Lifestyle Behavioral Self-Care Practices and Their Determinants Among Type 2 Diabetes Patients Attending a Non-communicable Disease Clinic in Agra District: A Cross-Sectional Study
Dhiraj Singh, Himalaya Singh, Manisha M Nagargoje, Purnoor Kaur, Sarvesh Kumar, Suvit S Sengar

TL;DR
This study examines lifestyle self-care practices among type 2 diabetes patients in Agra, finding that many have poor self-care habits, especially in physical activity and foot care.
Contribution
The study identifies sociodemographic predictors of poor self-care in type 2 diabetes patients in an Indian setting.
Findings
Only 2.1% of patients engaged in adequate physical activity.
Male gender, lower education, and unemployment were linked to poor self-care.
Urban residence and higher occupational status were associated with better self-care scores.
Abstract
Background: Type 2 diabetes (T2D) requires sustained self-care practices to achieve optimal glycemic control and prevent complications. In India, adherence to diabetes self-management remains suboptimal and is influenced by various sociodemographic and lifestyle behavioral factors. Therefore, the present study aimed to assess lifestyle-related self-care practices among patients with T2D attending a non-communicable disease (NCD) clinic in Agra District and to examine their association with sociodemographic characteristics. Materials and methods: A cross-sectional study was conducted among 340 patients with T2D aged 30-60 years who attended the NCD clinic at District Hospital in Agra from May to October 2024. Using systematic random sampling, data were collected through a semi-structured questionnaire based on the modified Summary of Diabetes Self-Care Activities tool, adapted to the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
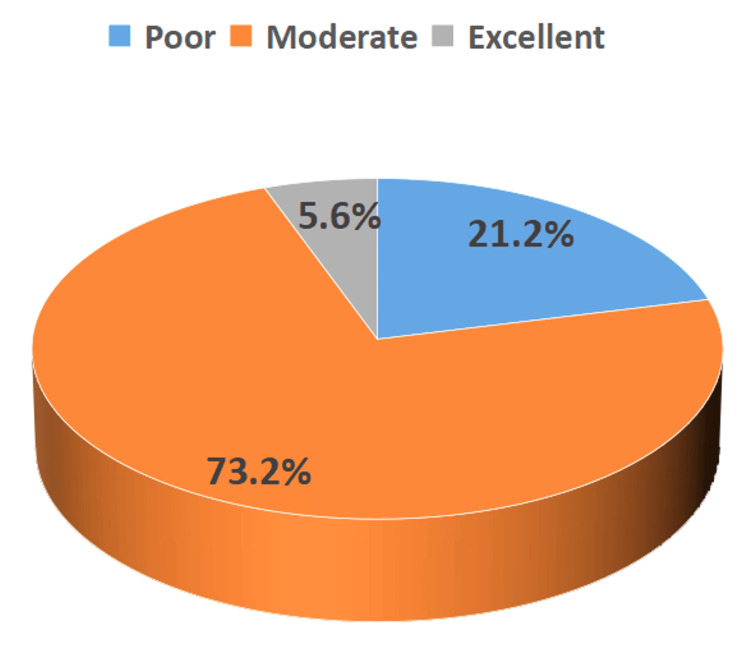 Figure 1
Figure 1| Domain | Parameters | Minimum | Maximum |
| Physical activity | Level of physical activity | 2 | 8 |
| Weekly physical activity (minutes) | |||
| Sedentary behavior | |||
| Diet | Daily fruit consumption | 1 | 4 |
| Daily meal frequency | |||
| Foot care | Daily foot inspection | 0 | 1 |
| Addiction | Alcohol consumption in the last month | 0 | 4 |
| History of alcohol consumption | |||
| Smoking tobacco usage | |||
| Chewing tobacco usage | |||
| Total | 3 | 17 |
| Sociodemographic characteristics | Category | Frequency n = 340 (%) |
| Mean age in years | 51.3 ± 10.6 | |
| Sex | Female | 192 (56.5) |
| Male | 148 (43.5) | |
| Age groups in years | 30-45 | 75 (22.1) |
| 46-60 | 219 (64.6) | |
| >60 | 46 (13.3) | |
| Married status | Single/divorced/widowed | 38 (11.3) |
| Married | 302 (88.7) | |
| Educational status | Illiterate | 118 (34.7) |
| Up to high school | 134 (39.5) | |
| Intermediate and above | 88 (25.8) | |
| Residence | Rural | 84 (24.7) |
| Urban | 256 (75.3) | |
| Head of family | Self | 196 (57.6) |
| Spouse | 133 (39.1) | |
| Others | 11 (3.3) | |
| Occupation | Employed | 51 (15) |
| Unemployed | 289 (85) | |
| Socioeconomic status (modified BG Prasad socioeconomic classification) | Upper | 28 (8.3) |
| Upper middle | 72 (21.2) | |
| Middle | 104 (30.5) | |
| Lower middle | 97 (28.5) | |
| Lower | 39 (11.5) | |
| Lifestyle behavior self-care parameters (study participants = 340) | Score 0 response (n, %) | Score 1 response (n, %) | Score 2 response (n, %) | Score 3 response (n, %) | Score 4 response (n, %) |
| Level of physical activity (score 0 - mild activity/walking, score 2 - vigorous activity) | 338 (99.4) | - | 2 (0.6) | - | - |
