Co-production with marginalised workers: working with homecare workers and managers caring for people approaching end-of-life
Zana Bayley, Cat Forward, Helene Elliott-Button, Justine Krygier, Caroline White, Mark Pearson, Liz Walker, Colin Moss, Jamilla Hussain, Paul Taylor, Jane Wray, Helen Roberts, Miriam J. Johnson

TL;DR
This paper describes a co-production process with homecare workers and managers to create training resources for end-of-life homecare, addressing a gap in workforce involvement.
Contribution
The first successful co-production of end-of-life care training resources with underrepresented homecare workers and managers.
Findings
Co-production workshops enabled power-sharing and created training resources tailored to homecare workers.
Challenges included inconsistent attendance and engagement from some participants.
The five co-production principles fostered inclusivity and enriched the final outputs.
Abstract
Co-production is important due to its effectiveness in creating relevant and meaningful outputs for use in social and healthcare practice, however, frontline staff such as homecare workers (also known as aides, personal assistants or domiciliary care workers providing paid care within the home) are a key group within the social care workforce who are under-represented in this approach. Here, we report our coproduction process engaging with this workforce to develop training resources for workers providing end-of-life homecare. To co-produce training resources with homecare workers and their managers to support and educate workers delivering end-of-life homecare using evidence from our larger qualitative interview study. We conducted a series of 12 co-production workshops with UK-based homecare workers and managers (partners) to design training resources and recommendations for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
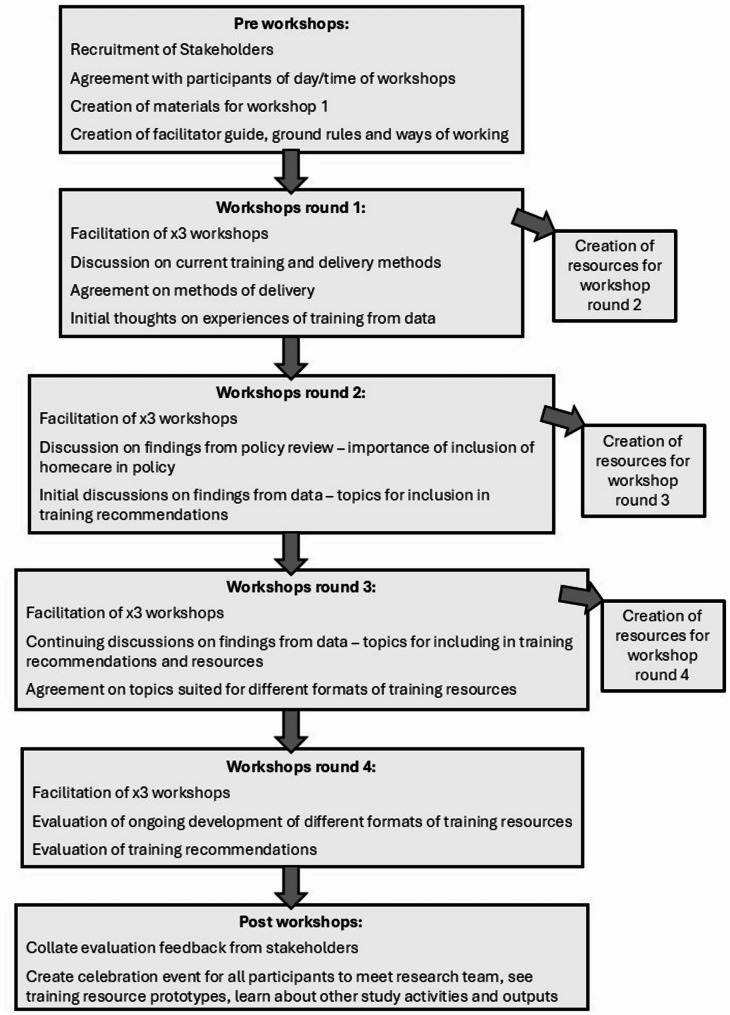 Figure 1
Figure 1- —https://doi.org/10.13039/501100000272National Institute for Health and Care Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare innovation and challenges · Geriatric Care and Nursing Homes · Palliative Care and End-of-Life Issues
Background
In the UK, homecare workers, (also called aides, care assistants, domiciliary carers, personal assistants or other titles in the UK and overseas), are a crucial workforce providing essential individualised, and relational basic personal care and support to people in their own homes [1, 2]. As people approach the end-of-life, many need care and support from homecare workers, particularly those wishing to remain (and die) in their own home.
