Implementation of a Self-Management Approach for Low Back Pain in a Public Health Care System
Ron Feldman, Tamar Pincus, Orna Reges, Alexandra Gorelik, Rachelle Buchbinder, Noa Ben Ami

TL;DR
A self-management approach for chronic low back pain was tested in a public health system and showed better outcomes with fewer sessions, but adoption was limited.
Contribution
Demonstrates the feasibility and effectiveness of a structured self-management model for chronic low back pain in a public health care setting.
Findings
ETMI was associated with greater improvements in function and fear-avoidance beliefs compared to usual care.
Patients receiving ETMI required fewer treatment sessions than those receiving usual physiotherapy care.
Only 17% of eligible patients received ETMI, highlighting challenges in large-scale implementation.
Abstract
This cohort study evaluates the feasibility of implementing the enhanced transtheoretical model intervention, a self-management approach to physiotherapy, and compares outcomes of patients who received the intervention vs usual physiotherapy care. Can a structured self-management intervention, the enhanced transtheoretical model intervention (ETMI), for people with chronic low back pain (CLBP), be feasibly implemented in a public health care system, and what patient outcomes are observed? In this cohort study of 128 physiotherapists and 4193 patients, 85.1% of physiotherapists were trained and 64.0% implemented ETMI in 711 patients with CLBP. Compared with usual care, ETMI-guided care was associated with greater improvements in function and fear-avoidance beliefs and required fewer treatment sessions. These findings suggest ETMI has the potential to improve outcomes for people with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
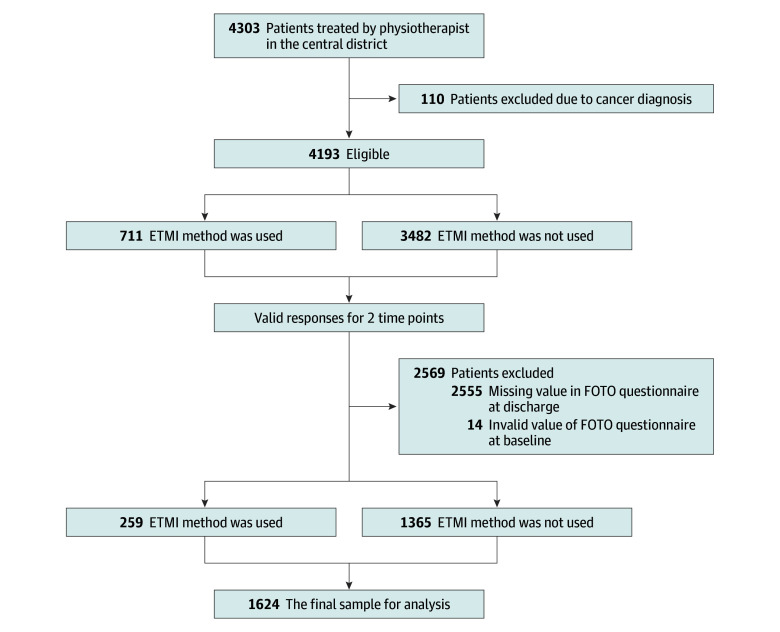 Figure 1
Figure 1| Variable | Participants, No. (%) | ||||
|---|---|---|---|---|---|
| All physiotherapists (N = 128) | Did not complete ETMI training (n = 19) | Completed ETMI training (n = 109) | |||
| Overall | Used ETMI with at least 1 patient (n = 70) | Did not use ETMI (n = 39) | |||
| Age, mean (SD), y | 37.5 (9.3) | 37.6 (9.0) | 37.6 (9.2) | 37.8 (9.3) | 37.2 (9.1) |
| Sex | |||||
| Female | 63 (49.2) | 11 (57.9) | 52 (47.7) | 34 (48.6) | 18 (46.2) |
| Male | 65 (50.8) | 8 (42.1) | 57 (52.3) | 36 (51.4) | 21 (53.8) |
| Years of experience | |||||
| <5 | 18 (14.1) | 5 (26.3) | 13 (11.9) | 9 (12.9) | 4 (10.3) |
| 5-10 | 37 (28.9) | 9 (47.4) | 28 (25.7) | 17 (24.3) | 11 (28.2) |
| 10-20 | 51 (39.8) | 2 (10.5) | 49 (45.0) | 30 (42.8) | 19 (48.7) |
| >20 | 22 (17.2) | 3 (15.8) | 19 (17.4) | 14 (20.0) | 5 (12.8) |
| MSc degree | 63 (49.2) | 11 (57.9) | 52 (47.7) | 34 (48.5) | 18 (46.1) |
| Satisfaction with the ETMI method | |||||
| Very satisfied | NA | NA | 83 (76.1) | 63 (90.0) | 20 (51.3) |
| Satisfied | NA | NA | 12 (11.0) | 6 (8.5) | 6 (15.3) |
| Neither satisfied nor dissatisfied | NA | NA | 9 (8.3) | 1 (1.5) | 8 (20.5) |
| Dissatisfied | NA | NA | 3 (2.8) | 0 | 3 (7.7) |
| Very dissatisfied | NA | NA | 2 (1.8) | 0 | 2 (5.2) |
| Variable | Included in the analysis (n = 1624) | Excluded from the analysis (n = 2569) | ||||
|---|---|---|---|---|---|---|
| Participants, No. (%) | Participants, No. (%) | |||||
| ETMI (n = 259) | No ETMI (n = 1365) | ETMI (n = 452) | No ETMI (n = 2117) | |||
