Synchronous Acute Appendicitis and Acute Cholecystitis: A Report of a Rare Case
Samuel C Kim, Salvatore Grasso, Anthony McCloud, Gudata Hinika

TL;DR
A 29-year-old woman experienced both acute appendicitis and acute cholecystitis at the same time, requiring two surgeries.
Contribution
This paper reports a rare case of synchronous acute appendicitis and cholecystitis in a young patient.
Findings
The patient initially presented with acute appendicitis requiring drainage.
Seventeen days later, she developed acute cholecystitis requiring surgery.
Both conditions were confirmed via imaging and treated with laparoscopic procedures.
Abstract
Two of the most common emergent surgical interventions are acute appendicitis and acute cholecystitis. However, synchronous presentation is rare. In this report, we present a 29-year-old female patient with three days of worsening right lower quadrant (RLQ) pain with nausea and vomiting. Physical examination showed tenderness to palpation at the RLQ. Workup showed acute appendicitis with probable localized perforation and peri-appendiceal abscess, and CT-guided drainage was performed. The patient was discharged after four days. Seventeen days later, the patient returned to the ED with complaints of new right upper quadrant (RUQ) pain with nausea, vomiting, and loss of appetite. The ultrasound showed similar gallbladder findings with a positive sonographic Murphy’s sign. A CT scan showed appendicitis and cholecystitis with gallstones and mild gallbladder wall thickening. The patient then…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
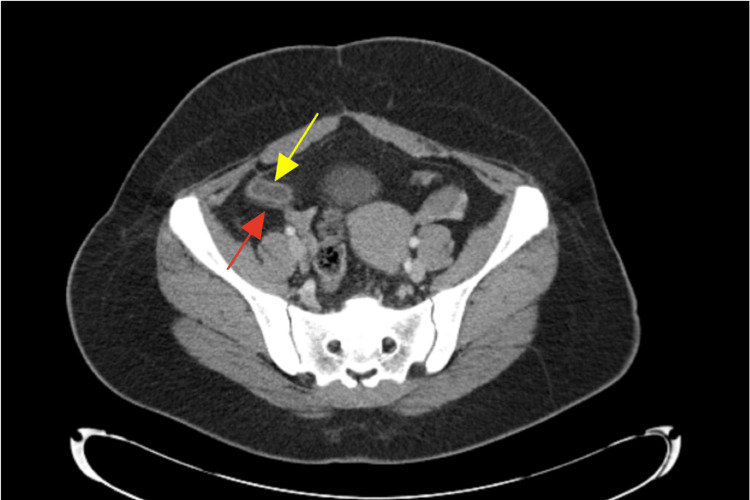 Figure 1
Figure 1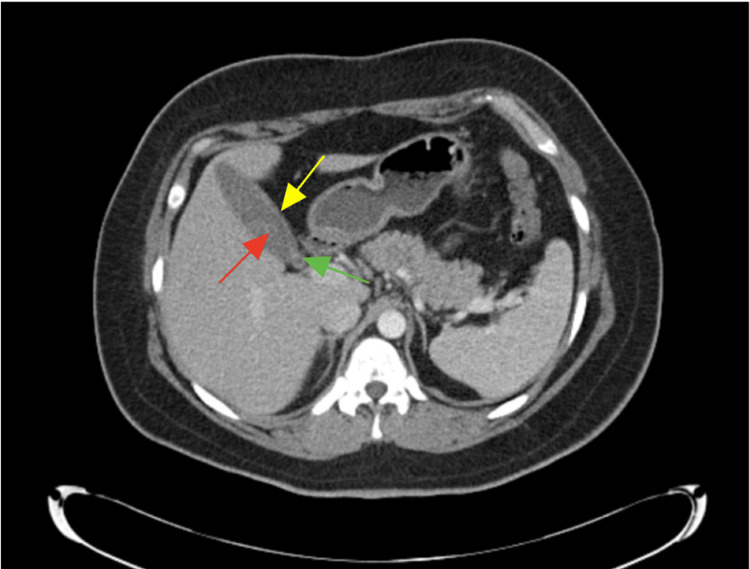 Figure 2
Figure 2| Parameters | Initial lab value | Lab values following presentation | Reference range |
| WBC | 18.9 | 8.2 | 4,500–11,000/mm3 |
| RBC | 4.64 | 4.81 | 4.40-6.00 M/uL |
| Hemoglobin | 13.1 | 13.6 | 12.0-16.0 g/dL |
| Hematocrit | 38.4 | 39.4 | 36%-46% |
| Mean corpuscular volume | 82.6 | 81.9 | 80-100 fL |
| Mean corpuscular hemoglobin | 28.3 | 28.2 | 25.0-35.0 pg |
| Mean corpuscular hemoglobin concentration | 34.2 | 34.4 | 31%-36% Hb/cell |
| Red cell distribution width | 13.1 | 13.2 | <16.4 % |
| Platelet | 385 | 381 | 150,000-400,000/mm3 |
| Mean platelet volume | 6.8 | 7.2 | 7-9 fL |
| Absolute neutrophil count | 16.4 | 5.1 | 2.0-8.0 K/uL |
| ABS lymphocyte count | 1.3 | 2.5 | 1.0-5.1 K/uL |
| ABS monocyte count | 1.1 | 0.4 | 0.0-0.8 K/uL |
| ABS eosinophil count | 0.0 | 0.2 | 0.0-0.5 K/uL |
| ABS basophil count | 0.0 | 0.0 | 0.0-0.2 K/uL |
| Neutrophil % | 87.0 | 62.2 | 49.0-74.0 % |
| Lymphocyte % | 6.9 | 30.3 | 26.0-46.0 % |
| Monocyte % | 5.8 | 4.9 | 2.0-12.0 % |