Training is crucial to enable homecare workers to work safely, confidently, and effectively, and can improve care quality, staff retention, and overall service user satisfaction [3]. Providing quality end-of-life homecare and managing the challenging emotional and psychological impact of such work requires staff training informed by real-world examples and experiences [4, 5]. In the UK, end-of-life care training for the homecare workforce varies in terms of availability and quality [1] with no standardisation for workers and providers. However, ongoing, end-of-life care training is needed to help improve provision of this care [6] for example, in managing symptoms like breathlessness or pain [7].
Co-production is an emerging field in health and social care [8, 9], including the co-creation of educational materials [10–12]. In this paper we adopt the definition of co-production as the process of co-developing a solution to a problem [13]. Co-production is more effective, relevant, engaging, and impactful, and outputs more likely to be accepted and used in health and social care [27, 28]. Despite the increased interest in this approach, there are few reports about the involvement of care services in co-developing solutions, reducing the ability for others to learn from best practice and prior experience [14], with few practical illustrations of co-creation approaches [8]. To our knowledge, none have included homecare workers. This workforce is often overlooked in health and social care service research and its implementation [15]. This is despite over 14,000 recognised homecare organisations providing care to over one million people in the UK [16] and homecare provision becoming a key issue worldwide due to an ageing population, increased family mobility, and increasing complexity of care required within the home setting [17, 18]. Knowledge mobilisation describes the generation, sharing and use of evidence within health and social care [19]. Here, we report how we designed and delivered successful co-production workshops with homecare workers and managers as partners to share and use evidence to develop focused, relevant, and appropriate training resources.
Aim
To describe the process of co-producing training resources with homecare workers and their managers to support and educate workers in delivering end-of-life care.
Parent study background
The SUPPORTED study [20], explored the experiences and training needs of homecare workers providing homecare at end-of-life and identified the topic areas and delivery approaches for training. Detailed methods and findings of this study are reported elsewhere [21–23]. In summary, we found that homecare workers are not routinely trained or knowledgeable about caring for clients approaching end-of-life, and have little engagement or involvement with any other professionals providing care, such as community nursing, hospices, therapy services or local charity support. The topic areas for training content and delivery considerations are shown in Table 1 below.
Table 1. Identified training topics and training resource formatsAgreed Topic Areas for TrainingFirst steps into end-of-life care‘Just a care worker’ – understanding what you bringPracticalities of delivering care at end-of-lifeLooking after yourselfHomecare worker as a professionalEnd-of-life care and the unexpectedThe final months of life – what might it look like?Different conditions – what you might seeNot just the physical – psycho-social and spiritual careCommunication skillsWorking with those important to the people you care forWorking with other professionalsEffective management – beyond the teamInteracting as a teamAdvanced communication skillsExpanding the role of the homecare workerDelivery Considerations – Agreed FormatsSlide decks for face-face teachingNarrated slide decks for remote learningWhat if…? Cards for adhoc ‘bitesize’ learning and supporting supervisions, debriefs, group and individual learning
Co-production methods
Co-production uses a participatory approach, where project facilitators and partners-with-experience work collaboratively, sharing power and valuing each other’s different expertise [24]. We adopted five key principles of co-production: Sharing of power; Including all perspectives and skills; Respecting and valuing knowledge; Reciprocity; and Building and maintaining relationships [25].
Recruitment
We invited homecare workers and homecare agency managers across England from organisations who had engaged in the SUPPORTED study, as well as using social media and established contacts known to the project team to identify other partners. Skills for Care, a national workforce development organisation, also promoted the workshops through their networks. As this population are under-represented in service development or research, getting access to, and positive responses from homecare providers was difficult. They were unfamiliar with the structure and purpose of coproduction, which, together with a varied and irregular work pattern, for example, no regularly time-tabled shifts, and workers on zero hours contracts, meant that sustained effort throughout the 7-month period was required to gain and maintain sufficient numbers.
From 133 people who registered to participate in the workshops, 31 homecare workers and 46 agency managers took part in 12 workshops (one face-face; 11 online) in four rounds of three parallel workshop sessions over a period of seven months during 2024 to enable the co-production of training resources. 37 people attended more than one session but attendance was unpredictable (see Table 2).
