A scoping and web-based review of current practices and lessons learnt in development and sustainability of global health emergency medicine fellowships
Haniya Khan, Alex McKnight, Kathleen Gamble, Lisa M Puchalski Ritchie, Melissa L Langhan, Lisa M Puchalski Ritchie, Stacey M. Kassutto, Lisa M Puchalski Ritchie

TL;DR
This paper reviews global health emergency medicine fellowships in high-income countries to understand their structure and lessons learned for program development.
Contribution
The study provides a scoping and web-based review of GHEM fellowship programs, highlighting gaps in trainee experiences and outcomes.
Findings
Eight articles and 43 websites were included, showing fellowship structures with 1–2 years duration.
Fellowships focus on clinical skills, education, research, or administration, funded by clinical hours.
Details on trainee experiences, international work, and outcomes were largely missing.
Abstract
Background: Despite significant interest in advanced global health training among Canadian emergency medicine trainees, only one global health emergency medicine (GHEM) fellowship existed in Canada at the time of this review. We conducted a scoping and web-based review to summarize the components of, and lessons learnt through development and implementation of global health emergency medicine fellowship programs to date, to inform program development. Methods: We conducted a scoping and web-based review by systematically searching electronic databases from inception to 2021 for articles and websites (2022) describing global health emergency medicine training programs based in high income countries. Results: From 2957 articles and 62 websites identified, eight articles and 43 websites were included in the review. Fellowships are generally structured as follows: 1–2 years duration…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
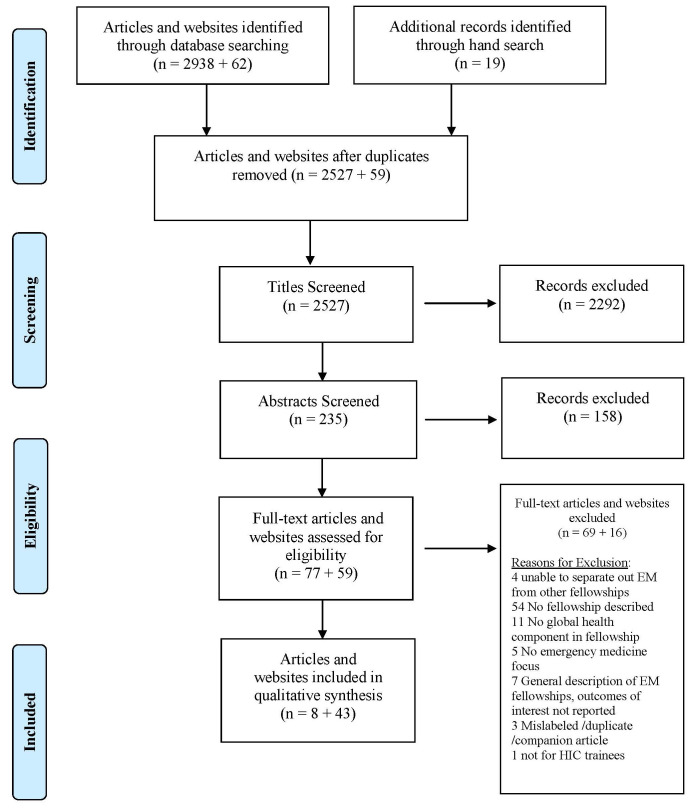 Figure 1
Figure 1| Anderson, Philip D.
| International
| Commentary
|
|
| Andescavage, S. M.
| Updated assessment of
| Study Abstract
|
|
| Bledsoe, Gregory H.
| Current status
| Study
|
|
| Crouse, Heather L.
| A Novel Approach to
| Commentary
|
|
| Jacquet, Gabrielle A.
| Fellowships in
| Study
|
|
| VanRooyen, M. J.
| International Health
| Commentary
|
|
| Collier, A.
| Global emergency
| Commentary Abstract
|
|
| Klesick, E.
