Impact of Millet-Based Dietary Intervention on the Nutritional Status of Children in Rural and Tribal Andhra Pradesh, India
Arti Gupta, Pulla Sirisha, Joe Amalan, Venkatashiva Reddy B, Rajeev Aravindakshan, Dadi J Madhuri, Durgavajjala P Manaswini, Dokiburra G Rachana, Yusuf N Shaik, Maharshi Deepa

TL;DR
A community-led millet recipe program improved children's nutrition in rural and tribal areas of India.
Contribution
Demonstrates that community-led millet interventions reduce child undernutrition through increased consumption.
Findings
Millet consumption increased from 26.2% to 39.4% after the intervention.
Underweight prevalence decreased from 35.0% to 21.3% (p < 0.001).
Children with mothers attending ≥7 sessions had higher millet consumption and lower underweight rates.
Abstract
Background: According to the International Year of Millets 2023, millets are incredible ancestral, nutrient-rich, climate-resilient grains recognized for their role in preventing malnutrition. However, their consumption among young children remains low due to changing food preferences and limited awareness. This study evaluates the nutritional impact of millet-based interventions among children aged two to six years in rural and tribal regions of Andhra Pradesh, India. Objectives: To assess millet consumption and nutritional status at baseline, identify socio-demographic determinants of undernutrition and to evaluate the effectiveness of a community-led millet recipe intervention (“Mother’s Kitchen”) on improving dietary intake and growth outcomes. Methods: A cohort-based survey was conducted among 345 children across Rayalaseema, Uttar Andhra, and Coastal Andhra. Maternal,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
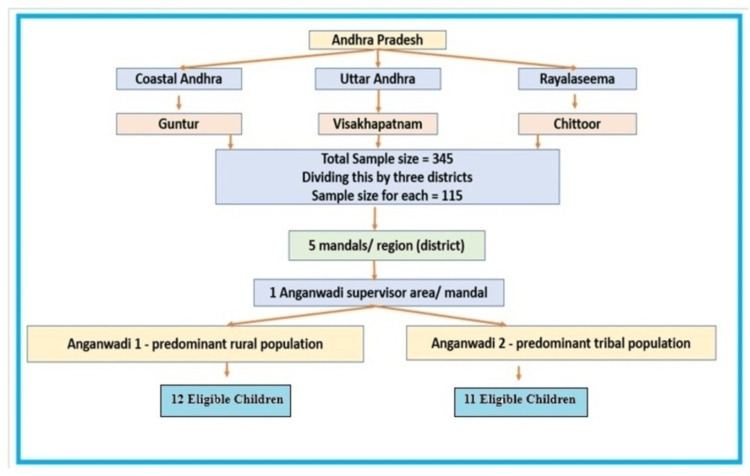 Figure 1
Figure 1| Child's age in months | Rayalaseema | Uttar Andhra | Coastal Andhra | Total | ||||||||||||
| Rural | Tribal | Rural | Tribal | Rural | Tribal | Rural | Tribal | |||||||||
| Category | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % |
| 24-35 | 14 | 23.33 | 14 | 25.45 | 19 | 31.7 | 11 | 20 | 5 | 8.33 | 3 | 5.45 | 38 | 21.11 | 28 | 16.97 |
| 36-47 | 15 | 25 | 12 | 21.82 | 14 | 23.3 | 31 | 56.36 | 21 | 35 | 20 | 36.36 | 50 | 27.78 | 63 | 38.18 |
| 48-60 | 20 | 33.33 | 17 | 30.91 | 17 | 28.3 | 11 | 20 | 26 | 43.33 | 15 | 27.27 | 63 | 35 | 43 | 26.06 |
| 61-71 | 11 | 18.33 | 12 | 21.82 | 10 | 16.7 | 2 | 3.64 | 8 | 13.33 | 17 | 30.91 | 29 | 16.11 | 31 | 18.79 |
| Total | 60 | 100 | 55 | 100 | 60 | 100 | 55 | 100 | 60 | 100 | 55 | 100 | 180 | 100 | 165 | 100 |
| Fischer's Exact/Chi-Square Test | 0.403 | 14.986 | 6.511 | 6.211 | ||||||||||||
| Degrees of freedom (df) | 3 | 3 | 3 | 3 | ||||||||||||
| p value | 0.94 | 0.002 | 0.089 | 0.102 | ||||||||||||
| Gender | Rayalaseema | Uttar Andhra | Coastal Andhra | Total | ||||||||||||
| Rural | Tribal | Rural | Tribal | Rural | Tribal | Rural | Tribal | |||||||||