| Age, mean (SD), y | 55.6 (15.8) | 57.1 (16.8) | .16 | 54.8 (16.5) | 56.6 (16.7) | .04 |
| Socioeconomic score (0-10, 10 is high), mean (SD) | 7.3 (2.0) | 7.3 (2.2) | .91 | 7.1 (2.1) | 7.2 (2.2) | .29 |
| BMI, mean (SD) | 27.2 (5.3) | 27.6 (5.1) | .28 | 28.0 (5.1) | 27.9 (5.4) | .86 |
| No. of physiotherapy visits, mean (SD) | 5.0 (4.2) | 6.3 (4.5) | <.001 | 2.9 (3.2) | 3.9 (4.2) | <.001 |
| Baseline function (0-100, 100 is a better function), mean (SD) | 47.5 (13.7) | 47.1 (14.0) | .70 | 51.4 (15.6) | 46.7 (15.5) | <.001 |
| Baseline pain score (0-10, 0 is no pain), mean (SD) | 6.0 (2.5) | 5.6 (2.5) | .01 | 5.4 (2.6) | 4.3 (2.7) | <.001 |
| Baseline fear avoidance beliefs (0-100, 100 is better), mean (SD) | 45.3 (21.6) | 45.2 (22.1) | .96 | 45.0 (21.6) | 44.9 (22.6) | .96 |
| Sex | ||||||
| Female | 150 (57.9) | 783 (57.4) | .87 | 263 (58.2) | 1258 (59.4) | .63 |
| Male | 109 (42.1) | 582 (42.6) | .86 | 189 (41.8) | 859 (40.6) | .67 |
| Hypertension | 71 (27.4) | 434 (31.8) | .16 | 122 (27.0) | 643 (30.4) | .15 |
| Diabetes | 23 (8.9) | 187 (13.7) | .03 | 45 (10.0) | 290 (13.7) | .03 |
| Ischemic heart disease | 13 (5.0) | 127 (9.3) | .02 | 39 (8.6) | 210 (9.9) | .40 |
| CVA/TIA | 4 (1.5) | 31 (2.3) | .46 | 8 (1.8) | 49 (2.4) | .48 |
| Anxiety or depression | 30 (11.6) | 176 (12.9) | .56 | 74 (16.4) | 312 (14.7) | .38 |
| No. of physical activity sessions per week | ||||||
| 0 | 100 (38.6) | 495 (36.2) | .76 | 141 (31.2) | 750 (35.4) | .37 |
| 1-2 | 81 (31.3) | 435 (31.9) | 154 (34.1) | 687 (32.5) | ||
| ≥3 | 78 (30.1) | 435 (31.9) | 157 (34.7) | 680 (32.1) | ||
| Referral pathway to physiotherapy | ||||||
| Orthopedic specialists | 68 (26.3) | 229 (16.8) | .001 | 161 (35.6) | 433(20.5) | <.001 |
| Family physician | 3 (1.2) | 25 (1.8) | 3 (0.7) | 53 (2.5) | ||
| Self-referral (direct access) | 188 (72.6) | 1111 (81.4) | 288 (63.7) | 1630 (77.0) | ||
| Unknown | 0 | 0 | 0 | 1 (<0.1) | ||
| Variable | Mean (SD) | Adjusted mean difference (95% CI) | |
|---|---|---|---|
| Usual physiotherapy care (n = 1365) | ETMI-guided care (n = 259) | ||
| Function | |||
| Baseline | 47.1 (14.0) | 47.6 (13.7) | 3.3 (1.5 to 5.1) |
| Discharge | 59.1 (16.5) | 63.2 (16.3) | |
| Change | 12.0 (13.7) | 15.7 (14.1) | |
| Pain | |||
| Baseline | 5.6 (2.5) | 6.0 (2.5) | −0.0 (−0.3 to 0.3) |
| Discharge | 3.9 (2.3) | 4.1 (2.4) | |
| Change | −1.7 (2.4) | −2.0 (2.4) | |
| Fear avoidance beliefs | |||
| Baseline | 45.2 (22.1) | 45.3 (21.6) | −4.3 (−7.0 to −1.7) |
| Discharge | 40.8 (21.6) | 36.4 (19.8) | |
| Change | −4.4 (22.7) | −8.9 (23.8) | |
| Variable | Mean (SD) | Adjusted mean difference (95% CI)a | |
|---|---|---|---|
| Usual physiotherapy care (n = 176) | ETMI-guided care (n = 30) | ||
| Function | |||
| Baseline | 45.9 (13.2) | 40.6 (13.8) | 5.8 (0.6 to 10.9) |
| Discharge | 55.6 (15.5) | 57.4 (17.4) | |
| Change | 9.7 (16.8) | 16.8 (14.2) | |
| Pain | |||
| Baseline | 5.0 (2.5) | 5.2 (2.7) | −0.5 (−1.3 to 0.3) |
| Discharge | 3.6 (2.2) | 3.0 (2.7) | |
| Change | −1.5 (2.4) | −2.1 (2.8) | |
| Fear avoidance beliefs | |||
| Baseline | 44.6 (22.7) | 49.3 (23.9) | −5.9 (−13.9 to 2.2) |
| Discharge | 42.1 (22.2) | 37.7 (20.5) | |
| Change | −2.6 (24.4) | −11.6 (28.5) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Diabetes Management and Education · Telemedicine and Telehealth Implementation