Table 2. Workshop attendancesWorkshop roundAgreed to attendActual attendanceAttendance for each workshopPreviously attended1301910, 6, 3-232213, 7, 115342206, 7, 716439175, 7, 516
Workshops were chosen to allow space for discussion, reflection, and refinement [26]. Planning of the co-production workshops was supported by a service user advisory group comprising of homecare workers and carers (family or friends) of people who had received care. They provided important feedback such as the use of parallel sessions to ensure managers and homecare workers were given separate spaces to openly contribute. The stages of the workshops are illustrated below in Fig. 1.
Fig. 1. Workshop stages
Our project team members included five experienced qualitative researchers with professional backgrounds in education, occupational therapy, social work, medicine, nursing, and social care, as well as transferable skills in facilitating workshop discussions and dialogue. One, who had professional training and experience in education, took responsibility for creating workshop resources and facilitator guides. A facilitator’s guide was produced for every workshop to ensure consistency. These detailed each activity including suggestions for stimulating discussion. Two team members facilitated each workshop to ensure partners felt included, and their perspectives were valued, rather than just perceived as an add-on to enhance research quality [29]. Having two facilitators reduced the risk of missing any important information or insight shared by partners, as a form of member-checking the information shared.
Data collection
Each workshop was video recorded in addition to facilitators making notes to aid accurate recall and summary of key points and decisions made. These were then used to help produce initial versions of the resources, and plan for the subsequent rounds of workshops where resources were refined.
Results
The workshop series enabled us to report three key areas. Firstly, the impact of our techniques on the co-production process, secondly the impact of co-production on the training resource outputs, and thirdly, the impact of participation in the co-production activities on the partners.
Impact of co-production techniques
The use of the various techniques helped foster knowledge sharing and collaborative working to co-produce training resources. The techniques we used which evidence each of the co-production principles [19] are shown in Table 3.
Table 3. Summary of co-production principles and techniques usedCo-production principlesTechniques usedSharing of power - The research is jointly owned,* and people work together to achieve a joint understanding*Researcher role designated as facilitatorPartners involved in the design and content of workshop seriesSharing of decision-making relating to resource production Including all perspectives and skills - Make sure the research team includes all those who can contribute Facilitators supported with guidance on how to manage group sessionsAccessible workshop design through format and materials usedFacilitators’ knowledge and skills in active listening and probing to encourage contributionsImplementing ‘Ways of Working’ plan to facilitate inclusionUse of technology (i.e. Microsoft Teams) to enable partners to contribute Respecting and valuing the knowledge of all those working together on the research - Everyone is of equal importance Facilitators encouraged group discussionsWorkshop materials provided in understandable language and style in advanceDirect acknowledgement of expertise and experiences of partnersRecording of session and note-taking to enable use of knowledge sharedPartners received payment for their contribution Reciprocity - Everybody benefits from working together Workshops achieved consensus among partners re: training materials design and contentPartners co-produced a list of recommendations for trainingPartners collaboratively decided on importance of training areasPartners gained knowledge on purpose of research, research methods, and co-production techniques Building and maintaining relationships Accommodation of partners’ needs in relation to scheduling of workshops, materials provided, structure of sessionsCreation of inclusive and respectful workshop environmentRegular communication throughout workshop series on impact of involvement and processes of co-productionInvitation to end of research celebration event
We dedicated preparatory time to develop materials for supporting the workshops and guiding partners; a key component of effective co-production [12]. We observed that the ‘Ways of Working’ and ‘Ground Rules’ materials helped us to establish a shared understanding of the workshop environment, especially important as many of the partners had not engaged in co-production activities before. The materials covered issues such as confidentiality and respect, encouraged inclusion, active listening, use of cameras and microphones for online sessions, and recording of sessions. We reminded partners of these ways of working, which helped us facilitate the workshops in a friendly, open, and inclusive way, and develop a rapport within groups. The partners advised us that they appreciated a structure with facilitators to guide discussion and to encourage people to contribute. These ground rules allowed us to create a safe and supportive space for us to monitor group dynamics, ensuring all were given time and space to share their perspectives [30].
Resource packs were created for each session, where we presented the information from the SUPPORTED study in accessible formats; these were shared in advance of each workshop. This was planned to help partners feel more prepared and confident for the session’. Partners also told us that it helped them to acquire new knowledge and understanding around the SUPPORTED study’s findings. They felt better able to engage and contribute to the workshops, resulting in higher quality co-produced outputs. We dedicated some of the early workshop sessions to providing an insight into the previous research process from the SUPPORTED study, explaining terminology and practices such as data analysis. This was a form of knowledge mobilisation and making the process more relevant, which has been argued to be an effective strategy for co-production in health research [17].
