Association of rheumatoid arthritis with chronic kidney disease
Mathias Ausserwinkler, Andreas Kronbichler, Sophie Gensluckner, Simon Aberger, Bernhard Paulweber, Eugen Trinka, Patrick Langthaler, Bernhard Iglseder, Maria Flamm, Elmar Aigner, Bernhard Wernly

TL;DR
People with rheumatoid arthritis are more likely to have chronic kidney disease, especially with albuminuria, and this may be linked to metabolic issues rather than inflammation alone.
Contribution
Identifies albuminuria at preserved kidney function as the main renal phenotype in RA patients with CKD, independent of inflammation.
Findings
RA patients had higher CKD prevalence compared to controls (11.8% vs 6.7%).
Albuminuria at preserved kidney function was more common in RA patients (6.8% vs 4.2%).
The RA-CKD association was largely explained by metabolic comorbidities rather than inflammation.
Abstract
Rheumatoid arthritis (RA) has been linked to an increased risk of chronic kidney disease (CKD), but the predominant renal phenotype and its independence from established risk factors remain unclear. We examined the RA–CKD association in a large, population-based cohort. RA and CKD were defined using American College of Rheumatology/European Alliance of Associations for Rheumatology and KDIGO criteria. Logistic regression models were employed with stepwise adjustment: first for cardiovascular risk [Systematic COronary Risk Evaluation 2 (SCORE2)], followed by a model including age, sex, metabolic syndrome, smoking status, non-steroidal anti-inflammatory drug (NSAID) use and high-sensitivity C-reactive protein. Interaction terms were tested to evaluate effect modification. Among 9665 participants from the Paracelsus 10,000 cohort, 296 (3.1%) had RA. CKD prevalence was higher in the RA…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
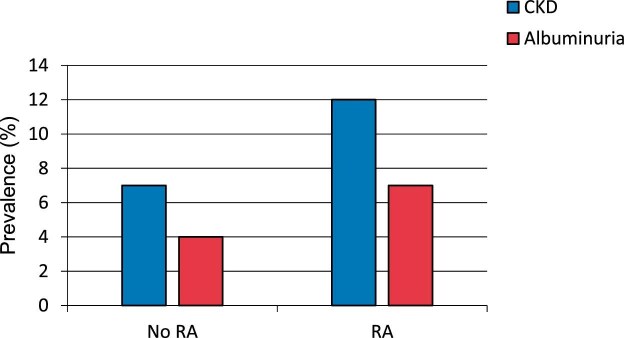 Figure 1
Figure 1| Characteristic | Total ( | No RA ( | RA ( |
|
|---|---|---|---|---|
| Demographics | ||||
| Age (years), median (IQR) | 55 (50–62) | 55 (50–62) | 59 (54–64) | <.001 |
| Age categories, | <0.001 | |||
| <50 years | 2335 (24.2) | 2307 (24.6) | 28 (9.5) | |
| 50–59 years | 4145 (42.9) | 4015 (42.8) | 130 (43.9) | |
| 60+ years | 3185 (33.0) | 3047 (32.5) | 138 (46.6) | |
| Male sex, | 4684 (48.5) | 4588 (49.0) | 96 (32.4) | <.001 |
| Anthropometric measures | ||||
| BMI (kg/m²), median (IQR) | 26.0 (23.0–29.0) | 26.0 (23.0–29.0) | 27.0 (23.0–31.0) | <.001 |
| BMI ≥30 kg/m², | 1853 (19.2) | 1753 (18.7) | 100 (33.8) | <.001 |
| Metabolic parameters | ||||
| Metabolic syndrome, | 2454 (25.4) | 2351 (25.1) | 103 (34.8) | <.001 |
| Abdominal obesity | 4098 (42.4) | 3925 (41.9) | 173 (58.4) | <.001 |
| Elevated triglycerides | 2513 (26.0) | 2429 (25.9) | 84 (28.4) | .34 |
| Low HDL cholesterol | 1016 (10.5) | 976 (10.4) | 40 (13.5) | .084 |
| Elevated blood pressure | 5724 (59.2) | 5530 (59.0) | 194 (65.5) | .029 |
| Elevated glucose | 2607 (27.0) | 2510 (26.8) | 97 (32.8) | .023 |
| Lifestyle factors | ||||
| Smoking status, | 0.040 | |||
| Never smoker | 4106 (44.9) | 3999 (45.4) | 107 (38.1) | |
| Previous smoker | 3369 (36.8) | 3247 (36.9) | 122 (43.4) | |
| Current smoker | 1674 (18.3) | 1623 (18.4) | 51 (18.1) | |