Introduction
Clinical guidelines for chronic low back pain (CLBP) recommend first-line management should include reassurance about the likely good long-term prognosis and assisting patients to self-manage their symptoms.^1,2,3^ Barriers to implementing these recommendations include misconceptions among clinicians about the causes and treatment of CLBP,^4,5^ limited knowledge and confidence in evidence-based approaches,^5,6^ and patient expectations about care^7,8^ Time constraints also make it challenging to deliver personalized, high-quality treatment.^9,10^ Additionally, encouraging people to be more physically active and reduce sedentary behavior remains difficult.^11^
In usual physiotherapy care for people with CLBP, treatment typically includes a combination of exercise therapy, education, manual techniques (such as mobilization or soft-tissue therapy), and adjunct modalities (eg, electrotherapy, dry needling, or heat and/or cold therapy). By contrast, the enhanced transtheoretical model intervention (ETMI) is a self-management approach for people with CLBP.^12^ Health care practitioners are trained to support patients by addressing unhelpful beliefs and providing education about natural recovery, helping them overcome barriers to self-management, and encouraging leisure-time physical activity.^12^ They are trained to use exposure to movement, accompanying patients during brisk walking sessions to demonstrate that movement is safe and not harmful. Through this process, patients gain confidence in their ability to move. By promoting active coping rather than focusing on symptom reduction, this approach helps patients reinterpret back pain as a common and self-limiting condition, thereby reducing fear avoidance and improving function.^12^ A central component of ETMI is helping patients to understand that regular physical activity is key to preventing and managing low back pain.^13^
A pragmatic clinical trial of ETMI vs usual physiotherapy care in people with CLBP (8 centers, 34 physiotherapists, and 220 CLBP participants) demonstrated that it is feasible to train physiotherapists to deliver ETMI within a short time frame, and its delivery resulted in significant improvements in function and reduced health care utilization.^12,14^ ETMI-guided care has been demonstrated to be acceptable to patients.^8^ The overall aim of this study was to investigate the feasibility of implementing ETMI-guided care for people with CLBP in 1 district (13 physiotherapy clinics) of Maccabi Healthcare Services (MHS). MHS is the second-largest public health care organization in Israel, operating across 5 districts and providing health care services to a population exceeding 2.5 million people nationwide. The primary aims were to determine the number of ETMI-trained physiotherapists who opted to use ETMI in practice (reach), the number of eligible patients who received ETMI-guided care (adoption), and the fidelity of the ETMI approach in their practice. We also assessed satisfaction with the ETMI method. Secondary aims were to explore the association between receiving ETMI-guided or usual physiotherapy care and clinical outcomes (function, pain, and fear-avoidance beliefs), and number of clinic visits. Finally, we also examined the association between depression and/or anxiety and clinical outcomes.