| Category | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % |
| Female | 31 | 51.67 | 27 | 49.09 | 33 | 55 | 30 | 54.55 | 24 | 40 | 31 | 56.36 | 88 | 48.89 | 88 | 53.33 |
| Male | 29 | 48.33 | 28 | 50.91 | 27 | 45 | 25 | 45.45 | 36 | 60 | 24 | 43.64 | 92 | 51.11 | 77 | 46.67 |
| Total | 60 | 100 | 55 | 100 | 60 | 100 | 55 | 100 | 60 | 100 | 55 | 100 | 180 | 100 | 165 | 100 |
| Fischer's Exact/Chi-Square Test | 0.76 | 0.002 | 3.079 | 0.68 | ||||||||||||
| Degrees of freedom (df) | 1 | 1 | 1 | 1 | ||||||||||||
| p value | 0.783 | 0.961 | 0.079 | 0.409 | ||||||||||||
| District | Site | Baseline | Endline | ||||
| n | Median (g/day) | Interquartile Range (IQR) (g/day) | n | Median (g/day) | Interquartile Range (IQR) (g/day) | ||
| Rayalaseema | Rural | 38 | 38.34 | 41.67 | 58 | 50.00 | 8.34 |
| Tribal | 41 | 50.00 | 58.34 | 47 | 50.00 | 0.00 | |
| Total | 79 | 43.33 | 60 | 105 | 50.00 | 8.34 | |
| Uttar Andhra | Rural | 1 | 30.00 | - | 16 | 28.34 | 38.83 |
| Tribal | 1 | 3.33 | - | 7 | 13.33 | 20 | |
| Total | 2 | 16.67 | - | 23 | 26.67 | 36.66 | |
| Coastal Andhra | Tribal | 9 | 13.33 | 10.84 | 7 | 16.67 | 3.33 |
| Total | 9 | 13.33 | 10.84 | 7 | 16.67 | 3.33 | |
| Total | Rural | 39 | 36.67 | 40 | 74 | 50.00 | 16.67 |
| Tribal | 51 | 36.67 | 60 | 61 | 50.00 | 20 | |
| Total | 90 | 36.67 | 50 | 135 | 50.00 | 16.67 | |
| Millet recipe | Baseline | Endline | ||
| n | % | n | % | |
| Ragi Malt | 7 | 7.87 | 12 | 8.22 |
| Ragi Dosa | 1 | 1.12 | 10 | 6.85 |
| Ragi Sangati | 81 | 91.01 | 1 | 0.68 |
| Jowar Dosa | - | - | 4 | 2.74 |
| Ragi Idli | - | - | 5 | 3.42 |
| Ragi Laddu | - | - | 3 | 2.05 |
| Jowar Roti | - | - | 6 | 4.11 |
| Jowar Popcorn | - | - | 105 | 71.92 |
| Total | 89 | 100 | 146 | 100 |
| Variable | Proportion of children who consumed millets | |||||||
| n | Baseline survey # | Endline survey | Relative Risk (95%CI) | Z statistics | P value | |||
| n | % (95%CI) | n | % (95%CI) | |||||
| Step 1: Excluding attrition | ||||||||
| Number of children excluding attrition | 343 | 90 | 26.2(21.9 to 31.1) | 135.0 | 39.4(34.3 to 44.6) | - | -5.267 | <0.001^ |
| Step 2: Stratifying mothers with respect to the number of local millet recipe talks attended | ||||||||
| >=7* | 117 | 32 | 61.0 | 2.23 (1.42 to 3.53) ^ | -4.849 | <0.001^ | ||
| <7 | 226 | 58 | 25.7 (20.4-31.7) | 74.0 | 32.7 (27.0-39.1) | -2.530 | 0.006^ | |
| Underweight among children | Rayalaseema | Uttar Andhra | Coastal Andhra | Total | ||||||||||||
| Rural | Tribal | Rural | Tribal | Rural | Tribal | Rural | Tribal | |||||||||
| Category | n | % | n | % | n | % | n | % | n | % | N | % | n | % | n | % |
| Moderate | 5 | 8.33 | 8 | 14.55 | 14 | 23.3 | 12 | 21.82 | 11 | 18.33 | 18 | 32.73 | 30 | 16.67 | 38 | 23.03 |
| Severe | 4 | 6.67 | 2 | 3.64 | 11 | 18.3 | 19 | 34.55 | 7 | 11.67 | 10 | 18.18 | 22 | 12.22 | 31 | 18.79 |