| Weekly physical activity (score 1 - <75 minutes, score 2 - 75-150 minutes, score 3 - >150 minutes) | - | 331 (97.4) | 7 (2.1) | 2 (0.6) | 00 (0) |
| Sedentary behavior (score 0 - yes, score 1 - no) | 265 (77.9) | 75 (22.1) | - | - | - |
| Daily fruit consumption (score 0 - none, score 1 - ≥1 serving) | 271 (79.7) | 69 (20.3) | - | - | - |
| Daily meal frequency (score 1 - 3 meals/day, score 2 - 3-5 meals/day, score 3 - >5 meals/day) | - | 332 (97.6) | 1 (0.3) | 7 (2.1) | - |
| Daily foot Inspection (score 0 - no, score 1 - yes) | 76 (22.4) | 264 (77.6) | - | - | - |
| Alcohol consumption in the last month (score 0 - yes, score 1 - no) | 39 (11.5) | 301 (88.5) | - | - | - |
| History of alcohol consumption (score 0 - yes, score 1 - no) | 52 (15.3) | 288 (84.7) | - | - | - |
| Smoking tobacco usage (score 0 - yes, score 1 - no) | 47 (13.8) | 293 (86.2) | - | - | - |
| Chewing tobacco usage (score 0 - yes, score 1 - no) | 98 (28.8) | 242 (71.2) | - | - | - |
| Mean self-care score = 7.45 + 1.49, min = 3, max = 17, range = 14 | |||||
| Sociodemographic characteristics N = 340 | Self-care practices | COR (95% CI) | p-value | |||
| Poor self-care score <7.0 | Good self-care score ≥7.0 | |||||
| Age | 30-45 years | 16 (21.3) | 59 (78.7) | 1 | 0.052 | |
| 46-60 years | 53 (24.2) | 166 (75.8) | 1.177 (0.625-2.217) | |||
| >60 years | 3 (6.7) | 42 (93.3) | 0.263 (0.072-0.962) | |||
| Sex | Male | 53 (35.8) | 95 (64.2) | 1 | <0.001 | |
| Female | 19 (9.9) | 173 (90.1) | 0.197 (0.110-0.352) | |||
| Educational status | Up to primary school | 4 (10.5) | 34 (89.5) | 1 | 0.02 | |
| Up to high school | 15 (13.0) | 100 (87.0) | 1.275 (0.396-4.106) | |||
| Intermediate and above | 53 (28.3) | 134 (71.7) | 3.362 (1.137-9.937) | |||
| Residential status | Rural | 24 (28.9) | 59 (71.1) | 1 | 0.031 | |
| Urban | 47 (18.4) | 209 (81.6) | 0.533 (0.313-0.978) | |||
| Head of the family | Self | 55 (28.1) | 141 (71.9) | 1 | <0.001 | |
| Spouse/other | 17 (11.8) | 127 (88.2) | 0.343 (0.189-0.622) | |||
| Occupation | Employed | 2 (3.9) | 49 (96.1) | 1 | 0.019 | |
| Unemployed | 70 (24.2) | 219 (75.8) | 7.831 (1.857-33.029) | |||
| Variables | 95% CI | |||||||||
| B | S.E. | Wald | Df | Sig. | aOR | Lower | Upper | |||
| Age | ||||||||||
| 30-45 years | - | - | 4.444 | 2 | 0.108 | - | - | - | ||
| 46-60 years | 0.168 | 0.376 | 0.198 | 1 | 0.656 | 1.182 | 0.566 | 2.472 | ||
| >60 years | -1.21 | 0.710 | 2.887 | 1 | 0.089 | 0.299 | 0.074 | 1.204 | ||
| Sex (male vs. female) | -1.57 | 0.417 | 14.16 | 1 | 0.000 | 0.209 | 0.092 | 0.472 | ||
| Residential status (rural vs. urban) | -0.513 | 0.337 | 2.313 | 1 | 0.128 | 0.599 | 0.309 | 1.160 | ||
| Educational status | ||||||||||
| Up to primary school | - | - | 17.503 | 2 | 0.000 | - | - | - | ||
| Up to high school | 1.971 | 0.587 | 11.286 | 1 | 0.001 | 7.180 | 2.273 | 22.678 | ||
| Intermediate and above | 1.100 | 0.354 | 9.661 | 1 | 0.002 | 3.004 | 1.501 | 6.012 | ||
| Head of the family (self vs. others) | -0.151 | 0.430 | 0.124 | 1 | 0.725 | 0.860 | 0.370 | 1.996 | ||
| Occupation (employed vs. unemployed) | 1.803 | 0.769 | 5.495 | 1 | 0.019 | 6.066 | 1.344 | 27.384 | ||
| Constant | -3.300 | 0.988 | 11.150 | 1 | <0.001 | 0.37 | - | - | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Management and Education · Medication Adherence and Compliance · Nursing care and research
Introduction