Methods
Study Design
This was a pragmatic implementation and cohort study comparing clinical outcomes of patients who received ETMI-guided vs usual physiotherapy care. It was informed by the Standards for Reporting Implementation Studies (StaRI) framework for implementation studies,^15^ and we followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cohort studies.^16^ The study was approved by the MHS institutional review board, which granted a full waiver of informed consent due to use of deidentified data. The study was registered at Clinicaltrials.gov on March 25, 2021 (NCT04819009).
Participants (Clinicians and Patients)
All physiotherapists working in 13 physiotherapy clinics in the Central District of MHS, a large public health maintenance organization in Israel, with at least 1 year of experience were invited to participate in ETMI training starting in January 2022. Participation was voluntary, and no financial incentives were provided. Physiotherapists who completed the ETMI training were asked to document the use of ETMI in patient care using the ETMI code in MHS’s database.
We included all patients aged 18 years or older who had received a diagnosis of CLBP based on the International Statistical Classification of Diseases, Eleventh Revision, Clinical Modification classification and sought treatment at a physiotherapy center within MHS’s central district between January 1, 2022, and July 31, 2023. We excluded patients with cancer.
Intervention: The ETMI Approach and Training
The ETMI approach is summarized in the eTable in Supplement 1 and described in detail elsewhere.^12,17^ In brief, it emphasizes the importance of listening to the patient’s story and validating their experiences, identifying and addressing misconceptions about the back problem, providing educational messages about the natural history of LBP, and providing reassurance that most patients will improve without treatment. It stresses the importance of physical activity and a healthy lifestyle, and the messages are tailored to the patient’s stage of change according to behavior change theory.^18,19^ In contrast to traditional physiotherapy care, no passive treatments or prescribed standard exercise programs are provided. Instead, the focus is on supporting the patient to do more physical activity they choose and enjoy. Patients who are hesitant about physical activity are provided with a safe exposure to brisk walking or running.
Participating physiotherapists attended 2-hour training sessions on ETMI during regular staff meetings. The first session focused on teaching the ETMI approach, while the second session allowed physiotherapists to share their experiences and challenges after using ETMI-guided care. The invitation was sent to all 13 clinics, and the managers selected 2 to 3 physiotherapists to participate in a 4-hour ETMI workshop (30 physiotherapists). This method was designed to ensure the identification and monitoring of difficulties that occurred during ETMI implementation. Following the ETMI training, participants were asked to complete a sociodemographic questionnaire and assess their satisfaction with the ETMI approach using a 5-point Likert scale, with response options ranging from very satisfied to very dissatisfied.
Outcome Measures
Implementation Outcomes
We determined the proportion of physiotherapists who adopted ETMI (reach) and number of patients receiving ETMI-guided care (adoption). To assess physiotherapists’ fidelity in applying ETMI, we performed in-person observations of 14 randomly selected physiotherapists at 7 different physiotherapy clinics. Fidelity was assessed using a study-specific ETMI fidelity checklist (eAppendix in Supplement 1), developed based on the core components of the ETMI approach.^12^ The checklist included items reflecting key communication behaviors, delivery of evidence-based messages about LBP, goal setting, and promotion of physical activity. Each item was rated as performed or not performed, and overall fidelity was expressed as the proportion of ETMI components delivered as intended. Satisfaction with the ETMI method was assessed on a Likert scale (very satisfied, satisfied, neither satisfied nor dissatisfied, dissatisfied, or very dissatisfied).