| Normal | 51 | 85.00 | 45 | 81.82 | 35 | 58.3 | 24 | 43.64 | 42 | 70.00 | 27 | 49.09 | 128 | 71.11 | 96 | 58.18 |
| Total | 60 | 100.00 | 55 | 100.00 | 60 | 100.0 | 55 | 100.00 | 60 | 100.00 | 55 | 100.00 | 180 | 100.00 | 165 | 100.00 |
| Fisher's exact/ Chi square | 1.519 | 4.128 | 5.273 | 6 | ||||||||||||
| Degrees of freedom (df) | 2 | 2 | 2 | 2 | ||||||||||||
| p value | 0.468 | 0.127 | 0.072 | 0.041 | ||||||||||||
| Variable | Category | Present (n=121) | Absent (n=224) | Total (n=345) | Unadjusted Odds ratio | OR CI 95% | p value | Adjusted OR | AOR CI 95% | p value | |||||
| n | % | n | % | n | % | Upper | lower | upper | lower | ||||||
| Mother age (years) | <=25 (ref) | 53 | 43.8 | 107 | 47.8 | 160 | 46.4 | 0.0852 | 0.546 | 1.329 | 0.481 | - | - | - | - |
| >25 | 68 | 56.2 | 117 | 52.2 | 185 | 53.6 | |||||||||
| Mother's age at marriage (years) | <18 (ref) | 25 | 20.7 | 30 | 13.4 | 55 | 15.9 | 1.684 | 0.939 | 3.021 | 0.078 | -0.425 | 0.264 | -1.115 | 0.227 |
| >=18 | 96 | 79.3 | 194 | 86.6 | 290 | 84.1 | |||||||||
| Mother occupation | Not working (ref) | 80 | 66.1 | 174 | 77.7 | 254 | 73.6 | 0.561 | 0.343 | 0.916 | 0.02 | 0.331 | 0.938 | -0.276 | 0.286 |
| Working | 41 | 33.9 | 50 | 22.3 | 91 | 26.4 | |||||||||
| Father occupation | labour (ref) | 76 | 62.8 | 140 | 62.5 | 216 | 62.6 | 1.013 | 0.641 | 1.601 | 0.955 | - | - | - | - |
| Others | 45 | 37.2 | 84 | 37.5 | 129 | 37.4 | |||||||||
| Mother's education status | Middle school or less (ref) | 54 | 44.6 | 62 | 27.7 | 116 | 33.6 | 2.106 | 1.325 | 3.345 | 0.001 | -0.288 | 0.328 | -0.904 | 0.36 |
| More than Middle school | 67 | 55.4 | 162 | 72.3 | 229 | 66.4 | |||||||||
| Father's education status | Middle school or less (ref) | 58 | 47.9 | 80 | 35.7 | 138 | 40.0 | 1.657 | 1.057 | 2.597 | 0.027 | -0.072 | 0.523 | -0.666 | 0.813 |
| Socioeconomic status | More than Middle school | 63 | 52.1 | 144 | 64.3 | 207 | 60.0 | ||||||||
| Middle class or lower (ref) | 104 | 86.0 | 173 | 77.2 | 277 | 80.3 | 1.803 | 0.989 | 3.287 | 0.0052 | -0.863 | -0.17 | -1.556 | 0.015 | |
| More than the middle class | 17 | 14.0 | 51 | 22.8 | 68 | 19.7 | |||||||||
| Consanguineous marriage of parents | No (ref) | 84 | 69.4 | 162 | 72.3 | 246 | 71.3 | 0.869 | 0.535 | 1.411 | 0.57 | - | - | - | - |
| Yes | 37 | 30.6 | 62 | 27.7 | 99 | 28.7 | |||||||||
| Standard of living index | low (ref) | 35 | 28.9 | 38 | 17.0 | 73 | 21.2 | 1.992 | 1.178 | 3.369 | 0.009 | 0.075 | 0.782 | -0.631 | 0.835 |
| Medium or more | 86 | 71.1 | 186 | 83.0 | 272 | 78.8 | |||||||||
| Child gender | Male (ref) | 59 | 48.8 | 110 | 49.1 | 169 | 49.0 | 0.986 | 0.634 | 1.535 | 0.951 | - | - | - | - |
| Female | 62 | 51.2 | 114 | 50.9 | 176 | 51.0 | |||||||||
| Child's age in months | 24-48 | 50 | 41.3 | 129 | 57.6 | 179 | 51.9 | 0.519 | 0.331 | 0.812 | 0.004 | 0.877 | 1.419 | 0.336 | 0.002 |
| 49-72 | 71 | 58.7 | 95 | 42.4 | 166 | 48.1 | |||||||||