| Global emergency
| Study
|
|
- —Faculty of Medicine University of Toronto, Education Development Fund.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Health and Surgery · Global Health Workforce Issues · Trauma and Emergency Care Studies
Introduction
Interest in global health training opportunities has grown rapidly over recent decades. In the United States, the percentage of medical students participating in global health experiences ranged from 15% to 27.1% from 2017 to 2021; a significant increase from 5.9% in 1978 ^ 1 ^. Over the same period, there has been an increase in the number of global health fellowships offered by North American academic institutions across a range of medical disciplines ^ 2, 3 ^. The first global health emergency medicine (GHEM) fellowship was introduced in 1994 ^ 4 ^. This number has increased steadily, with at least 39 currently available, accounting for over 40% of all global health fellowships offered ^ 5 ^.
Global health emergency medicine fellowships represent an avenue for academic institutions to deepen the learning experiences provided to trainees ^ 3, 6 ^. Such opportunities provide exposure to both a unique range of health conditions and spectrum of illness severity uncommon in high-income country settings ^ 3, 6 ^. In addition, trainees experience first-hand the challenges faced in providing clinical care within a resource limited healthcare setting. As a result, participants can gain clinical skills and may decrease their reliance on medical technologies while becoming more culturally sensitive and mindful of the resources available to them ^ 4 ^. However, fellowships vary significantly and little is known about best practices with respect to fellowship goals, structure, duration, supervision, and funding, in order to optimize trainees’ experience and program sustainability.
Despite significant interest in advanced global health training among Canadian medical trainees, only one emergency medicine-specific fellowship existed in Canada at the time of this review ^ 7 ^. To inform the development of a global health emergency medicine fellowship at the University of Toronto, we conducted a web-based and scoping review guided by the Johanna Briggs Institute guidance for scoping reviews ^ 8 ^. Our review addresses the following question: what are the current practices and lessons learnt to date in development and sustainability of global health emergency medicine fellowships for physicians during or post-residency based in high income countries?
Methods
Protocol
A protocol was developed for this review and registered with Open Science Framework ^ 9 ^. Reporting of findings was guided by the preferred reporting for systematic reviews and meta-analyses extension for scoping reviews (PRISMA ScR) ^ 10 ^.
Eligibility criteria
We included websites that provided details of global health emergency medicine fellowships and articles that presented the experiences of GHEM fellowship developers, programs, faculty or trainees as narrative reports, or original research articles of any design, including formal review articles, qualitative and quantitative designs. Only reports of global health emergency medicine fellowships offered through academic institutions based in high-income countries were included. Countries were defined as high-income according to the World Bank’s World Country and Lending Group classification. Articles where reports of fellowships based in low- and middle-income countries that could not be separated out were not included.
Information sources and literature search
A search strategy was developed in consultation with an experienced information specialist and peer-reviewed by a second information specialist using the Peer Review of Electronic Search Strategies checklist ^ 11 ^. The following databases were searched from inception to February 27, 2018 and subsequently updated to March 22, 2021, using medical subject heading (MeSH) headings and text words related to emergency medicine, fellowship, global health, and high income countries: OVID MEDLINE and EMBASE, CAB global health, CINAHL, HealthSTAR, ISIS Web of Science, EBM reviews, DARE abstracts, Scopus, psycINFO, ProQuest ERIC, LILACS, Google Scholar, Google, The British Library catalogue, ProQuest Dissertation, Open-Grey, New York academy of Medicine's grey literature, National Collaborative center for public health, OAIster, Health Canada, and Global Health Fellowships.org. Two databases planned for inclusion in our search were no longer accessible by our group at the time of the search, Sociological abstracts and NLM gateway. In addition, we searched reference lists of included articles (see Extended data for full MEDLINE search strategy ^ 12 ^).
Finally, we searched websites of global health and/or international health emergency medicine (EM) fellowship programs identified through the database search and a Google search (2022) with key words global and/or international health, emergency medicine, and fellowship.