Patient Outcomes
As part of MHS routine care, all patients are asked to complete the Focus On Therapeutic Outcomes Lumbar Computerized Adaptive Test^20^ at baseline and at discharge. This tool has been validated for use in patients with back pain seeking rehabilitation in outpatient therapy clinics and is reliable and sensitive to change.^21^ It includes self-reported function measured on a linear scale of 0 to 100, with a higher score indicating greater function; self-reported pain intensity in the last 24 hours measured on a numeric rating scale of 0 to 10, with 10 indicating severe pain; and the Physical Activity subscale of the Fear Avoidance Beliefs Questionnaire (FABQ-PA) with scores (0 to 24) transformed to a 0 to 100 scale, where higher scores indicate greater fear of movement. The Hebrew version of the tool was cross-culturally translated using standardized procedures and is widely used in clinical practice.^22^ In populations similar to ours, the minimal clinically important difference (MCID) for function has been reported to range from 3 to 9 points, depending on the baseline score (overall MCID is 5, MCID is 3 for a baseline score of >51-58 and MCID is 9 for a baseline score <44)^21^; for pain, it has been reported to be 2 points,^23^ and for FABQ-PA it has been reported to be 4 points.^24,25^
Data Collection
We extracted data about all eligible physiotherapists from the central district in MHS, including their age, gender, years of experience, and whether they had a masters degree. Extracted patient data included gender, age, socioeconomic score (a weighted socioeconomic measure derived from economic and social data from the Israeli Central Bureau of Statistics, scored on a continuous scale from 0 to 10, with higher scores indicating higher socioeconomic position),^26^ body mass index, level of physical activity (none, 1-2 times per week, or 3 or more times per week), comorbidities, number of physiotherapy visits, use of ETMI, self-reported function, and pain and fear avoidance beliefs about physical activity at baseline and care discharge.
Statistical Analysis
All relevant data were extracted from MHS database and exported into SPSS version 27 (IBM) for analysis. All continuous data were tested for normality using the Shapiro-Wilks test. Summary statistics were used to describe both physiotherapists and patients included in and those excluded from the study. The results were reported as means (SD) for continuous variables and as numbers (percentages) for categorical variables. Similar methods were used to describe patients treated with ETMI and those treated with usual care.
The outcomes of ETMI on changes in function, pain, and fear-avoidance beliefs from baseline to discharge among CLBP patients compared with those who received usual physiotherapy care were assessed using t tests for continuous data and χ^2^ tests for categorical variables. A multilevel mixed-effect linear regression model with random effects for physiotherapist identification was used to examine the outcomes of ETMI (yes or no) on changes in function, pain, and fear-avoidance beliefs while controlling for age, gender, socioeconomic score as a continuous variable, diagnosed depression and/or anxiety, and the level of each variable at baseline.
The effects of depression and/or anxiety on the outcomes of interest are well established.^27^ Therefore, we not only adjusted the main analysis for baseline depression and/or anxiety, we also examined the association between ETMI and changes in function, pain, and fear avoidance beliefs score in the subset of patients with established depression and/or anxiety using the same methods.
The level of significance was set at P < .05 for all tests. The analysis of secondary or descriptive outcomes was not adjusted for multiplicity and should not be used to infer definitive treatment effects. All results were interpreted with respect to both statistical significance and clinical relevance.
Results
All 128 eligible physiotherapists (mean [SD] age, 37.5 (9.3) years; 63 [49.2%] female) agreed to participate in the ETMI training. A total of 109 (85.1%) completed the training and 19 (all from a single clinic) dropped out after the first session, citing resistance to the shift from traditional physiotherapy treatments to recommending physical activity and supporting self-management. Demographic factors were similar among those who did and did not complete ETMI training (Table 1).
Implementation Outcomes
Of those who completed the ETMI training, 70 (64%) implemented the intervention: 21 (30%) used it with 10% to 20% of their CLBP patients, 28 (40%) with 20% to 40%, and 21 (30%) with more than 40%. There were no differences in terms of gender, age, years of experience, or master qualification between physiotherapists who used ETMI and those who did not. Physiotherapists who used ETMI expressed greater satisfaction with the ETMI method compared with those who did not (odds ratio, 8.55; 95% CI, 3.14-23.29; P < .001).
Fidelity to ETMI-guided care was good among the 14 physiotherapists who were observed. Of these, 12 sessions (85.7%) were properly documented, 9 physiotherapists (64.2%) communicated evidence-based information on LBP, 13 (92.8%) discussed healthy lifestyles, and 10 (71.4%) conveyed the essential messages.
Overall, 4303 patients with CLBP attended at least 1 physiotherapy session during the study period (Figure). One hundred and ten (2%) were excluded due to a cancer diagnosis. Of the remaining 4193 eligible patients (mean [SD] age, 56.3 [16.7] years; 2454 [58.5%] women), 711 (17%) received ETMI-guided care at least once.