| Child known case of disease | yes (ref) | 7 | 5.8 | 10 | 4.5 | 17 | 4.9 | 0.761 | 0.282 | 2.053 | 0.589 | - | - | - | - |
| No | 114 | 94.2 | 214 | 95.5 | 328 | 95.1 | |||||||||
| Prelacteal | Yes | 45 | 37.2 | 60 | 26.8 | 105 | 30.4 | 0.618 | 0.385 | 0.991 | 0.045 | 0.236 | 0.861 | -0.388 | 0.458 |
| No (ref) | 76 | 62.8 | 164 | 73.2 | 240 | 69.6 | |||||||||
| Exclusive breastfeeding | Yes | 55 | 45.5 | 69 | 30.8 | 124 | 35.9 | 1.872 | 1.186 | 2.955 | 0.007 | -0.492 | 0.123 | -1.107 | 0.117 |
| No (ref) | 66 | 54.5 | 155 | 69.2 | 221 | 64.1 | |||||||||
| Child immunized for age | Fully (ref) | 101 | 83.5 | 124 | 55.4 | 225 | 65.2 | 4.073 | 2.356 | 7.04 | <0.001 | -1.093 | -0.304 | -1.883 | 0.007 |
| Partially | 20 | 16.5 | 100 | 44.6 | 120 | 34.8 | |||||||||
| Child millet consumed in 24-hour dietary recall | Yes | 14 | 11.6 | 76 | 33.9 | 90 | 26.1 | 0.255 | 0.137 | 0.475 | <0.001 | 1.362 | 2.289 | 0.436 | 0.004 |
| No | 107 | 88.4 | 148 | 66.1 | 255 | 73.9 | |||||||||
| Site | Rural | 52 | 43.0 | 128 | 57.1 | 180 | 52.2 | 0.565 | 0.884 | 0.362 | 0.012 | 0.649 | 1.209 | 0.088 | 0.023 |
| Tribal | 69 | 57.0 | 96 | 42.9 | 165 | 47.8 | |||||||||
| Variable | Underweight child | |||||||
| N | Baseline survey # | Endline survey | Relative Risk (95%CI) | Z statistics | P value | |||
| n | % (95%CI) | N | % (95%CI) | |||||
| Step 1: Excluding attrition | ||||||||
| Number of children excluding attrition | 343 | 120 | 35.0 (30.1-40.2) | 73.0 | 21.3 (17.3-25.9) | - | 5.039 | <0.001 |
| Step 2: Stratifying mothers with respect to the number of local millet recipe talks attended | ||||||||
| >=7* | 117 | 34 | 29.1 (21.6-37.9) | 20.0 | 17.1 (11.3-25.0) | 0.673 (0.380-1.192) | 2.858 | 0.002 |
| <7 | 226 | 86 | 38.1(32.0 -44.5) | 53.0 | 23.5 (18.3-29.4) | 4.158 | <0.001 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Nutrition and Water Access · Social and Economic Development in India · Food Security and Health in Diverse Populations
Introduction
Millets, often called nutri-cereals, are small-grained crops valued for their hardiness and role in sustainable agriculture. Public health efforts in India now prioritize reviving traditional foods, with millets at the forefront due to their nutritional and cultural importance [1]. India produces nearly 80% of Asia’s millet supply and 20% of the supply, with Andhra Pradesh having a historically deep connection to these grains. Unlike refined rice and wheat, millets are naturally gluten-free and nutrient-dense, making them a smart dietary choice [2]. They provide B vitamins, calcium, magnesium, zinc, and polyphenols while offering high fiber, low calories, and a low glycaemic index benefits, which support cholesterol reduction and blood sugar control [3]. Varieties such as finger millet (ragi), pearl millet (bajra), foxtail, and little millet are especially rich in iron [4].