| Eosinophil % | 0.1 | 2.0 | 0.0-5.0 % |
| Basophil % | 0.2 | 0.6 | 0.0-2.0 % |
| Sodium | 136 | 137 | 136-146 mEq/L |
| Potassium | 4.1 | 5.1 | 3.5-5.0 mEq/L |
| Chloride | 100 | 106 | 95-105 mEq/L |
| CO2 | 24 | 20 | 22-28 mEq/L |
| Anion gap | 12 | 11 | 8-16 mEq/L |
| Glucose | 114 | 120 | <140 mg/dL |
| Blood urea nitrogen (BUN) | 8.00 | 11.0 | 7-18 mg/dL |
| Creatinine | 0.8 | 0.8 | 0.6-1.2 mg/dL |
| BUN/creatinine ratio | 10.1 | 14.5 | 10-20:1 |
| Estimated glomerular filtration rate (eGFRcr) | 104 | 109 | 90-120 mL/min/1.73m |
| Calcium | 9.4 | 9.1 | 8.4-10.2 mg/DL |
| Protein, total | 8.60 | 8.40 | 6.0-7.8 g/dL |
| Albumin (A) | 4.0 | 3.9 | 3.5-5.5 g/dL |
| Globulin (G) | 4.6 | 3.9 | 2.3-3.5 g/dL |
| A/G ratio | 0.9 | 4.5 | 1.1-2.5 |
| Bilirubin total | 0.5 | 0.2 | 0.1-1.0 mg/dL |
| Alanine transaminase (ALT) | 30 | 28 | 10-40 U/L |
| Aspartate aminotransferase (AST) | 23 | 33 | 12-39 U/L |
| Alkphos | 92.0 | 71.0 | 25-100 U/L |
| Lipase | 9 | 25 | 13-60 U/L |
| Urianalysis: Color | Yellow | Straw | - |
| Appearance | Hazy | Clear | - |
| Specific gravity | 1.026 | 1.025 | 1.005-1.030 |
| Urinary pH | 7.5 | 5.5 | 4.5-8 |
| Urinary glucose | Negative | Negative | Negative |
| Urinary bilirubin | Negative | Negative | Negative |
| Urinary ketones | 10 mg/dL | Negative | Negative |
| Urinary blood | Moderate | Small | Negative |
| Urinary protein | 50 mg/dL | Negative | Negative |
| Urianalysis urobilinogen | Negative | Negative | Negative |
| Urinary nitrite | Negative | Negative | Negative |
| Urinary leukocyte esterase | Small | Moderate | Negative |
| Urinary analysis squamous epithelial | 17/HPF | 21/HPF | Negative |
| Urine WBCs | 6-10 | 3-5 | Negative |
| Urinary RBC | 16-25 | 6-10 | Negative |
| Urinary mucous | Rare | Rare | Negative |
| Urinary bacteria | Rare | Rare | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAppendicitis Diagnosis and Management · Gallbladder and Bile Duct Disorders · Intestinal Malrotation and Obstruction Disorders
Introduction
Acute appendicitis and acute cholecystitis are very common in the United States. There are approximately 350,000 cases of appendicitis and 200,000 cases of cholecystitis annually [1,2]. Acute appendicitis often presents as pain in the periumbilical region that migrates to the right lower quadrant (RLQ) to McBurney’s Point, while acute cholecystitis often presents as pain in the right upper quadrant (RUQ) or epigastrium with possible radiation to the right shoulder or back and a positive Murphy’s sign. Both conditions often present with fever, nausea, vomiting, and/or anorexia.