| NSAID use, | 728 (7.5) | 667 (7.1) | 61 (20.6) | <.001 |
| Cardiovascular risk | ||||
| SCORE2 risk, median (IQR) | 4.0 (2.1–6.8) | 4.0 (2.1–6.8) | 4.8 (2.6–7.8) | <.001 |
| Laboratory parameters | ||||
| Creatinine (mg/dL), median (IQR) | 0.8 (0.7–1.0) | 0.8 (0.7–1.0) | 0.8 (0.7–0.9) | <.001 |
| eGFR (mL/min/1.73 m²), median (IQR) | 89 (79–98) | 89 (79–98) | 90 (77–97) | .72 |
| hsCRP (mg/dL), median (IQR) | 0.12 (0.06–0.24) | 0.12 (0.06–0.24) | 0.14 (0.08–0.28) | .002 |
| Medications | ||||
| Antihypertensive therapy, | 1998 (20.7) | 1901 (20.3) | 97 (32.8) | <.001 |
| Statin therapy, | 799 (8.3) | 767 (8.2) | 32 (10.8) | .11 |
| Variable | Multivariable, OR (95% CI) |
| Interaction with RA, OR (95% CI) |
|
|---|---|---|---|---|
| RA | 1.43 (0.96–2.13) | .079 | ||
| Age categories | ||||
| <50 years | Reference | Reference | ||
| 50–59 years | 1.15 (0.88–1.52) | .304 | 2.11 (0.26–17.19) | .487 |
| 60+ years | 2.78 (2.14–3.61) | <.001 | 1.40 (0.18–10.97) | .751 |
| Male sex | 0.90 (0.76–1.07) | .249 | 1.64 (0.79–3.44) | .186 |
| Metabolic syndrome | 2.00 (1.67–2.40) | <.001 | 0.88 (0.42–1.85) | .740 |
| Metabolic syndrome components | ||||
| Abdominal obesity | 0.64 (0.30–1.37) | .252 | ||
| Elevated triglycerides | 1.22 (0.58–2.56) | .596 | ||
| Low HDL cholesterol | 0.59 (0.21–1.65) | .314 | ||
| Hypertension | 1.70 (0.63–4.59) | .299 | ||
| Elevated glucose | 1.00 (0.48–2.08) | .999 | ||
| Smoking status | ||||
| Never smoker | Reference | Reference | ||
| Previous smoker | 0.88 (0.73–1.07) | .208 | 1.17 (0.50–2.73) | .715 |
| Current smoker | 1.16 (0.92–1.47) | .218 | 1.23 (0.44–3.48) | .693 |
| NSAID use | 1.51 (1.16–1.96) | .002 | 0.40 (0.17–0.97) | .042 |
| hsCRP (per unit) | 1.35 (1.19–1.54) | <.001 | 0.99 (0.64–1.53) | .955 |
| Outcome | Total ( | No RA ( | RA ( |
|
|---|---|---|---|---|
| CKD | ||||
| CKD (binary), | 664 (6.9) | 629 (6.7) | 35 (11.8) | <.001 |
| CKD stages (GFR + ACR categories), | 0.006 | |||
| G1A1 (eGFR ≥90, ACR <30) | 4319 (44.7) | 4182 (44.6) | 137 (46.3) | |
| G1A2 (eGFR ≥90, ACR 30–299) | 205 (2.1) | 194 (2.1) | 11 (3.7) | |
| G1A3 (eGFR ≥90, ACR ≥300) | 11 (0.1) | 10 (0.1) | 1 (0.3) | |
| G2A1 (eGFR 60–89, ACR <30) | 4682 (48.4) | 4558 (48.6) | 124 (41.9) | |
| G2A2 (eGFR 60–89, ACR 30–299) | 208 (2.2) | 199 (2.1) | 9 (3.0) | |
| G2A3 (eGFR 60–89, ACR ≥300) | 15 (0.2) | 14 (0.1) | 1 (0.3) | |
| G3aA1 (eGFR 45–59, ACR <30) | 176 (1.8) | 166 (1.8) | 10 (3.4) | |
| G3aA2 (eGFR 45–59, ACR 30–299) | 22 (0.2) | 22 (0.2) | 0 (0.0) | |
| G3aA3 (eGFR 45–59, ACR ≥300) | 2 (0.0) | 2 (0.0) | 0 (0.0) | |
| G3bA1 (eGFR 30–44, ACR <30) | 9 (0.1) | 8 (0.1) | 1 (0.3) | |
| G3bA2 (eGFR 30–44, ACR 30–299) | 5 (0.1) | 5 (0.1) | 0 (0.0) | |
| G3bA3 (eGFR 30–44, ACR ≥300) | 1 (0.0) | 1 (0.0) | 0 (0.0) | |
| G4A1 (eGFR 15–29, ACR <30) | 3 (0.0) | 2 (0.0) | 1 (0.3) | |
| G4A2 (eGFR 15–29, ACR 30–299) | 2 (0.0) | 2 (0.0) | 0 (0.0) | |
| G4A3 (eGFR 15–29, ACR ≥300) | 4 (0.0) | 3 (0.0) | 1 (0.3) | |
| G5A3 (eGFR <15, ACR ≥300) | 1 (0.0) | 1 (0.0) | 0 (0.0) | |
| ACR | ||||
| ACR (mg/g), median (IQR) | 3 (2–7) | 3 (2–7) | 4 (2–9) | .002 |
| ACR categories, | 0.028 | |||
| ACR <30 | 9201 (95.1) | 8927 (95.2) | 274 (92.3) | |
| ACR 30–300 | 443 (4.6) | 423 (4.5) | 20 (6.7) | |