Partners were paid for their time in line with the National Institute of Health Research (NIHR) and best practice for co-production guidelines. Payment encouraged recruitment and participation as homecare workers advised that they appreciated this, particularly as we also paid for time to read and review the material prior to the workshops. Payments also helped to demonstrate that we valued their time and expertise and provided a tangible benefit for their involvement; particularly relevant for a low-paid workforce.
We used our series of workshops to enable a larger number of perspectives to be heard across the groups, and to develop ideas as the resources were developed. The workshops were arranged at mutually convenient times. Some workshops were held at the weekend or during the evening to accommodate the varying needs of a workforce who provide a 24/7 service. Our approach of having multiple workshops, each building on the previous session, enabled us work at a slower and focused pace [31] and develop relationships, as we found over half of partners attended more than one workshop.
Impact of co-production
The various strategies we employed to build rapport, support inclusion, and work in a mutually beneficial workspace enabled significant homecare worker input to the development of the training resources throughout the workshops.
The first round of workshops was focused on initial ideas and concepts for the resources. The proposal to ensure some training was targeted at managers arose from concerns that as often the gatekeepers for staff to undertake training, they need to have the knowledge and skills to do so. The partners also helped to shape the length, format, and level of training – advising that training should be tiered to suit different stages of career, be available in different formats depending on whether it is face-face or remote training, and different lengths to suit a “coffee break” snippet or longer dedicated training sessions.
In the second round we shared some initial findings from the research study, which prompted discussions on the key topics that training should cover, influencing our curriculum document. The partners also worked with us on our policy review findings and agreed that policy around end-of-life care must include community-based care workers, because of the crucial work they provide for people who often want to be at home when approaching end-of-life.
We presented more findings from the SUPPORTED study for the third round of workshops. This enabled partners to consider specific areas of training that we could develop, for example, managing conflict, emotional burden, and signs of dying. We were also able to work together to understand which training was better suited to different formats, for example, partners were keen that any training focused on communication such as working with family members, should be designed for a face-face delivery style i.e. PowerPoint slides for a manager/trainer.
In the final round of workshops, partners were able to advise on draft versions of training material we had produced following their suggestions in round 3. This critique enabled us to modify and refine our resources. We were also able to share a draft version of our training recommendations document, which we were able to collectively improve to be more reflective of what the research and our partners feel is most useful and effective.
The culmination of all the workshops enabled us to generate a suite of resources including a training recommendations booklet, Powerpoint slide decks, PowerPoint videos with voiceover, and a series of printable postcards entitled “What if…” cards which detail a response to a fictional question based on the research data and the workshops discussions e.g. “What should I do if my client says something inappropriate to me?”.
We recorded the impact of the partner’s recommendations within each round of workshops separately and have summarised these in Table 4.
Table 4. Impact of Co-production on outputsPartner RecommendationImpact Workshop 1 Training managers is crucial to better support homecare workers, and to potentially provide in-house end-of-life care trainingSeparate recommendations for end-of-life care training have been created for managersEnd-of-life care training should be at distinct levels as new homecare workers may be overwhelmed by too much content on end-of-life careAdaptation of training recommendations into three levels of ‘first weeks’, ‘first months’ and ‘advanced’ for homecare staff, including training aimed at managerial level to support workers when learning about end-of-life careAny materials should be easily accessibleWe will ensure all end-of-life care training materials are freely accessible online and agencies can print off resources to give to staff who cannot access onlineTraining sessions should be different lengths of time to allow for remote learning and in-person trainingPresentation length was reduced, with space for lengthening or merging materials to create longer sessions by agencies if required to meet specific end-of-life care training needs locally.Any materials need to include case studies, scenarios, and problem-based learningCase studies from our data, input from expert writers knowledgeable of end-of-life care, and fictional situations have been included in the trainingMaterial should be permanently available, for refresher training even after completionMaterial will be freely available at any time onlineTraining should be personalised to suit learners –delivery, content, approach, assessmentMaterial can be modified by managers to suit their individual learners and context of their own location and staffConsider accreditation of any training contentThis is beyond the scope of this project, but it has been included as part of our policy recommendationsEnsure communication is a key component of any end-of-life care trainingTraining in communication has been included within the end-of-life care training resources Workshop 2 Identified reasons for homecare workers to be included in policy on community-based end-of-life careSome of the points raised have been integrated into our policy recommendationsIdentification and agreement on critical areas of training needs for homecare workers, based on findings from research data themesUsed in first draft of training recommendations and considered when creating list of training resource topics Workshop 3 Further dentification of important training areas through discussion and activities drawing on themes from interview data analysis findingsUsed to generate list of end-of-life care training resources to be created, and development of the training recommendations document Workshop 4 Critiqued draft recommendations with guidance on improvementsCritique used to modify recommendations for training curriculumCritiqued draft formats of training resources with guidance on improvementsResources modified according to workshop suggestions including colour, layout, format. Recommendations to keep text levels minimal, employing colourful and fun design, include interaction, space for discussion and reflection, and quotes where possible shared with resource writers. Allowance for mangers to modify where appropriate. Recommendations influenced final designs including hearing the authentic voice of experts including homecare workers and managers.