Self-care practices play a pivotal role in the management of type 2 diabetes (T2D). As a chronic condition, T2D requires ongoing attention to lifestyle, diet, and medication adherence to prevent complications and maintain optimal glycemic control. Effective self-care is essential for improving quality of life and reducing the risk of complications such as cardiovascular disease, neuropathy, and nephropathy [1]. Understanding the determinants of self-care behaviors among individuals with T2D can inform healthcare strategies to improve patient outcomes. Self-care in T2D encompasses a range of activities, including blood glucose monitoring, adherence to prescribed medications, physical activity, healthy eating, and regular foot care [2,3].
A variety of factors influence self-care behaviors among people with T2D. These determinants broadly fall into individual, interpersonal, and systemic domains. At the individual level, demographic factors such as age, gender, and education, along with psychological factors including self-efficacy and health literacy, play a substantial role [4]. Studies have shown that higher self-efficacy is associated with better adherence to self-care behaviors, underscoring the importance of patients’ confidence in managing their condition [5]. Likewise, health literacy, the ability to obtain, process, and understand essential health information, is a critical determinant of effective diabetes self-management [6]. Interpersonal factors, including social support from family members, peers, and healthcare providers, further influence self-care practices. Evidence suggests that individuals who receive emotional and practical support are more likely to engage in health-promoting behaviors [7]. The role of healthcare providers in delivering tailored education and guidance is equally important, as diabetes self-management education and support programs have been shown to enhance patients’ self-care capabilities significantly [8].
Given the multifaceted nature of these determinants, a comprehensive understanding of the factors influencing self-care is crucial for designing effective interventions. Tailored approaches that address individual, interpersonal, and systemic barriers are necessary to promote sustainable self-care practices among individuals with T2D [9]. In India, the Ministry of Health and Family Welfare has launched a national program to prevent and control non-communicable diseases (NCDs), including diabetes, through the "National Programme for Prevention and Control of Non-Communicable Diseases" [10]. While the program emphasizes early diagnosis, it places limited focus on self-care practices among diabetic patients. Given the high reliance on the public healthcare system, understanding existing self-care behaviors is essential yet remains underexplored in Indian settings [10-12].
Against this backdrop, the present study assessed lifestyle-related self-care practices, including diet, physical activity, and foot care, among adults with T2D attending an NCD clinic and examined their association with sociodemographic characteristics. The findings will generate evidence to support program managers in understanding the epidemiological distribution of lifestyle self-care practices in diabetes management and identifying patient-level barriers to their adoption.
Materials and methods
Study design and setting
The present cross-sectional study was conducted under the Department of Community Medicine, Government Medical College, Agra, to assess self-care practices among individuals with T2D attending the NCD clinic (Table 1). The single NCD clinic in Agra, located at District Hospital, was selected as the study site.