| ACR >300 | 34 (0.4) | 31 (0.3) | 3 (1.0) | |
| Summary patterns | ||||
| Normal kidney function (G1A1 + G2A1) | 9001 (93.1) | 8740 (93.3) | 261 (88.2) | <.001 |
| Albuminuria at preserved GFR (G1A2 + G2A2) | 413 (4.3) | 393 (4.2) | 20 (6.8) | .027 |
| Reduced GFR (G3a–G5) | 225 (2.3) | 211 (2.3) | 14 (4.7) | .005 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRheumatoid Arthritis Research and Therapies · Chronic Kidney Disease and Diabetes · Gout, Hyperuricemia, Uric Acid
INTRODUCTION
Chronic kidney disease (CKD) and rheumatoid arthritis (RA) are highly prevalent conditions that contribute substantially to the global burden of disease [1–4]. CKD affects approximately 10% of the adult population and is a major driver of cardiovascular events, reduced quality of life and healthcare costs [5]. RA is a chronic autoimmune disease characterized by systemic inflammation and a high burden of comorbidity, including stroke, ischemic heart disease and kidney complications [6–8].
Growing evidence suggests that RA is independently associated with an increased risk of CKD and that higher RA disease activity is associated with accelerated eGFR decline and increased risk of clinically relevant kidney dysfunction [9]. Large population-based cohort studies have consistently demonstrated that RA patients are more likely to develop CKD compared with the general population, even after adjustment for established risk factors such as hypertension, diabetes and dyslipidemia. For instance, a nationwide cohort analysis reported a 31% increased risk of CKD among RA patients. Furthermore, Mendelian randomization data support a direct causal relationship, indicating that genetically determined RA increases the risk of CKD, kidney failure and related complications [10].
Mechanistically, the association is likely multifactorial. Chronic systemic inflammation, central to RA pathogenesis, is known to cause endothelial dysfunction, glomerular injury and kidney fibrosis [11]. Elevated high-sensitivity C-reactive protein (hsCRP) levels and high RA disease activity have been independently linked to accelerated kidney function decline. Additionally, extra-articular kidney disease (e.g. glomerulonephritis, amyloidosis) and potentially nephrotoxic medications such as non-steroidal anti-inflammatory drugs (NSAIDs) or certain disease-modifying agents contribute to development of CKD in RA [9, 12]. On the other hand, biologic agents that reduce systemic inflammation may attenuate this risk [13].
However, the extent to which RA increases CKD risk independently of established risk factors, systemic inflammation and medication exposures remains uncertain. Moreover, a paucity of data exists on potential interactions between RA and the above-mentioned risk factors, modification of the risk by inflammation levels or medication exposures. Using a large population-based cohort with comprehensive metabolic and inflammatory profiling, we examined whether the RA-CKD association is mediated by systemic inflammation and modified by antirheumatic therapy. Specifically, we investigated potential interactions between RA and traditional risk factors, inflammatory markers and medication exposures.
