34516954/10.1016/S 1470-2045(21)00375-234516954 · doi ↗ · pubmed ↗
- 2Abramson JS, Palomba ML, Gordon LI, Lunning MA, Wang M, Arnason J et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet [Internet]. 2020 [cited 2025 Sep 13];396:839–52. Available from: https://www.thelancet.com/action/show Full Text?pii=S 014067362031366010.1016/S 0140-6736(20)31366-032888407 · doi ↗ · pubmed ↗
- 3Di Blasi R, Le Gouill S, Bachy E, Cartron G, Beauvais D, Le Bras F et al. Outcomes of patients with aggressive B-cell lymphoma after failure of anti-CD 19 CAR T-cell therapy: a DESCAR-T analysis. Blood [Internet]. 2022 [cited 2025 Sep 13];140:2584–93. Available from: https://pubmed.ncbi.nlm.nih.gov/36122385/10.1182/blood.202201694536122385 · doi ↗ · pubmed ↗
- 4Alarcon Tomas A, Fein JA, Fried S, Flynn JR, Devlin SM, Fingrut WB et al. Outcomes of first therapy after CD 19-CAR-T treatment failure in large B-cell lymphoma. Leukemia [Internet]. 2023 [cited 2025 Sep 13];37:154–63. Available from: https://pubmed.ncbi.nlm.nih.gov/36335261/10.1038/s 41375-022-01739-2PMC 989221136335261 · doi ↗ · pubmed ↗
- 5Chow VA, Gopal AK, Maloney DG, Turtle CJ, Smith SD, Ujjani CS et al. Outcomes of patients with large B-cell lymphomas and progressive disease following CD 19-specific CAR T-cell therapy. Am J Hematol [Internet]. 2019 [cited 2025 Sep 13];94:E 209. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC 6776079/10.1002/ajh.25505 PMC 677607931056762 · doi ↗ · pubmed ↗
- 6Iacoboni G, Iraola-Truchuelo J, O’Reilly M, Navarro V, Menne T, Kwon M, et al. Treatment outcomes in patients with large B-cell lymphoma after progression to chimeric antigen receptor T-cell therapy. Hema Sphere. 2024;8. 10.1002/hem 3.6210.1002/hem 3.62PMC 1110679838774657 · doi ↗ · pubmed ↗
- 7Iacoboni G, Navarro V, Sesques P, Rejeski K, Bastos-Oreiro M, Serpenti F et al. Development and validation of the post-CAR prognostic index for large B-cell lymphoma patients after CAR-T progression in third or later line treatment. J Hematol Oncol [Internet]. 2024 [cited 2025 Sep 13];17. Available from: https://pubmed.ncbi.nlm.nih.gov/39468591/10.1186/s 13045-024-01608-8PMC 1152087339468591 · doi ↗ · pubmed ↗