Article and website selection & data collection process
A screening checklist was developed and pilot tested by two authors (HK, AM) on 50 citations with three rounds necessary to reach >90% agreement. Articles were then screened independently by two authors (HK, AM) in two stages: titles and abstracts stage 1, and a full-text stage 2.
Discrepancies at each stage were resolved through discussion and involvement of the senior author as needed. A data abstraction form was developed and calibration exercise performed by two authors (HK, AM) to ensure consistency in data extraction. The calibration involved comparison and discussion of completed data abstraction forms for the first five articles. Data extraction was then done in duplicate by the same two authors, and discrepancies resolved through discussion and involvement of the senior author as needed. Information abstracted included population, concept and context characteristics and where applicable study characteristics and outcomes. Population characteristics of interest included: medical doctor (MD) stage and type of EM training. Concept characteristics of interest included: type of fellowship (formal/informal, accredited/not), when established, duration of the fellowship, curriculum, program structure, funding, location/type of GH/internal experience, supervision, number of trainees to date, lessons learnt in development/conduct of GH fellowships and program changes applied to the fellowships over time, fellows experiences, and perceived/known impact on fellows future careers. Context characteristics of interest included: fellowships based in high income country academic institutions. As no included articles reported studies appropriate for risk of bias assessment, risk of bias assessment was not done. Website screening was conducted in one stage, by two study team members independently (LPR and KG), and data extraction was conducted by KG and verified by LPR.
Synthesis of results
Descriptive synthesis was conducted for all included articles and website data, and is reported narratively and in tabular form (see Table 1, and Extended data table 2 ^ 12 ^).
Results
Literature search
A total of 2957 articles were identified through the database and hand search, and 62 websites were identified through the database and Google search. After duplicates were removed, 2527 titles and abstracts were screened, and 77 articles and 58 websites reviewed in full. A total of eight articles and 43 websites met eligibility criteria ( Figure 1).
Prisma flow diagram.
Characteristics of included articles and websites
Included articles were published between 1997 and 2021, and included six full text articles and two abstracts for which no full text article was available. Half of the articles presented results of survey studies and half were commentaries describing the need for and/or development of global health emergency medicine programs. The four studies conducted surveys, three with the objective of summarizing GHEM fellowship opportunities available in the United States ^ 2, 13, 14 ^ and one examining perceptions of program directors and fellows on whether GHEM fellowships cover core curricular elements outlined in the literature ^ 5 ^. All other included articles are commentaries describing the need for and/or the components of existing GHEM fellowships. Characteristics of one singular fellowship were described by three of the eight included articles; the remaining five articles summarize the state of GHEM fellowships in general or characteristics of multiple fellowships. All fellowships described or included in these eight articles originate in North America; one fellowship is based in Canada while all others are based in the United States. Similarly, with the exception of one program based in Canada, all included websites provided information on programs based in the United States.
Review findings
** Program establishment, length, structure, funding, curriculum. ** Date of program establishment was provided by three articles and 16 websites. Program establishment dates ranged from 1994 to 2018, with only three established before 2000, seven established between 2000–10 and eight established between 2011–18 respectively.
Program length was reported in five of the included articles, with four ranging from 1–2 years ^ 6, 7, 13, 15 ^ and one, open to both pediatric and general EM-trained fellows, is 3–4 years long ^ 16 ^. All program websites reported program length which ranged from 12 to 26 months, with the majority of programs 2 years in length and the majority of (18 of 19) 1 year programs only available for fellows having previously obtained an appropriate advanced degree ^ 12 ^.
Half of the articles included describe the funding structure of the fellowship program(s). Most programs require fellows to work a certain number of clinical hours to fund their fellowship activities/salary ^ 2, 15, 16 ^. The description of the 3–4 year fellowship mentions financial support provided from the hospital department ^ 16 ^. One fellowship is described as self-funded by the fellow ^ 6 ^. Findings from the program website review were similar to the published articles, with 41 of 43 websites noting funding through clinical work ^ 12 ^. Provision of stipends or coverage of education costs such as tuition and travel, was noted in 16 websites ^ 12 ^.