Despite these nutritional benefits, millet consumption among young children (two to six years) remains inadequate, and they are particularly vulnerable to nutritional gaps, with iron deficiency anaemia remaining the leading global cause of morbidity and mortality in this age group [5]. Millets help address these deficiencies through high bioavailability of iron, calcium, and other micronutrients. Research shows that including millets, often as ragi sangati, in young children’s diets improves protein and iron intake and supports growth [6].
However, multiple socioeconomic and behavioural barriers impede widespread adoption of millet, contributing to persistent childhood malnutrition [7]. Parental education, especially maternal schooling at the middle or lower levels, also correlates with poor child nutrition [8]. Mothers often cite unfamiliarity, limited availability, and preference for other grains as obstacles [7]. Breastfeeding practices matter too: exclusive breastfeeding protects against underweight, while prelacteal feeding increases risk [9]. Additionally, the rise of fast foods and packaged snacks has reduced millet acceptance among children [10].
Community-based interventions, such as mother-led millet recipe sessions using local and affordable ingredients, have successfully boosted consumption and improved child nutrition [9]. The study aimed to assess millet intake, identify socio-demographic determinants of undernutrition, and evaluate the effectiveness of the "Mother's Kitchen millet" session on dietary intake and anthropometric outcomes.
Materials and methods
This is a cohort design study with baseline and end-line comparison conducted in 2024-2025, across three regions of Andhra Pradesh: Guntur district (Uttar Andhra), Visakhapatnam district and Anakapalle district (Coastal Andhra), and Annamayya district (Rayalaseema). The study population was children aged two to six years residing in the study area for ≥6 months, with written informed consent obtained from their parents/caregivers. Acutely sick children were excluded. The sample size calculations assume an estimated incidence with 15% precision and 95% confidence (1.96). A design effect of two and the number of clusters is 10. The cohort included 340 mothers. A total of 115 children were studied in one district. Five mandals were randomly selected in each district using the lottery method. A list of rural and tribal anganwadis in the mandal was received from the Integrated Child Development Services (ICDS) scheme office. Within one mandal, one anganwadi with predominantly rural children and one with predominantly tribal children were randomly selected from the list using a lottery method. A total of 23 children were studied in each mandal. Figure 1 presents the flow diagram of study participant recruitment.
Flow diagram of the study participant recruitment
For data collection, trained investigators used structured tools to collect socio-demographic, dietary, anthropometric, and morbidity data from parents/caregivers at baseline and endline (three months apart). For dietary assessment, an interactive, inter-rater-reliable 24-hour recall on three non-consecutive days, using visual aids from dietary software to measure food portions, was conducted. The 24-hour dietary recalls were administered by trained project staff who underwent training conducted both online and in person by experts in dietary assessment. Portion size estimation was facilitated using DietCalc software, supplemented by standardized utensils and photographs to enhance accuracy. Data collection occurred during both the forenoon and afternoon as per the participants' parents/caregivers' availability. Nutrient intake was calculated via the paid version of DietCalc with the Indian Food Composition Table 2017. All children were measured using SECA 210 and 213 instruments, which were calibrated at baseline and endline, respectively; malnutrition was assessed using the World Health Organization (WHO) Anthro (2006 standards) [11]. Anthropometric measurements were taken in duplicate for each child to ensure accuracy and reliability. All measurements were conducted during the forenoon or the afternoon, as per the child's availability. All study tools were piloted in the Center for Rural Health, Primary Health Care Nutakhi, All India Institute of Medical Sciences, Mangalagiri, to refine data collection tools and protocols. Data entry was checked for duplicates, and supervisory checks were conducted once every fortnight for 5% to monitor adherence to protocols.