Study population
The study population comprised all T2D patients who attended the NCD clinic at District Hospital in Agra between May and October 2024. Adults aged ≥30 years who had been diagnosed with T2D and were undergoing diabetes treatment for at least one year were included in the study [11]. Patients with other types of diabetes or gestational diabetes, those with cognitive impairment, and those unable or unwilling to participate were excluded.
Sampling size and sampling procedure
The sample size was calculated using the single-population proportion formula. Assuming a 5% margin of error, a 95% confidence interval (CI), a 5% non-response rate, and using the proportion of diabetes self-care practice (46.7%) reported in a previous study from the Tigray region [12], the final sample size was determined to be 340. Study participants were selected using systematic random sampling. Each OPD day at the NCD clinic, the first participant was selected by lottery, and every 3rd eligible participant thereafter was included, based on an estimated daily attendance of approximately 60 diabetes patients. This process continued until the required sample size was achieved.
Data collection procedure
Data were collected daily at the NCD clinic by a single interviewer using the sampling procedure until the required sample size was achieved. A pre-tested, semi-structured, interviewer-administered questionnaire was used to collect information from diabetic patients attending the clinic for routine medical check-ups.
The questionnaire consisted of two sections. The first section collected sociodemographic information, including age, gender, marital status, education, and socioeconomic status, classified using the modified BG Prasad scale, updated for February 2024 [13]. All data were recorded using standardized formats, and participants were assigned numerical identifiers to ensure anonymity and confidentiality.
The second section assessed lifestyle-related self-care practices specific to diabetes across four domains: physical activity, diet, foot care, and addiction. These domains were selected based on established evidence linking them to improved glycemic outcomes [14].
Ten pre-tested items corresponding to these domains were included in a principal component analysis, which yielded a four-component structure. Sampling adequacy was acceptable (KMO = 0.587), and Bartlett’s test of sphericity was significant (p < 0.001), confirming that the data were suitable for factor extraction. The extracted components demonstrated adequate communalities and clear, interpretable loadings.
Each item was scored on a scale from 0 to 4, where a score of "0" indicated no engagement and higher scores (up to 4) reflected greater adherence to the specific self-care behavior. This scoring approach enabled more nuanced quantification of adherence than a simple binary classification. Item scores were summed across the four domains to generate a cumulative self-care score for each participant.
Total scores were then dichotomized at the sample mean to classify participants into two categories: good self-care (scores above the mean) and poor self-care (scores at or below the mean). This method provided a standardized and interpretable classification for comparing self-care practices within the study population.
Data management and analysis
To ensure data quality and questionnaire alignment with the study objectives, a pretest was conducted on 5% of the total sample of patients attending diabetes clinics at a tertiary-level teaching hospital that was not selected as the study site. During data management, storage, and analysis, all collected data were thoroughly checked for accuracy and consistency. Data were entered into Microsoft Excel (Microsoft Corp., Redmond, WA, USA) and analyzed using Epi-Info version 7.2.6.0 (Centers for Disease Control and Prevention, Atlanta, GA, USA). Categorical variables were presented as proportions, while continuous variables were summarized using mean, standard deviation (SD), median, and interquartile range (IQR). Univariate and multivariate logistic regression analyses were performed to identify associated risk factors, and adjusted odds ratios (AORs) with 95% CI were reported. A p-value of <0.05 was considered statistically significant.
Study variables
Sociodemographic factors included age, sex, place of residence, educational status, occupation, marital status, religion, and estimated monthly income. Behavioral factors included a history of smoking, alcohol consumption (lifetime use), and engagement in physical activity.
Ethical considerations
Ethical approval for the study was obtained from the Institutional Review Board of S. N. Medical College, Agra (approval number: SNMC/IEC/2024/204, dated February 2, 2024). Permission to conduct the research was also secured from the relevant health institution. Written informed consent was obtained from all participants, and anonymity was ensured by assigning non-identifiable codes.
Results
Sociodemographic characteristics of study participants
Table 2 shows that among the 340 study participants, the mean age was 51.3 ± 10.6 years. The largest proportion (64.6%) was aged 46-60 years, followed by 22.1% aged 30-45 years and 13.3% aged 60 years and older. Females comprised 56.5% of the sample, and males 43.5%, with 88.7% of participants married. Regarding educational status, 39.5% had completed high school, while 34.7% were illiterate. Most participants (75.3%) resided in urban areas. In terms of family leadership, 57.6% of households were headed by the participant themselves ("self"), and the spouse headed 39.1%. According to the modified BG Prasad socioeconomic classification (2024), 30.5% of participants belonged to the middle class, 28.5% to the lower middle class, and 21.2% to the upper middle class, while the upper class and lower class each accounted for less than 12% of the population.