Acute appendicitis is usually diagnosed by a CT scan, a medical imaging technique used to obtain detailed internal images of the body, and a physical examination. Sensitivity is reported at 0.95 (95% CI [0.93, 0.96]) and specificity at 0.94 (95% CI (0.92, 0.95)) using a CT scan to diagnose acute appendicitis [3]. Acute cholecystitis is usually diagnosed with an ultrasound, an imaging test that uses sound waves to make pictures of organs, tissues, and other structures inside the body, but a CT scan can also be effective. The ultrasound has the best unadjusted sensitivity (0.97; 95% CI (0.95, 0.99)) and specificity (0.95; 95% CI (0.88, 1.00)) for evaluating patients with acute cholecystitis [4].
Each individual condition and presentation in patients can be treated medically with antibiotics and symptom management or surgically with laparoscopic resection or open resection [5,6]. Laparoscopic surgery is the gold standard for both conditions, respectively [1,7]. There have been rare cases of synchronous appendicitis and cholecystitis. One literature review found only 11 case reports of coexistent acute appendicitis and acute cholecystitis [8]. Furthermore, one coexistent case of ruptured appendix and acute cholecystitis has been reported [9], while another case with ruptured gallbladder and acute appendicitis has been reported [10]. In this report, we present a unique, and to the best of our knowledge, first-of-its-kind case of acute appendicitis with appendiceal abscess with synchronous acute cholecystitis.
This article was previously presented as a poster presentation at the 2024 California Hospital Medical Center (CHMC)/Ross University Medical School Annual Conference on May 31st, 2024.
Case presentation
A 29-year-old Hispanic female patient presented to the emergency department with three days of worsening RLQ pain with associated nausea, vomiting, dysuria, and diarrhea. On the third day of pain, she went to see her primary medical doctor, who sent her to the emergency department (ED) to rule out acute appendicitis. She reported experiencing a similar episode one week earlier that had resolved spontaneously. Her only past medical history consisted of a prior cesarean section; she denied other medical, family, or social risk factors.
In the ED, the patient was afebrile (36.4°C) with a heart rate of 85 bpm, respiratory rate of 20, blood pressure of 132/86 mmHg, and oxygen saturation of 97% on room air. Her abdomen was mildly distended and exhibited marked RLQ tenderness to even light palpation, accompanied by guarding. There was no rigidity, no rebound tenderness, and both the obturator and Rovsing’s signs were negative. Laboratory studies (Table 1) revealed leukocytosis to 18.9 thousand with a left shift (87% neutrophils) and otherwise unremarkable electrolytes and liver function tests.