MATERIALS AND METHODS
Study population
This retrospective study used data from the Paracelsus 10,000 cohort, a population-based observational study conducted in Salzburg, Austria. The cohort consisted of participants aged 40–77 years who underwent baseline assessments between April 2013 and March 2020 [14]. Recruitment aimed to randomly select individuals from the Austrian national registry of residents, with approximately 56 600 invitation letters sent out, resulting in 10 044 participants being examined. For this analysis, we included 9665 participants with complete information on RA diagnosis and kidney function parameters. Individuals diagnosed with RA were identified based on American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/EULAR) classification criteria, requiring a total score of 6 or more out of 10 points across four key domains [15]. After this assessment detailed rheumatologic phenotyping beyond case classification was not available in the Paracelsus 10,000 dataset. In particular, we did not have information on RA disease duration, composite disease activity scores or serostatus (rheumatoid factor and anti-citrullinated protein antibodies) for each single case. We also did not capture exposure to disease-modifying antirheumatic drugs (DMARDs). The control group comprised individuals without RA from the cohort, excluding patients with chronic inflammatory bowel diseases and other rheumatic diseases [2, 14, 16, 17].
Clinical assessments
All participants underwent standardized clinical, laboratory and imaging assessments. Blood samples were collected after an overnight fast for analysis of lipid profiles, glucose metabolism markers (fasting glucose and HbA1c), inflammatory markers (hsCRP) and kidney function parameters. Anthropometric measurements included body mass index and waist circumference. Blood pressure was measured bilaterally in a seated position, repeated three times per side after a 60-s resting interval. Participants completed structured interviews capturing personal medical history, medication use and lifestyle factors including smoking and alcohol consumption. The study collected data on medications addressing cardiovascular and metabolic risk factors, including antihypertensives, diabetes treatments, statins and NSAIDs.
Kidney function assessment
CKD was defined according to KDIGO guidelines as an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m² or albumin–creatinine ratio (ACR) ≥30 mg/g creatinine. eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration 2009 equation based on serum creatinine levels. CKD staging was performed according to the KDIGO classification system combining CKD stages, eGFR categories (G1–G5) with albuminuria categories (A1–A3). Albuminuria was assessed using spot urine samples and categorized as A1 (ACR <30 mg/g), A2 (ACR 30–299 mg/g) or A3 (ACR ≥300 mg/g) [8].
Statistical analysis
Continuous variables were expressed as median and interquartile range and compared using the Wilcoxon rank-sum test. Categorical data were expressed as percentages and compared using chi-squared tests. A two-sided significance level of P < .05 was used for all analyses.
The primary exposure was the diagnosis of RA. The primary endpoint was the presence of CKD (binary variable). Secondary endpoints included CKD stage and albuminuria categories. We fitted multiple logistic regression models: an unadjusted model, a model adjusted for Systematic COronary Risk Evaluation 2 (SCORE2) cardiovascular risk, and a comprehensive multivariable model adjusted for age categories, sex, metabolic syndrome, smoking status, NSAID use and hsCRP.
For albuminuria analysis, we used ordinal logistic regression to examine the association between RA and albuminuria categories. Interaction terms were tested individually between RA and all covariates to explore potential effect modification. All analyses were performed using Stata 18/BE.
Ethics
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the federal state of Salzburg (415-E/1521/3–2012). All participants provided written informed consent.
RESULTS
Study population and baseline characteristics
A total of 9665 participants were included in the analysis, of whom 296 (3.1%) were diagnosed with RA. Participants with RA were significantly older than those without RA (median age 59 vs 55 years, P < .001) and more likely to be female (68% vs 51%, P < .001). RA patients had a higher prevalence of metabolic syndrome (35% vs 25%, P < .001) and were more likely to have abdominal obesity (58% vs 42%, P < .001), elevated blood pressure (66% vs 59%, P = .029) and elevated glucose levels (33% vs 27%, P = .023). Regular NSAID use was markedly higher in RA patients (21% vs 7%, P < .001). Cardiovascular risk profiles differed significantly, with RA patients showing higher SCORE2 risk scores (median 4.8 vs 4.0, P < .001) and elevated hsCRP levels (median 0.14 vs 0.12 mg/dL, P = .002; Table 1).