Lifestyle behavior, self-care practices, and their association with sociodemographic characteristics among study participants
Among the 340 study participants, the majority (73.2%) demonstrated moderate self-care practices (scores between 50 and 70%). In contrast, only 5.6% exhibited excellent self-care, and 21.2% fell into the poor self-care category (scores <50%), as illustrated in Figure 1. Table 3 shows that the overall mean self-care score was 7.45 ± 1.49, with a range of 3-17, indicating suboptimal engagement in self-care among the surveyed T2D patients.
Distribution of lifestyle behavior self-care score among T2D patients attending the NCD clinic at District HospitalAs per the Summary of Diabetes Self-Care Activities questionnaire.Poor self-care practices: <50%, moderate self-care practices: 50-70%, excellent self-care practices: >70%T2D: type 2 diabetes, NCD: non-communicable disease
Regarding physical activity, almost all participants (99.4%) reported only mild activity or walking, with a negligible proportion (0.6%) engaging in vigorous activity. Most participants (97.4%) performed less than 75 minutes of physical activity per week, substantially below the recommended 150 minutes of moderate-intensity aerobic activity; only 0.6% met the 150-300 minutes target, and none exceeded 300 minutes. Sedentary behavior was highly prevalent, reported by 77.9% of participants.
Dietary data showed that 79.7% of participants consumed no servings of fruit daily, indicating inadequate intake of essential micronutrients and fiber. While 97.6% adhered to three meals per day, a small proportion (2.1%) consumed more than five meals per day. Foot care practices were suboptimal, with 22.4% of participants not performing daily foot inspections, placing them at risk for diabetic foot complications.
Regarding substance use, 88.5% reported no alcohol consumption in the past month, and 84.7% had no history of alcohol use; however, 11.5% were current drinkers, and 15.3% had a history of alcohol consumption. Tobacco use was notable, with 13.8% smoking and 28.8% using smokeless tobacco.
As shown in Table 4, gender (female), higher educational status (intermediate and above), and employment were significantly associated with better self-care practices (p = 0.000 for gender and education, p = 0.019 for employment).
The multivariate logistic regression analysis presented in Table 5 identified several key sociodemographic factors independently associated with poor self-care among patients with T2D. Educational status emerged as a significant predictor (Wald = 12.239, p = 0.002), with participants having "intermediate and above" education showing 3.36 times higher odds of poor self-care compared to those with "up to primary school" education (aOR = 3.362; 95% CI: 1.137-9.937; p = 0.028). Unemployment was also a significant risk factor, with unemployed individuals having approximately six times the odds of poor self-care compared with employed participants (aOR = 6.066; p = 0.019). Female gender was protective, with females having significantly lower odds of poor self-care than males (aOR = 0.209; p < 0.001).
Conversely, age (p = 0.108), residential status (p = 0.128), and head-of-household status (p = 0.725) were not independently associated with poor self-care in this model. Notably, older age groups (46-60 years and >60 years) were less likely to engage in moderate or excellent self-care than the youngest age group (<30 years), highlighting an important demographic for targeted interventions. Overall, males had significantly lower odds of exhibiting moderate or excellent self-care compared to females.
Discussion
The present study aimed to assess lifestyle and self-care practices among patients with T2D attending the NCD clinic. We found that while 73.2% of participants demonstrated moderate self-care scores, 21.2% fell into the poor self-care category. However, total scores may obscure specific gaps in patient care. Notably, only 2.1% of participants met the recommended physical activity levels of 75-150 minutes per week, which is concerning given that both Colberg et al. [12] and the WHO [13] emphasize regular exercise as essential for glycemic control and cardiovascular health in T2D.
Foot care was another area of significant concern. In our study, 77.6% of participants did not perform daily foot inspections. As noted by Boulton et al. [15], neglecting daily foot checks represents a missed opportunity to prevent complications, particularly in the context of diabetic neuropathy. This finding aligns with a study from Eastern India by Mitra et al. [16], which reported that 79% of patients had poor knowledge regarding foot care. Dietary practices were similarly suboptimal, with only 20.3% of participants consuming the recommended 400 g of fruits and vegetables per day, as advised by the WHO [17]. This finding is consistent with the Chennai Urban Rural Epidemiology Study by Radhika et al. [18], which identified cost and misconceptions as common barriers to adequate fruit and vegetable intake among Indian patients.