The patient's urinalysis demonstrated pyuria suggestive of a mild urinary tract infection. Given the physical exam findings, the ED physicians opted to bypass ultrasound and proceed with CT imaging for further evaluation. A CT abdomen and pelvis with IV contrast showed findings consistent with acute appendicitis with probable localized perforation and peri-appendiceal abscess. The patient received Toradol, Zosyn, and 1 L of normal saline (NS) bolus x two before admission to the floor.
The following day, the patient underwent CT-guided IR drainage of the abscess. A right lower quadrant drain was placed, and purulent material was noted upon insertion. She continued to improve clinically and was discharged on postoperative day four with strict return precautions and instructions for outpatient drain monitoring and eventual removal.
On postoperative day eight, the patient returned to the ED requesting removal of the drain. She reported only mild discomfort and approximately 15 cc of output in the accordion reservoir. Repeat CT imaging demonstrated no residual abscess but persistent inflammation surrounding the appendix (Figure 1). Given these findings, the decision was made to leave the drain in place for an additional week, and she was discharged home.
Transverse CT of abdomen on postoperative day eightYellow arrow: Appendiceal wall thickening without an overt source of obstruction; Red arrow: Fat stranding surrounding the appendix signifying an inflammatory reaction
Five days later, the patient again presented to the ED with mild abdominal pain and continued minimal drainage from the catheter. Because she had a history of a perforated appendicitis with ongoing drainage, repeat imaging was clinically justified. The CT imaging revealed a fluid-filled, distended appendix unchanged from prior studies and no remaining fluid collections. New findings included gallbladder sludge and stones. As the abscess had resolved and the drain was no longer necessary, it was removed, and the patient was discharged in stable condition.
Approximately 20 days after her initial appendicitis and abscess drainage, the patient returned to the ED with a two-day history of worsening RUQ pain accompanied by mild residual RLQ discomfort. She reported that the pain typically began about 10 minutes after eating and radiated to her mid-back, noting that she had experienced similar episodes in the past. She also endorsed associated nausea and decreased appetite, but denied any vomiting.
On examination, the patient was afebrile at 36.6°C with a heart rate of 63 bpm, respiratory rate of 18, blood pressure of 109/74 mmHg, and oxygen saturation of 97% on room air. She exhibited focal tenderness to palpation in the RUQ. Laboratory evaluation revealed a WBC count of 8.2 × 10³/µL with 62.2% neutrophils and otherwise normal complete blood count (CBC) and comprehensive metabolic panel (CMP) values (see Table 1). Urinalysis was notable for asymptomatic bacteriuria. The CT abdomen and pelvis (Figure 2) with IV contrast showed a fluid-filled appendix with mucosal thickening and surrounding inflammation changes consistent with acute appendicitis, though less dilated than prior CT, with gallstones and gallbladder wall thickening. The RUQ ultrasound showed gallstones with wall thickening and a positive sonographic Murphy’s sign. General surgery was consulted, and a combined laparoscopic cholecystectomy and appendectomy was planned.
Transverse CT of abdomen on postoperative day 20Yellow arrow: Mild gallbladder wall thickening; Red arrow: Presence of gallstones; Green arrow: Gallstone evident at the neck of the gallbladder as a possible source of obstruction to outflow of bile secretion
Preoperatively, the patient was resuscitated with IV fluids. She received IV pain control and was started on empiric IV antibiotics with Zosyn (piperacillin-tazobactam). The following day, she was taken to the operating room for a laparoscopic cholecystectomy and appendectomy, which she tolerated well without complications. Postoperatively, she resumed a regular diet and had a return of bowel function, allowing for discharge on postoperative day four with a prescribed course of antibiotics. Her recovery was uneventful.