Kidney disease outcomes
CKD was present in 664 participants (6.9%) overall, with a significantly higher prevalence in RA patients compared with controls (11.8% vs 6.7%, P < .001) (Table 2). The distribution of CKD stages revealed distinct patterns between groups (P = .006). Presence of albuminuria in the context of preserved eGFR was predominant in RA patients and controls (6.8% vs 4.2%). Additionally, RA patients showed an increased prevalence of higher GFR categories (G3a–G5: 4.7% vs 2.3%). The ACR was higher in RA patients (median 4 vs 3 mg/g, P = .002), with 7.7% having ACR ≥30 mg/g compared with 4.8% in controls (P = .028, Fig. 1).
Distribution of ACR in participants with and without rheumatoid arthritis. RA patients exhibit a higher proportion of albuminuria even at preserved eGFR.
Association between rheumatoid arthritis and chronic kidney disease
In unadjusted analysis RA was significantly associated with CKD [odds ratio (OR) 1.86, 95% confidence interval (CI) 1.30–2.68, P = .001]. This association remained virtually unchanged after adjustment for cardiovascular risk using the SCORE2 calculator (OR 1.86, 95% CI 1.27–2.73, P = .001), suggesting that cardiovascular risk factors do not explain the observed relationship.
However, comprehensive multivariable adjustment substantially attenuated the association. After controlling for age categories, sex, metabolic syndrome, smoking status, NSAID use and hsCRP, the association between RA and CKD became non-significant (OR 1.43, 95% CI 0.96–2.13, P = .079), representing a 23% reduction in the odds ratio compared with the unadjusted analysis (Table 3).
Interaction analysis
To explore potential effect modification, we tested interactions between RA and all covariates in the multivariable model. A significant interaction was observed between RA and NSAID use (P = .042), suggesting that the association between RA and CKD varies by NSAID use status. Among participants not using NSAIDs, RA remained significantly associated with CKD (OR 2.02, 95% CI 1.34–3.05, P = .001), while the interaction term indicated a modified effect in RA patients using NSAIDs (interaction OR 0.40, 95% CI 0.17–0.97, P = .042).
No significant interactions were found between RA and age categories (50–59 years: interaction OR 2.11, 95% CI 0.26–17.19, P = .487; 60+ years: interaction OR 1.40, 95% CI 0.18–10.97, P = .751), sex (interaction OR 1.64, 95% CI 0.79–3.44, P = .186), metabolic syndrome (interaction OR 0.88, 95% CI 0.42–1.85, P = .740), smoking status (previous smoking: interaction OR 1.17, 95% CI 0.50–2.73, P = .715; current smoking: interaction OR 1.23, 95% CI 0.44–3.48, P = .693) or individual metabolic syndrome components (all P > .05). Similarly, no interaction was observed between RA and hsCRP levels (interaction OR 0.99, 95% CI 0.64–1.53, P = .955).
Albuminuria-specific analysis
Given the observed pattern of increased albuminuria in RA patients, we performed ordinal logistic regression to examine the association between RA and albumin–creatinine ratio categories. In unadjusted analysis, RA patients had significantly higher odds of more severe albuminuria categories (OR 1.66, 95% CI 1.07–2.56, P = .023). This association became slightly stronger after adjustment for cardiovascular risk using SCORE2 (OR 1.72, 95% CI 1.09–2.71, P = .019), suggesting that traditional cardiovascular risk factors may have been acting as negative confounders.
However, after comprehensive multivariable adjustment for age categories, sex, metabolic syndrome, smoking status, NSAID use and hsCRP, the association between RA and albuminuria severity was no longer statistically significant (OR 1.43, 95% CI 0.90–2.28, P = .132). This pattern paralleled the findings for binary CKD outcomes, suggesting that the relationship between RA and kidney disease outcomes is mediated through similar pathways regardless of the specific outcome measure.
DISCUSSION
In this large, population-based cohort, we found that RA was associated with a higher prevalence of CKD. Importantly, the predominant renal manifestation was albuminuria with preserved eGFR, rather than reduced eGFR. This phenotype suggests that early glomerular involvement is common in RA and highlights the need to assess both ACR and eGFR when evaluating kidney health in this population. Our findings extend previous research linking RA to an increased risk of CKD. Large cohort studies have consistently shown that RA patients are more likely to develop CKD compared with the general population [9]. Mendelian randomization analyses also support a causal effect of RA on kidney outcomes [11]. Earlier studies emphasized eGFR decline as the key feature of RA-related kidney disease [13]. By contrast, our data show that albuminuria is more frequent than reduced eGFR in RA patients, indicating early, subclinical renal injury. Mechanistically, this may reflect immune-mediated endothelial dysfunction, microvascular injury or subclinical glomerulonephritis [18, 19]. Importantly, because detailed rheumatology-specific data such as disease duration, serostatus and antirheumatic treatment exposure were not available, we cannot determine which RA-related factors (autoantibody-positive disease, chronic inflammatory activity or DMARD exposure) are driving the observed renal phenotype. Our findings therefore describe the renal phenotype of RA at a population level but do not allow causal or mechanistic inference.