To explore factors influencing self-care, we dichotomized the "self-care score" (range: 3-13) using a mean split (cutoff ≥7.0) to classify participants as having either "good" or "poor" self-care. This approach was chosen because the data are non-normally distributed and allows the calculation of odds ratios for associated risk factors. This methodology aligns with recent diabetes studies, such as Dedefo et al. [19], and is consistent with the scale guidelines from Toobert et al. [14], facilitating clinically meaningful interpretation of the results.
Our multivariate analysis identified male gender, lower education, and unemployment as significant predictors of poor self-care. The association between lower education and suboptimal self-care is likely mediated by reduced health literacy, which can make it more difficult for patients to comprehend and adhere to complex instructions regarding diet and medication. These findings align with the Lancet Commission on Diabetes framework proposed by Chan et al. [20], which identifies economic instability as a key driver of inadequate diabetes management. Similarly, the ICMR-INDIAB study by Anjana et al. [21] demonstrated that diabetes outcomes in India are closely linked to socioeconomic status. Interestingly, we did not observe significant differences in self-care across religious groups, suggesting that socioeconomic factors, such as education and employment, have a stronger influence on health behaviors than cultural background, a trend also reported by Pradeepa et al. [22].
The study has several strengths, including its robust cross-sectional design and use of systematic random sampling, which helped minimize selection bias. However, reliance on self-reported data introduces potential recall and social desirability bias. The dichotomization of the self-care score simplified data collection and accommodated participants with varying levels of health literacy, albeit at the cost of some statistical precision. This binary format, however, reduced respondent burden and likely improved reporting accuracy. The tool, adapted from the Summary of Diabetes Self-Care Activities, was pretested to ensure clarity and contextual relevance. Limitations include the single-center setting, which may overrepresent urban patients and limit generalizability, and the exclusive focus on sociodemographic variables without accounting for clinical or psychosocial determinants.
Conclusions
Attendance at the NCD clinic has not translated into adequate adherence to lifestyle-related self-care. Current education on key domains such as physical activity and foot care appears insufficient, particularly for high-risk groups, including men and unemployed individuals. Clinical strategies should move beyond passive knowledge dissemination toward targeted behavioral interventions that address these non-pharmacological aspects of diabetes management. Integrating regular diabetes self-care education with mandatory knowledge assessment during follow-up visits into primary care services may enhance patient comprehension and improve adherence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diabetes self-care activities among patients with type 2 diabetes: a systematic review and meta-analysis Int J Diabetes Dev Ctries Khosravizadeh O Ahadinezhad B Maleki A Yousefy S Momeni Z 1019442024
- 2Self-care: a concept analysis Int J Nurs Sci Martínez N Connelly CD Pérez A Calero P 418425820213463199210.1016/j.ijnss.2021.08.007PMC 8488814 · doi ↗ · pubmed ↗
- 3AADE 7 self-care behaviors Diabetes Educ 4454493420081853531710.1177/0145721708316625 · doi ↗ · pubmed ↗
- 4Factors influencing adherence to self-care practices among patients of type 2 diabetes mellitus from Saurashtra region of Gujarat: a conclusive research J Family Med Prim Care Joshi J Patel P Gandhi S Patel N Chaudhari A 639564011120223661821310.4103/jfmpc.jfmpc_473_22PMC 9810919 · doi ↗ · pubmed ↗
- 5Self-efficacy impact adherence in diabetes mellitus Diabetes Updates DMS ASNM 1312018
- 6The evolving concept of health literacy Soc Sci Med Nutbeam D 207220786720081895234410.1016/j.socscimed.2008.09.050 · doi ↗ · pubmed ↗
- 7Emotional and psychological needs of people with diabetes Indian J Endocrinol Metab Kalra S Jena BN Yeravdekar R 6967042220183029458310.4103/ijem.IJEM_579_17PMC 6166557 · doi ↗ · pubmed ↗
- 8Diabetes self-management education and support in type 2 diabetes: a joint position statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics J Acad Nutr Diet Powers MA Bardsley J Cypress M 1323133411520152605442310.1016/j.jand.2015.05.012 · doi ↗ · pubmed ↗