The Mother's Kitchen program consisted of weekly, hands-on cooking demonstrations conducted over 12 weeks. Sessions were facilitated by a trained nutritionist, with step-by-step, quantity-wise recipe preparation, recipe samples, and community health workers at anganwadi centers, or participants homed in groups of 5-10 mothers. Each week featured a demonstration of two to three age-appropriate, culturally acceptable millet recipes using locally available ingredients. The intervention covered nine true millets (finger millet/ragi, pearl millet/bajra, foxtail millet, little millet, kodo millet, proso millet, barnyard millet, brown top millet, and sorghum/jowar) and two pseudo cereals (amaranth and buckwheat). Recipes were explicitly designed for children aged two to six years. Emphasizing palatability, ease of preparation, and nutrient density. Mothers were shown visual diaries with a step-by-step and quantity-wise recipe preparation, along with samples of recipes.
The Institute Ethics Committee of All India Institute of Medical Sciences, Mangalagiri, approved the study. All the mothers were given information on the research and provided a patient information sheet. The mothers who accepted to participate in the study were asked to provide written informed consent. There are no incentives/compensation provided to mothers.
All 345 mothers were being followed up as per protocol. Two mothers were relocated from the study area, resulting in attrition and leaving 343 mothers for the end-line analysis. Data were entered in Microsoft Excel (Microsoft® Corp., Redmond, WA). It was analysed using Statistical Product and Service Solutions (SPSS, version 29; IBM SPSS Statistics for Windows, Armonk, NY), WHO Anthro, and DietCalc. Descriptive statistics were reported; associations were tested via the chi-square test or Fisher’s exact test. Exposure was operationally defined as attending seven or more sessions of the Mother Kitchen Millet talk. Effectiveness assessed using Relative Risk and logistic regression (bivariate then multivariate, p<0.2 entry, p<0.05 significance).
Results
A total of 345 children (180 rural, 165 tribal) were enrolled across three regions. Two children were lost to follow-up, yielding an attrition rate of 0.6%.
Table 1 shows the age distribution of the studied children: in Rayalaseema, 48-60 months: rural 20 (33.3%) and tribal 17 (30.9%); and in Uttar Andhra, 36-47 months: tribal 31 (56.4%); 24-35 months: rural 19 (31.7%) (Table 1).
Table 2 shows gender distribution: (1) Rayalaseema - rural: 31 (51.7%) female and 29 (48.3%) male; tribal: 27 (49.1%) female and 28 (50.9%) male; (2) Uttar Andhra - rural: 33 (55.0%) female and 27 (45.0%) male; tribal: 30 (54.5%) female and 25 (45.5%) male; and (3) Coastal Andhra - rural: 36 (60.0%) male and 24 (40.0%) female; tribal: 31 (56.4%) female and 24 (43.6%) male.
Table 3 shows the median daily intake increased from 36.67 g (IQR: 50) at baseline to 50 g (IQR: 16.67) at endline across all sites. In Rayalaseema, rural millet intake rose from 38.34 g (IQR: 41.67) to 50 g (IQR: 8.34), while tribal median remained at 50 g. Uttar Andhra saw rural millet intake slightly drop from 30 g to 28.34 g, but tribal millet intake rose from 3.33 g to 13.33 g. Coastal Andhra tribal millet intake increased from 13.33 g to 16.67 g.
Table 4 shows baseline and endline millet recipes: Ragi Malt increased from 7 (7.87%) to 12 (8.22%) and Ragi Dosa rose from 1 (1.12%) to 10 (6.85%). New recipes appeared at the endline: Jowar Dosa (4, 2.74%), Ragi Idli (5, 3.42%), Ragi Laddu (3, 2.05%), Jowar Roti (6, 4.11%), and Jowar Popcorn (105, 71.92%).
Table 5 shows endline millet consumption in children rose significantly from 90 (26.2%) at baseline to 135 (39.4%) (Z = -5.267, p < 0.001). Children of mothers attending ≥7 recipe talks had 71 (61.0%) consumption vs. 74 (32.7%) for p-value < 0.001.
Table 6 shows that Uttar Andhra had the highest severe underweight rate (19, 34.6%) in tribal children, while Rayalaseema had the lowest overall underweight prevalence; tribal areas showed significant variance in underweight categories (p = 0.041).