Generally, programs align with the curriculum areas described by the Society for Academic Emergency Medicine (SAEM), which outlines three areas in which fellows should gain skills in at least one, in addition to clinical skills: administration, education, and research. Though the activities that fellows participate in under each vary, all fellowships discussed in the included articles mentioned fellows’ participating in all areas. The majority of articles (6/8) mention programs that include working towards a Master of Public Health degree as either a mandatory or optional route to fulfill the education component. This is sometimes supplemented with global health courses and/or journal clubs and other informal learning opportunities ^ 2, 6, 7, 13, 14, 16 ^. Similarly, all websites outline curriculum aligning with SAEM recommendations ^ 12 ^. The vast majority of programs require completion of a masters degree (37/43) (most commonly a master of public health) as part of 2 year programs unless an appropriate degree has been previously completed, with completion of masters degree an option in the remaining 2 year programs ^ 12 ^.
** Global health/international experience and fellow supervision. ** All fellowships described in these articles include an international fieldwork component, though the duration and nature of the fieldwork varies. The shortest duration reported is 2 weeks while the longest is 52 weeks ^ 13 ^. Fieldwork opportunities are mostly described as flexible, with opportunities to attach to ongoing international projects that the program is engaged in, or develop their own fieldwork experience based on the fellow’s existing relationships. The majority of programs (32/43) require an international fieldwork component, with eight programs noting international experience options but without clarity in whether this is a requirement ^ 12 ^. As noted in the published articles, fieldwork opportunities described on program websites vary widely in duration (2 to 12 months), and focus (clinical, research, education), although the majority include clinical work as part of the international experience ^ 12 ^. Established international partnerships were noted by 22 programs, with several noting that other international sites may be considered ^ 12 ^.
Only two articles discuss supervision of fellows ^ 6, 16 ^. Both describe faculty mentorship at the fellow’s home institution. In addition, Crouse mentions that fellows are paired with a local supervisor during their fieldwork while maintaining regular contact with their faculty mentor at their home institution ^ 16 ^. As with the published articles, supervision is infrequently discussed in program websites, with eight noting supervision/mentorship to be provided by local faculty with appropriate expertise, and none clearly outlining on-site supervision during international fieldwork ^ 12 ^.
** Number of trainees to date. ** The total number of GHEM fellowship trainees to date was noted by two included articles and ranged from 0–7 at the time of publication ^ 2, 16 ^. Similar to the published articles, few programs reported information on the number of trainees to date, with numbers ranging from 2–31 for the three programs reporting totals ^ 12 ^.
** Fellows’ experiences in the program, perceived impacte on fellows careers. ** The articles did not discuss graduates’ career trajectories in-depth, however two studies ^ 2, 13 ^ surveyed participants to find out where graduates were working following their fellowships. Bledsoe found that out of a total of 29 graduates of international emergency medicine (IEM) fellowships identified, all remain active in international medicine, however it is unclear whether the author interviewed the graduates to obtain this information, or received this information from programs ^ 2 ^. Klesick received information from the fellowship programs, stating that 59% of graduates were working in US academic centers; 24% were working in US community practice settings, 9% were working for nonprofit agencies, and 9% were working in international clinical practice ^ 13 ^. Only one website provides information on graduates career trajectories, noting that three graduates work in academic pediatric emergency medicine global health programs and are engaged in international work ^ 12 ^. Quotes from graduates regarding specific activities undertaken and lessons learnt during their fellowship training were included in two websites. While quotes were quite positive there are too few to draw meaningful conclusions about fellows’ experiences.