Discussion
We report a successful collaboration which valued each other’s expertise and knowledge. Co-production is a flexible and holistic method of developing educational materials [32] more likely to be adopted and usable [12], but which comes with its own challenges and tensions [33]. We managed challenges and tensions, being mindful of the difficulties of working with a workforce poorly represented in co-production, who benefitted from adapted strategies for inclusion within co-production [34]. We had to build trust within the homecare workforce, aware that the lack of experience and knowledge of co-production could cause mistrust and reluctance to contribute [27].
Changes to practices and cultures are needed to enable the application of co-production principles [33]. The specific support needs required for collaborations with under-represented groups such as the homecare workforce [15] need to be understood, and a bespoke plan made, which is flexible around the context, content, and the cohorts engaged [34].
Co-production has enabled previously marginalised service users to become equal partners [35]. This was true in our experience with the homecare workforce. By incorporating co-production principles into the planning and delivery of the workshops we evidence tangible outcomes that were directly influenced by homecare workers and homecare managers. These outcomes were not just in terms of the training resources produced, but also in the mutual benefits for both the project team members and the homecare workers and managers involved, who were able to develop a closer relationship and understanding about their different perspectives and knowledge base.
We aimed to co-produce training resources with homecare workers and homecare managers, as we wanted our resources to be grounded in their experiences and expertise and be useful within the care sector. To our knowledge, this is the first study to develop training resources for homecare workers that has not only used data directly sourced from homecare workers and those associated with home care at end-of-life but also partnered with homecare workers and managers to collaboratively co-produce resources.
This report provides an example of a successful method used to create training resources for health and social care service providers who are often not included in collaborative and inclusive practice, have no regulation regarding what end-of-life training (if any) they should receive, and yet are arguably one of the most essential care providers of end-of-life homecare. Previous studies around education and training for end-of-life care have not been developed with this workforce in mind, and many are not able to access training due to costs, availability, or lack of support by their employers. Our study has endeavoured to address that omission to benefit this crucial and yet often unheard workforce.
Challenges and lessons learned
We faced challenges and learned lessons about co-production with an unfamiliar and marginalised group. As the workshops were offered nationally, we could not offer in-person options in every round. This may have been a barrier for some who feel less confident or lack the necessary technology or digital confidence to contribute online. However, online sessions, and acknowledging that homecare can be a 24/7 job, often alongside other caring and family commitments, enabled opportunities for participation at various times of the day and week with sessions agreed collaboratively with partners. Also, we were able to offer this opportunity to people nationally, allowing us to include experiences from different regions, which may commission homecare services at end-of-life differently.
The sustained commitment of our partners is a key strength, as most opted to return for subsequent workshops, which was not a requirement or anticipated by the team. Having stages of workshops enabled those who returned to see the generation and growth of the training resources, provided confirmation that their contribution materially affected the development of resources, and enabled a greater appreciation of the value and purpose of co-production.
Due to the study timeframe, the resources could not be made available for a fuller appraisal before the end of the workshops, however all attendees will be able to access these once completed. This was a limitation of the study design itself, where the timing of the workshops should have coincided better with the physical production of the resources to allow more testing of content, design, and accessibility.