The association between RA and CKD was attenuated after multivariable adjustment, suggesting that much of the excess risk is mediated by comorbidities such as obesity, hypertension and diabetes, which are highly prevalent in RA [20–22]. Nevertheless, the persistence of albuminuria in RA patients points to an additional disease-specific contribution beyond traditional risk factors. We also observed that the association between RA and CKD was confined to participants not reporting regular NSAID use. This counterintuitive finding is best explained by confounding by indication or reverse causation: patients at higher renal risk may avoid NSAIDs, while regular users may represent a healthier subset with preserved kidney function. Prior evidence shows that long-term NSAID use increases CKD risk, and prescribing patterns often reflect disease severity and baseline renal status [23, 24]. Thus, our results should not be interpreted as evidence of a protective effect of NSAIDs.
Strengths of this study include the large, unselected population sample, detailed metabolic and laboratory profiling, and the combined assessment of eGFR and albuminuria. This study has limitations. First, its cross-sectional design precludes causal inference regarding the direction of the association between RA and kidney injury. Second, although RA was defined according to established ACR/EULAR criteria, we lacked key rheumatology-specific variables, including disease duration, composite disease activity measures, serostatus and current or cumulative exposure to DMARDs. Third, albuminuria was assessed from a single spot urine sample, which may overestimate persistent proteinuria [13, 25].
In conclusion, albuminuria with preserved eGFR emerges as the predominant renal phenotype in RA, whereas reduced eGFR is less common. These findings emphasize the importance of routine albuminuria screening in RA patients, complementing eGFR measurement, to enable earlier detection and timely intervention. Multidisciplinary care models integrating nephrology into rheumatology practice may help improve long-term renal and cardiovascular outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aletaha D, Smolen JS. Achieving clinical remission for patients with rheumatoid arthritis. JAMA 2019;321:457–8. 10.1001/jama.2018.2124930721278 · doi ↗ · pubmed ↗
- 2Ausserwinkler M, Gensluckner S, Frey V et al. Cerebrovascular risk in rheumatoid arthritis patients: insights from carotid artery atherosclerosis in the Paracelsus 10,000 study. Rheumatol Int 2025;45:33. 10.1007/s 00296-024-05781-439825928 PMC 11742769 · doi ↗ · pubmed ↗
- 3Jankowski J, Floege J, Fliser D et al. Cardiovascular disease in chronic kidney disease: pathophysiological insights and therapeutic options. Circulation 2021;143:1157–72. 10.1161/CIRCULATIONAHA.120.05068633720773 PMC 7969169 · doi ↗ · pubmed ↗
- 4Kassebaum N J, Arora M, Barber R M et al. Global, regional, and national disability-adjusted life-years (DAL Ys) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1603–58. 10.1016/S 0140-6736(16)31460-X 27733283 PMC 5388857 · doi ↗ · pubmed ↗
- 5Shahbazi F, Doosti-Irani A, Soltanian A et al. Global forecasting of chronic kidney disease mortality rates and numbers with the generalized additive model. BMC Nephrol 2024;25:286. 10.1186/s 12882-024-03720-w 39223482 PMC 11370028 · doi ↗ · pubmed ↗
- 6Rahmadi A R, Pranata R, Raffaello W M et al. The effect of statin on major adverse cardiovascular events and mortality in patients with rheumatoid arthritis—a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci 2022;26:3171–8.35587067 10.26355/eurrev_202205_28734 · doi ↗ · pubmed ↗
- 7Smolen J S, Aletaha D, Mc Innes IB. Rheumatoid arthritis. Lancet 2016;388:2023–38. 10.1016/S 0140-6736(16)30173-827156434 · doi ↗ · pubmed ↗
- 8Levey A S, Eckardt K-U, Dorman N M et al. Nomenclature for kidney function and disease: report of a kidney disease: improving global Outcomes (KDIGO) Consensus Conference. Kidney Int 2020;97:1117–29. 10.1016/j.kint.2020.02.01032409237 · doi ↗ · pubmed ↗