Table 7 shows baseline underweight risk factors in 345 children (121, 35%). Maternal factors are as follows: age >25 years (68, 56.2%), early marriage (25, 20.7%), non-working (80, 66.1%), low education (54, 44.6%), low paternal education (58, 47.9%), low socioeconomic status (104, 86%), consanguinity (37, 30.6%), and low standard of living index (35, 28.9%). Child factors are follows: female (62, 51.2%), age 49-72 months (71, 58.7%), pre-lacteal feeding (45, 37.2%), exclusive breastfeeding (55, 45.5%), full immunization (101, 83.5%), and low millet intake (14, 11.6%).
Table 8 shows that, among 343 children, underweight prevalence decreased from 120 (35.0%) at baseline to 73 (21.3%) at endline (p < 0.001). In the ≥7 recipe talks group, underweight decreased from 34 (29.1%) to 20 (17.1%) (RR = 0.673, p = 0.002).
Discussion
The present study provides community-level evidence on the role of millets in improving nutritional outcomes among children aged two to six years in rural and tribal Andhra Pradesh. The demographic profile showed a balanced age distribution, with a higher concentration in the 36-60-month age group, consistent with declining fertility rates and effective family planning in rural India [10]. Gender ratios were near parity across regions, with minor male predominance in Coastal Andhra, aligning with National Family and Health Survey (NFHS)-5 trends of gradual normalization in the sex ratio at birth [12].
Morbidity was predominantly acute, with over 90% of children free from chronic conditions. Respiratory symptoms were the most reported, underscoring the persistent burden of acute respiratory infections in rural under-five populations [13]. The low detection of chronic illnesses likely reflects underdiagnosis in community settings rather than actual absence, emphasizing the need for enhanced paediatric screening [14].
Feeding practices varied significantly by region. Exclusive breastfeeding rates were high in Rayalaseema and Uttar Andhra (80-92%) but alarmingly low in Coastal Andhra (5-25%), particularly among tribal mothers, where top feeding predominated. This disparity mirrors NFHS-5 findings and is attributable to maternal employment, urbanization, and access to commercial milk substitutes [14-16]. Prelacteal feeding remained culturally entrenched in Uttar Andhra (56-63%), despite awareness campaigns, highlighting the influence of social norms [16]. Immunization coverage, however, was exemplary (92-100%), exceeding national averages and reflecting the success of initiatives such as Mission Indradhanush [12,17].
Maternal profiles revealed that young caregivers (21-30 years) were the primary decision-makers for child feeding [18,19]. Early marriage persisted in tribal communities (18-33%), exceeding national averages [20], and was associated with reduced dietary autonomy. Educational disparities were stark, with one in five tribal mothers being illiterate, a known determinant of poor dietary diversity. Socioeconomic constraints further shaped dietary patterns: tribal households relied heavily on daily wage labour and clustered in the lowest income quintile, sustaining millet consumption due to affordability and cultural continuity [20,21]. In contrast, upwardly mobile rural families increasingly favoured refined cereals, reflecting aspirational dietary shifts [22].
Millet consumption among children was dominated by ragi sangati, with limited variety or preparation options. This pattern aligns with traditional practices in South India, where ragi-based complementary foods are valued for digestibility and micronutrient density [3,18]. However, low-frequency and variety underscore barriers in acceptability, preparation complexity, and caregiver knowledge [8,23]. The 12-week Mother’s Kitchen intervention, with weekly hands-on millet recipe demonstrations, significantly improved dietary intake and nutritional status. A marked decline in underweight (from 35.0% to 21.3%, p < 0.001) was found. Children whose mothers attended ≥7 sessions showed superior outcomes (RR = 0.673 for underweight reduction), highlighting dose-response efficacy.
These gains are mechanistically supported by millet’s nutrient profile: high-quality protein (8-12 g/100 g), exceptional calcium in finger millet (300-350 mg/100 g), and iron (2-8 mg/100 g) with enhanced bioavailability through traditional processing such as fermentation and germination [24,25]. Comparative studies consistently favour millet-based over rice-based diets for anthropometric recovery, haemoglobin improvement, and sustained growth velocity [3,26,27]. Biofortified varieties further amplify iron and zinc absorption, with cognitive benefits observed in young children [27].
The intervention’s success hinges on maternal engagement and child-centric recipe design. Integration of millets with familiar foods (e.g., milk, pulses) improved palatability and compliance, outperforming direct supplementation models [3]. Community-based cooking demonstrations empowered mothers as agents of change, aligning with evidence that family-centered nutrition education yields higher adherence than institutional programs [28].