Flow Chart of Study Population Selection
Fourteen patients (0.3%) had incomplete baseline data, and 2555 (60.9%) did not attend their final treatment session and therefore did not have discharge data. The final analysis-ready dataset therefore included 1624 patients (39%), of whom 259 (15.9%) received ETMI-guided care and 1365 (84.1%) received usual physiotherapy care.
The sociodemographic and baseline clinical characteristics and referral pathways of patients according to whether or not they were included in the analysis and comparing those who received ETMI-guided care with those who did not are shown in Table 2. Overall, there were no clinically meaningful differences in baseline sociodemographic or clinical characteristics between those who did and did not receive ETMI-guided care, irrespective of whether they were included in the outcome analysis.
A higher proportion of patients included in the outcome analysis were self-referred, and this was consistent across ETMI and non-ETMI groups (χ^2^3 = 51.8; P < .001). Patients who received ETMI-guided care had fewer treatment sessions than patients who received usual care, and this was also consistent across both those included and excluded from the outcome analysis (mean [SD] 5.0 [4.2] vs 6.3 [4.5]; adjusted mean difference [aMD], 1.3; 95% CI, 0.6 to 1.8; P < .001 and 2.9 [3.2] vs 3.9 [4.2]; aMD, 1.0; 95% CI, 0.6 to 1.3; P < .001, respectively).
Patient Outcomes Analysis
Among the 1624 patients included in the outcomes analysis, those who received ETMI-guided care had greater improvements in function and fear-avoidance beliefs compared with those who received usual care (Table 3). The mean change (SD) in function score was 12.0 (13.7) with usual care and 15.7 (14.1) with ETMI-guided care (aMD, 3.3; 95% CI, 1.5 to 5.1), and the mean (SD) change in fear-avoidance scores was −4.4 (22.7) with usual care and −8.9 (23.8) with ETMI-guided care (aMD, −4.3; 95% CI, −1.7 to −7.0). Improvement in pain was similar in both treatment groups (mean [SD] change, −1.7 [2.4] with usual care and −2.0 [2.4] with ETMI-guided care; aMD, −0.0; 95% CI, −0.3 to 0.3).
For the subset of patients with depression and/or anxiety at baseline (206 patients), those who received ETMI-guided care (30 patients) had greater improvement in function at discharge compared with those who received usual care (176 patients). The mean (SD) change was 9.7 (16.8) with usual care and 16.8 (14.2) with ETMI-guided care (aMD, 5.8; 95% CI, 0.6 to 10.9). Improvements in pain and fear avoidance were similar in both groups (Table 4).
Discussion
We have demonstrated the feasibility of training physiotherapists in the ETMI approach and implementing it with fidelity into ETMI-guided care for patients with CLBP in a large public health care setting in Israel. Our findings showed that, compared with usual care, ETMI-guided care was associated with better outcomes in function and fear-avoidance beliefs and this was achieved with fewer treatment sessions. These clinical practice data are consistent with the results of a previous pragmatic clinical trial.^12,14^ Similar outcomes were also observed among the subset of patients with depression and/or anxiety, although only the difference in function was significant.
The improved function and fear-avoidance of physical activity beliefs with ETMI-guided care may reflect the behavioral focus of ETMI. The intervention targets patients’ beliefs and activity patterns rather than directly addressing pain symptoms, which may also explain a lack of difference in improvement in pain between the treatment groups.
While almost two-thirds of physiotherapists who completed training applied ETMI-guided care to at least 1 patient, ETMI-guided care was only provided to 17% of patients with CLBP overall. While this may indicate that 2 education sessions are insufficient to change practice, another explanation for the low overall uptake of the intervention is that physiotherapists may find it difficult to transition from actively treating people with CLBP to simply supporting their self-management. Previous qualitative studies with physiotherapists introduced to ETMI suggest that some see the approach as threatening to their professional identity.^28,29^ The transition from a clinician-managed approach to back pain that focuses on specific diagnoses, such as weak core muscles or poor posture, and treatments involving targeted exercises, passive modalities, and/or specialized techniques, toward a model that prioritizes patient self-management may be challenging for physiotherapists. Many are accustomed to a fixing mindset, making it difficult to shift toward empowering patients to manage their own recovery.
A previous study that determined the perceptions of patients with CLBP treated with ETMI approach found that patients had no problem with the fact that they did not receive passive treatment.^7,8^ They highlighted their need for reassurance and encouragement and perceived ETMI as a practical tool for self-management.