Discussion
Classical presentations of both pathologies are extensively described in medical literature, but their synchronous presentation varies for every patient, which may lead to challenges in diagnosis and management. In our unique patient, her initial appendiceal abscess with appendicitis was treated medically, as that was deemed safer for the patient [11]. After her synchronous development of acute cholecystitis with appendicitis, medical management was no longer safe for the patient, and urgent surgical intervention was planned.
Carter et al. [12] described biliary reflux or gallbladder dyskinesia associated with acute appendicitis that was relieved after an appendectomy. Another report suggested that the direct bacterial invasion or translocation from the muscularis propria of a gangrenous appendix into the portal venous system caused impairment of bile salt excretion, leading to acute cholecystitis, which was managed surgically [8]. The Kancheva et al. [13] case report of synchronous acute appendicitis and acute cholecystitis summarized some synchronous cases and showed that all but one case were treated surgically. The gold standard of permanent treatment for acute cholecystitis remains surgical resection [14]. Though the Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis (APPAC) [15] trials established that antibiotic medical treatment of uncomplicated appendicitis is appropriate, our patient’s case of appendicitis was complicated. Buhamed et al. [8] report that surgical management in synchronous cases is appropriate to avoid complications of perforation or septicemia.
With few reported cases of simultaneous pathologies, with possibly no prior reported cases of an appendiceal abscess with appendicitis and synchronous acute cholecystitis, it is difficult to explain the etiology. Drawing from the literature review, which reports a 73.6% rate [16] favoring operative intervention, we find that surgical management offers superior outcomes for patients with synchronous appendicitis and cholecystitis compared with medical management. Therefore, a five-port laparoscopic approach is recommended as an appropriate and effective operative strategy.
Conclusions
Concurrent acute appendicitis and acute cholecystitis remain a medical mystery and a surgical urgency. Thorough history, physical examination, and imaging workup are essential for diagnosis. Surgical interventions, especially laparoscopic procedures, remain the gold standard. This case underscores the importance of recognizing and managing this rare condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The global incidence of appendicitis: a systematic review of population-based studies Ann Surg Ferris M Quan S Kaplan BS 23724126620172828806010.1097/SLA.0000000000002188 · doi ↗ · pubmed ↗
- 2Nationwide trends of hospital admissions for acute cholecystitis in the United States Gastroenterol Rep (Oxf) Wadhwa V Jobanputra Y Garg SK Patwardhan S Mehta D Sanaka MR 3642520172717443410.1093/gastro/gow 015PMC 5444253 · doi ↗ · pubmed ↗
- 3Computed tomography for diagnosis of acute appendicitis in adults Cochrane Database Syst Rev Rud B Vejborg TS Rappeport ED Reitsma JB Wille-Jørgensen P 2019201910.1002/14651858.CD 009977.pub 2PMC 695339731743429 · doi ↗ · pubmed ↗
- 4Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease Arch Intern Med Shea JA Berlin JA Escarce JJ 2573258115419947979854 · pubmed ↗
- 5Delays by patients, emergency physicians, and surgeons in the management of acute appendicitis: retrospective study Hong Kong Med J Chung CH Ng CP Lai KK 25425962000 https://pubmed.ncbi.nlm.nih.gov/11025842/11025842 · pubmed ↗
- 6Clinical presentation, imaging, and management of acute cholecystitis Tech Vasc Interv Radiol Katabathina VS Zafar AM Suri R 2562651820152661516610.1053/j.tvir.2015.07.009 · doi ↗ · pubmed ↗
- 7Acute cholecystitis: a review JAMA Gallaher JR Charles A 96597532720223525852710.1001/jama.2022.2350 · doi ↗ · pubmed ↗
- 8Synchronous acute appendicitis and acute cholecystitis, is it a myth or reality? A literature review Open Access Emerg Med Buhamed F Edward M Shuaib A 2012031120193149684210.2147/OAEM.S 214161 PMC 6701664 · doi ↗ · pubmed ↗