** Lessons learned in development/conduct of GH fellowships overtime; program changes over time. ** Half of the included articles (4/8) identified several salient lessons from their experience either directly participating in an existing GHEM fellowship or evaluating the landscape of GHEM fellowships. All noted that the available GHEM fellowships at the time of their writing were considerably varied; the global health emergency medicine field is vast, and fellows are presented with many different foci within the field (e.g., disaster medicine, humanitarian relief, developing emergency systems, public health, and others). The authors note that this variability in focus can result in fellows that are not adequately prepared in any area. “Neither program directors (PDs) nor fellows believe that fellows have achieved an adequate level of capacity (minimum score of 3) in any of the six core curriculum components studied: EM systems development, EM education development, humanitarian aid, public health, EMS and disaster medicine. After completing a 1- or 2-year IEM fellowship, it is unlikely that a graduate would master all six core curriculum areas. However, the fact that having an average score of 3 (perfect amount) in any of the six curriculum areas was reported neither by PDs or fellows is an interesting finding which begets the question whether IEM fellowship are trying to achieve ‘too much’, stacking the deck with more core competencies than they can achieve within the allocated time frame” ^ 5 ^.
Crouse notes that a significant challenge can lie in establishing a sustainable funding structure, in an era of reduced grant funding and smaller operating margins for academic institutions ^ 16 ^. Ensuring that a fellowship program is supported from within the institutions, philosophically and financially, is vital to ensuring the long-term health of the fellowship.
None of the include articles reported changes to the program overtime. Similarly, none of the websites discussed lessons learned or changes to programs overtime.
Discussion
The goal of this scoping review was to summarize components of existing global health emergency medicine fellowship programs and lessons learnt by developers, faculty and trainees in these programs. Our findings revealed some information on the structural components of the fellowship programs such as duration, supervision, funding structure, and broad curricular elements. Notably, though, our review revealed that the experience of developers, faculty and trainees of existing global health emergency medicine fellowship programs have not been rigorously reported in the literature. Data on the experiences of trainees, details of trainees’ international exposure, and program outcomes is lacking in the literature. This poses a challenge for institutions attempting to develop global health emergency medicine fellowship programs as the literature excludes experiential lessons that could be applied to improve new and existing programs.
Fellowship structure
There is discussion in the literature around the appropriate design of a global health emergency medicine fellowship. Specifically, the discourse centered on whether fellowships should have standardized vs. flexible curricula, and exposure-based (exposure to all pre-defined curricular components) vs. proficiency-based (focus on select curricular components) curricula ^ 5 ^. Additionally, the literature revealed that many trainees are not actually aware of fellowship curricula prior to starting a program ^ 5 ^. Given the diverse motivations of trainees completing global health emergency medicine fellowships, a one size fits all approach may not be appropriate. Anderson et al. described that “fellowship programs are most useful when they are flexible in accommodating individual backgrounds and needs” ^ 15 ^. As such, fellowship programs may benefit from developing specific curricular goals in collaboration with individual trainees. Although this process may prove to be more resource intensive, it may lead to improved outcomes for trainees and programs.
Trainee experiences
The literature is lacking an account of trainee experiences in global health emergency medicine fellowship programs. Only three of the eight articles included and one of the websites in this review reported fellowship graduates’ career trajectories. This is a critical piece of data that should be better documented to assess the impact of fellowship training programs. Additionally, it would be important to learn from trainees whether the skills, exposure, and knowledge they gained from their fellowships proved beneficial in their future roles and whether there are aspects of training provided by existing programs that could be improved.