We found that a higher proportion of patients who had self-referred for care completed their final visit, indicating they may have had higher levels of engagement in their rehabilitation. However, there was no difference in the proportion of patients who failed to attend their final visit between those who were and were not treated with ETMI, suggesting that the type of care they received did not influence their decision to attend.
Strengths and Limitations
Our study had a pragmatic design with high ecological validity. The results are more likely a reflection of the true uptake of ETMI-guided care in clinical practice. Physiotherapists trained in the ETMI method may also have incorporated some ETMI features into their usual physiotherapy care, which may have underestimated the benefits of the ETMI approach. In addition, ETMI exposure was based on physiotherapists’ coding in the electronic medical record. Some ETMI elements may have been applied without formal coding, which could also have reduced the observed differences between groups.
Fidelity of ETMI delivery was assessed in a relatively small sample of physiotherapists (approximately 20%). While our observations provided useful insights, they may not fully represent the practices of all physiotherapists who delivered ETMI.
Due to the extent and uncertain mechanism of missing discharge data, multiple imputation was not performed, as it would likely violate the missing-at-random assumption. Consequently, the results are based on observed data from completers and may not be generalizable to all patients who received care. Additionally, the small number of participants with depression and/or anxiety limits the interpretation of our subgroup findings, which should be considered exploratory.
Conclusions
This cohort study found that the implementation of the ETMI approach within a large public health care system was feasible and associated with improved patient outcomes with fewer physiotherapy sessions and minimal practitioner training. Although the reach was limited, these findings highlight the potential of scalable, self-management–based interventions to enhance care efficiency and reduce resource use for people with CLBP. Wider adoption could contribute to more sustainable musculoskeletal care provided that implementation barriers are systematically addressed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Foster NE, Anema JR, Cherkin D, ; Lancet Low Back Pain Series Working Group. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368-2383. doi:10.1016/S 0140-6736(18)30489-629573872 · doi ↗ · pubmed ↗
- 2Maher CG, Archambeau A, Buchbinder R, . Introducing Australia’s clinical care standard for low back pain. Emerg Med Australas. 2023;35(3):370-373. doi:10.1111/1742-6723.1421837120762 · doi ↗ · pubmed ↗
- 3WHO guideline for non-surgical management of chronic primary low back pain in adults in primary and community care settings. 2023. Accessed November 20, 2025. https://www.ncbi.nlm.nih.gov/books/NBK 599212/38198579 · pubmed ↗
- 4Sharma S, Traeger AC, Reed B, Hamilton M, O’Connor DA, Hoffmann TC . Clinician and patient beliefs about diagnostic imaging for low back pain: a systematic qualitative evidence synthesis. BMJ Open. 2020; 23;10(8):e 037820. doi:10.1136/bmjopen-2020-037820 PMC 745153832830105 · doi ↗ · pubmed ↗
- 5Holopainen R, Simpson P, Piirainen A, . Physiotherapists’ perceptions of learning and implementing a biopsychosocial intervention to treat musculoskeletal pain conditions: a systematic review and metasynthesis of qualitative studies. Pain. 2020;161(6):1150-1168. doi:10.1097/j.pain.000000000000180931977935 · doi ↗ · pubmed ↗
- 6Lemmers GPG, Bier JD, van Lankveld W, Westert GP, Staal JB, van der Wees PJ. Guideline adherence of physiotherapists in the treatment of patients with low back pain: a qualitative study. J Eval Clin Pract. 2022;28(6):1147-1156. doi:10.1111/jep.1370335615965 PMC 9796459 · doi ↗ · pubmed ↗
- 7Feldman R, Nudelman Y, Haleva-Amir S, Ben Ami N. Patients’ prior perceptions and expectations of the enhanced transtheoretical model intervention for chronic low back pain: a qualitative study. Musculoskeletal Care. 2022;20(2):371-382. doi:10.1002/msc.160034726320 · doi ↗ · pubmed ↗
- 8Feldman R, Nudelman Y, Haleva-Amir S, Pincus T, Ben Ami N. Patients’ perceptions and outcome measures after undergoing the enhanced transtheoretical model intervention (ETMI) for chronic low back pain: a mixed-method study. Int J Environ Res Public Health. 2022;19(10):6106. doi:10.3390/ijerph 1910610635627641 PMC 9140490 · doi ↗ · pubmed ↗