Reluctance to contribute, and non-attendance need to be considered when designing co-production activities with a workforce who are time-poor, engaged in an unpredictable work environment, and who have little experience of such involvement which might cause anxiety prior to attending, or distrust in the genuineness of the process (fear of tokenism). We needed to recruit homecare workers and managers throughout the period to ensure we had enough for each round. Possible strategies to mitigate these difficulties in the future may be to provide more guidance and support on what to expect within a co-production workshop setting, and background on co-production as a method for applying new knowledge. This would help partners to be more confident in their expectations of what was required in the workshops, and the benefits of their engagement. Also, the format of a group discussion online is not necessarily the preferred format for some people, and 1–1 sessions with facilitators could be considered, depending on numbers and practical issues around workload.
We were not able to robustly evaluate the process with our partners which limited our understandings of their perspectives on the workshop format, process, and outcomes. We did not conduct interviews exploring their experience of the process, and although we did conduct a short survey, so few people responded (11/40), this gave little useful information. Low completion of the evaluation survey may reflect their marginalised status, as people from minority groups, low-literacy, and/or language and access barriers have been associated with poor responses in surveys [36]. There may be other reasons for non-response, including unfamiliarity of workshops and evaluation processes; concern that negative feedback would not be acted upon or valued; lack of priority given by a time-poor workforce; and difficulties in quantifying views with a Likert scale or expressing them in written form in the free text [37, 38]. Lower education levels and low incomes and non-response have been previously linked [39, 40]. The low response from the survey underlines the need for a more direct engagement with people less used to being asked for feedback, such as interviews, or individual contact to assist survey completion.
Conclusion
We provide an example of co-production of training resources with an under-represented social care workforce, evidencing adopted strategies that enabled effective engagement over a sustained period. We explain how we engaged with these partners adopting the five key principles of co-production, enabling collaboration in the creation of training resources to support homecare workers delivering care at end-of-life. We share the learning points and challenges which may help others planning similar co-production activities with under-represented groups. Finally, we acknowledge the need to develop current national strategies for increasing social care service improvement and research engagement with consideration of the uniqueness of the homecare workforce [15].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nagata C, Tsutsumi M, Kiyonaga A, Nogaki H. Evaluation of a training program for community-based end-of-life care of older people toward aging in place: a mixed methods study. Nurse Educ Pract. 2021.54 10.1016/j.nepr.2021.10309110.1016/j.nepr.2021.10309134087577 · doi ↗ · pubmed ↗
- 2National Audit Office. The Adult Social Care Market in England [Internet]. 2021 [cited 2025 May 26]. Available from: https://www.nao.org.uk/press-releases/adult-social-care-markets/.
- 3Hughes S. Domiciliary care, self and older age [dissertation]. Anglia Ruskin University; 2023. https://hdl.handle.net/10779/aru.23760969.v 1.
- 4Bayley Z, Bothma J, Bravington A, Forward C, Hussain J, Manthorpe J, et al. Supported: Supporting, enabling, and sustaining homecare workers to deliver end-of-life care: A qualitative study protocol. P Lo S ONE. 2023;18(12). 10.1371/journal.pone.0291525.10.1371/journal.pone.0291525 PMC 1071842738091299 · doi ↗ · pubmed ↗
- 5Bayley Z, Forward C, White C, Elliott-Button HL, Krygier J, Walker L, Pearson M, Hussein J, Taylor PM, Wray J, Roberts A. Addressing barriers to interprofessional working with homecare workers in community palliative care: insights from a multi-site qualitative case study in England. Med Rxiv. 2025 Aug;15:2025–08.10.1177/02692163251383385 PMC 1277977041277395 · doi ↗ · pubmed ↗
- 6NIHR. Guidance on co-producing a research project [Internet]. 2024 https://www.learningforinvolvement.org.uk/content/resource/nihr-guidance-on-co-producing-a-research-project/.
- 7Filipe A, Renedo A, Marston C. The co-production of what? Knowledge, values, and social relations in health care. P Lo S Biol. 2017;15(5):e 2001403. 10.1371/journal.pbio.2001403.10.1371/journal.pbio.2001403 PMC 541499628467412 · doi ↗ · pubmed ↗
- 8Massey M. Survey practice in Non-Survey-Literate populations: lessons learned from a cognitive interview study in Brazil. Surv Pract. 2025;19(SI). 10.29115/SP-2024-0035.10.29115/SP-2024-0035 PMC 1198766140224398 · doi ↗ · pubmed ↗