A key strength of this study lies in its rigorous cohort design with baseline and endline comparisons over a defined period across diverse regions of Andhra Pradesh. The use of cluster selection increased generalisability, while the training and quality control measures ensured data integrity. The limitations of this study included the 24-hour dietary recall obtained from the mother; the cohort inference study needs to be further validated by a larger randomized study; and the absence of a control group significantly limits the ability to draw causal inferences.
Despite high awareness of millet’s nutritional value, persistent barriers continue to limit widespread adoption. Taste preferences, especially among children, pose a significant challenge, often favoring Westernized or processed foods over traditional millet dishes. Culinary knowledge gaps and limited cooking confidence further limit the use of regular millet, while accessibility and affordability issues, particularly for less common millet varieties, compound the problem. To translate these findings into practice, we recommend scaling the Mother’s Kitchen model statewide through Anganwadi and self-help groups using child-friendly millet recipes, millet inclusion in ICDS, mid-day meals, and Pradhan Mantri Poshan Shakti Nirman (PM POSHAN) with biofortified varieties, and training primary healthcare workers in millet counselling paired with point-of-care anaemia screening. Targeted literacy-nutrition programs for mothers to enhance dietary autonomy. The subsidized Public Distribution System should strengthen millet supply chains.
Conclusions
This study confirms millets’ intake among Indian children, identifies socio-cultural and economic barriers to their growth, and demonstrates the success of the weekly Mother’s Kitchen intervention in Andhra Pradesh. Millets remain vital in low-income and tribal diets, protecting against anaemia and undernutrition, while refined grains dominate in wealthier households. Maternal education, early marriage, and feeding practices significantly influence outcomes. The intervention markedly improved intake of protein, energy, calcium, and iron, reducing underweight. Despite awareness, taste, accessibility, and convenience, adoption is limited. Community-led, culturally relevant education is critical to sustain millet integration across generations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moving towards sustainable food systems: a review of Indian food policy budgets Glob Food Sec Brown KA Srinivasapura Venkateshmurthy N Law C 1004622820213373818410.1016/j.gfs.2020.100462 PMC 7941605 · doi ↗ · pubmed ↗
- 2Prevalence of chronic morbidities and healthcare seeking behavior among urban community dwelling elderly population residing in Kalyani municipality area of West Bengal, India J Family Med Prim Care Ahamed F Ghosh T Kaur A Debnath A 419341991020213513678810.4103/jfmpc.jfmpc_893_21PMC 8797103 · doi ↗ · pubmed ↗
- 3Acceptance and impact of millet-based mid-day meal on the nutritional status of adolescent school going children in a peri urban region of Karnataka state in India Nutrients Anitha S Kane-Potaka J Tsusaka TW 20771120193148437710.3390/nu 11092077 PMC 6770931 · doi ↗ · pubmed ↗
- 4The nutritional powerhouse: unlocking the benefits of millets 12 2025 2023 https://www.investindia.gov.in/team-india-blogs/nutritional-powerhouse-unlocking-benefits-millets
- 5Odisha Govt introduced ragi ladoos as morning snack for preschool children in supplementary nutrition programme under ICDS’INVEST INDIA 12 2025 8https://www.smartfood.org/project/odisha-govt-introduced-ragi-ladoos-as-morning-snack-for-preschool-children-in-supplementary-nutrition-programme-under-icds/2020 https://indiaeducationdiary.in/odisha-govt-introduced-ragi-ladoos-as-morning-snack-for-preschool-children-in-supplementary-nutrition-programme-under-icds/
- 6Unlocking the nutritional, medicinal, and cultural treasures of ragi millet: a comprehensive exploration of botanical, historical, and health perspectives Int J of Pharm Sci Dharmani B Kumari P Gupta M Jangra S 19821272025
- 7Exclusive breastfeeding practices and its determinants in Indian infants: findings from the National Family Health Surveys-4 and 5Int Breastfeed J Reddy NS Dharmaraj A Jacob J Sindhu KN 691820233812406510.1186/s 13006-023-00602-z PMC 10731841 · doi ↗ · pubmed ↗
- 8Factors associated with appropriate complementary feeding: a scoping review J Pediatr Nurs Herman H Mansur AR Chang YJ 08971202310.1016/j.pedn.2023.04.01737150632 · doi ↗ · pubmed ↗