Fellowship challenges
The most frequently described challenges in initiating and maintaining global health emergency medicine fellowships outlined in the literature were: (a) lack of stable funding, (b) scarcity of international partnerships, (c) challenges with fellow supervision on international experiences, and (d) low levels of institutional support. All articles and websites included in this review that provided information on funding models described that trainees were financially supported by revenue from their clinical work, project-specific grants, and in rare cases institutional funds. An understanding of programs and fellows’ experiences would provide greater appreciation for the benefits and drawbacks of the various funding models. While 22 websites note ongoing international relationships which provide fieldwork opportunities to trainees, relatively little detail is provided about the fieldwork experiences of trainees to date, such as knowledge and skills acquired. Additionally, although adequate support and supervision are essential to optimizing fieldwork experiences, data on supervision is largely omitted from the data sources reviewed. Institutions offering global health emergency medicine fellowships should initiate, foster, and sustain partnerships with organizations in low- and middle-income countries to allow for an organized and sustainable exchange of knowledge and resources. Given trainees’ increasing interest in global health emergency medicine, it is surprising to see a lack of institutional support described as one of the challenges in initiating and maintaining such fellowships. Future work should define the types of institutional support required to succeed.
Strengths
This scoping review employed a rigorous and systematic methodology, was prospectively registered, and used predetermined inclusion and exclusion criteria. Additionally, the review employed a broad search strategy, which included a search of grey literature sources and program websites, and a search update to identify all relevant studies.
Limitations
The main limitation of this review is the lack of reporting of evaluation of existing programs and sharing of lessons learnt to date. As a result, data for some areas of interest were not available or lacked the detail necessary to draw meaningful conclusions. Such detail may have been gained through direct contact with programs, to interview program staff and review departmental reports related to concepts of interest. Future work to address these gaps through mixed methods research with program developers, faculty and trainees, to understand experiences and impacts on fellows’ careers to inform program improvements to optimize program benefits to fellows and support continued growth of GHEM as a subspecialty, is needed.
Conclusions
Despite significant interest in advanced global health training among emergency medicine trainees and practitioners and the growth in availability of GHEM fellowships in recent decades, this review highlights that information to guide development and implementation of such programs is limited. Future work to learn from the experiences of program developers, faculty and trainees to date, including gaps in training and impacts of current training on future career trajectories is needed to inform program improvements to optimize the benefits of GHEM fellowship training to trainees and to advance the GHEM as a subspecialty.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Colleges A.o.A.M: Medical School Graduation Questionnaire: 1984 All Schools Summary Report.AAMC: Washington, D.C,1984.
- 2Bledsoe GH Dey CC Kabrhel C : Current status of International Emergency Medicine fellowships in the United States. Prehosp Disaster Med. 2005;20(1):32–5. 10.1017/s 1049023 x 00002119 15748012 · doi ↗ · pubmed ↗
- 3Nelson B Izadnegahdar R Hall L : Global Health Fellowships: A National, Cross-Disciplinary Survey of US Training Opportunities. J Grad Med Educ. 2012;4(2):184–9. 10.4300/JGME-D-11-00214.1 23730439 PMC 3399610 · doi ↗ · pubmed ↗
- 4Alagappan K Holliman CJ : History of the development of international emergency medicine. Emerg Med Clin North Am. 2005;23(1):1–10. 10.1016/j.emc.2004.09.013 15663970 · doi ↗ · pubmed ↗
- 5Jacquet GA Bayram JD Ewen WB : Improving knowledge and process for international emergency medicine fellowship applicants: a call for a uniform application. Emerg Med Int. 2013;2013:737391. 10.1155/2013/737391 23533764 PMC 3594982 · doi ↗ · pubmed ↗
- 6Van Rooyen MJ Townes DA Hart RG : International Health Fellowship: a proposed curriculum for emergency physicians. J Emerg Med. 1997;15(2):249–52. 10.1016/s 0736-4679(96)00352-6 9144072 · doi ↗ · pubmed ↗
- 7Collier A Bartels SA Messenger DW : MP 21: Global emergency medicine fellowship: establishing a global EM training program at Queen's University. Canadian Journal of Emergency Medicine. 2018;20(S 1):S 47–S 48. 10.1017/cem.2018.175 · doi ↗
- 8Peters MD Godfrey CM Khalil H : Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13(3):141–6. 10.1097/XEB.0000000000000050 26134548 · doi ↗ · pubmed ↗