Effects of Treatment and Weather Variables on Nocturnal Enuresis: Long-Term Analysis Using the Classification and Regression Trees Model
Yuta Onuki, Teruo Miyano, Yuma Iwanaka, Takahiro Ono, Shota Endo, Chisato Oyake, Yoshitaka Watanabe, Masaki Fuyama, Tsuneki Watanabe, Tomoko O Morita, Takahiro Arai, Hirokazu Ikeda

TL;DR
This study found that weather and treatment factors influence bedwetting in children, suggesting personalized plans could improve long-term outcomes.
Contribution
The study introduces a novel approach by combining clinical and weather variables to analyze long-term nocturnal enuresis risk using CART models.
Findings
Meteorological variables like temperature and calendar month significantly influence NE risk.
Vibegron appears more effective than other treatments in reducing NE risk.
Individualized treatment plans considering seasonal and environmental factors may improve outcomes.
Abstract
Objective: Nocturnal enuresis (NE), also known as bedwetting, is a common urological condition in children that often requires extended treatment. Although numerous studies have examined NE risk factors, the long-term effects of combined clinical and external factors, such as weather variables, remain unexplored. This study aimed to explore composite risk factors for NE and evaluate their long-term effects. Methods: This was a prospective observational study with unbalanced panel data analyzed using the classification and regression trees (CART) model. The study was conducted in Japan, with clinical and meteorological data collected over 14 months. Nineteen pediatric patients aged 6-15 years diagnosed with NE based on International Pediatric Continence Society guidelines were included. In total, 3194 daily records from 19 participants (after excluding 1 due to excessive missing values)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1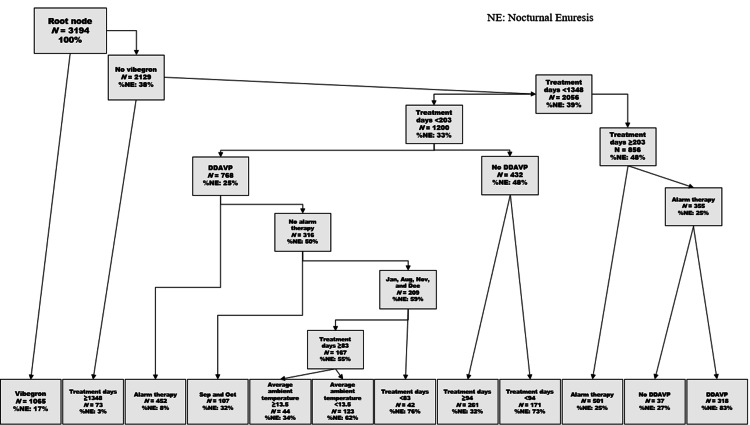 Figure 2
Figure 2| Sr. No. | Inclusion and Exclusion Criteria |
| Inclusion criteria | |
| 1 | Intermittent urinary incontinence during sleep in children aged >5 years |
| 2 | Bedwetting at least once a month for ≥3 months |
| 3 | Primary monosymptomatic nocturnal enuresis |
| 4 | No missing data |
| Exclusion criteria | |
| 1 | Urinary tract infection within the preceding 3 months |
| 2 | Diabetes mellitus |
| 3 | History of renal disease, hypertension or genitourinary abnormalities, neurological disease, or psychological disease |
| Characteristics | Overall (n = 19) | |
| Age | ||
| Mean ± SD | 9.58 ± 2.48 | |
| Median | 9 | |
| Range | (6-15) | |
| Sex | ||
| Male | 12 | |
| Female | 7 | |
| Height | ||
| Mean ± SD | 128.2 ± 11.1 | |
| Median | 127.2 | |
| Range | 111.0 - 147.7 | |
| Weight | ||
| Mean ± SD | 27.2 ± 6.7 | |
| Median | 27.6 | |
| Range | 17.5 - 40.0 | |
| Treatment | ||
| Vasopressin (DDAVP) | 11 | |
| Solifenacin succinate | 9 | |
| Vibegron | 6 | |
| Alarm therapy | 10 | |
| Osmotic laxatives | 4 | |
| No. | Presence or Absence of Bedwetting | Number of Days of Observation | Presence or Absence of Treatment | DDAVP Used | Alarm Used | Solifenacin Used | Vibegron Used | Osmotic Laxative Used |
| 1 | 24 | 223 | 183 | 0 | 0 | 223 | 182 | 0 |
| 2 | 55 | 141 | 141 | 0 | 0 | 141 | 141 | 0 |
| 3 | 49 | 315 | 315 | 0 | 0 | 292 | 256 | 311 |
| 4 | 263 | 317 | 317 | 317 | 0 | 218 | 0 | 98 |
| 5 | 43 | 260 | 260 | 180 | 260 | 180 | 0 | 0 |
| 6 | 24 | 78 | 78 | 0 | 78 | 0 | 0 | 78 |
| 7 | 28 | 245 | 245 | 0 | 237 | 0 | 245 | 0 |
| 8 | 24 | 161 | 161 | 0 | 0 | 0 | 161 | 0 |
| 9 | 78 | 80 | 80 | 80 | 80 | 0 | 80 | 0 |
| 10 | 81 | 273 | 273 | 273 | 273 | 273 | 0 | 0 |
| 11 | 28 | 98 | 90 | 0 | 90 | 0 | 0 | 0 |
| 12 | 61 | 154 | 154 | 154 | 154 | 154 | 0 | 0 |
| 13 | 9 | 134 | 134 | 109 | 64 | 64 | 0 | 0 |
| 14 | 23 | 133 | 77 | 77 | 0 | 0 | 0 | 0 |
| 15 | 143 | 154 | 98 | 98 | 98 | 98 | 0 | 0 |
| 16 | 6 | 203 | 203 | 203 | 0 | 203 | 0 | 0 |
| 17 | 12 | 64 | 64 | 64 | 0 | 28 | 0 | 64 |
| 18 | 18 | 75 | 64 | 64 | 0 | 0 | 0 | 0 |
| 19 | 64 | 86 | 56 | 0 | 56 | 0 | 0 | 0 |
| Total | 1033 | 3194 | 2993 | 1619 | 1390 | 1874 | 1065 | 551 |
| Year | January | February | March | April | May | June | July | August | September | October | November | December |
| 2000 | 7.6 | 6 | 9.4 | 14.5 | 19.8 | 22.5 | 27.7 | 28.3 | 25.6 | 18.8 | 13.3 | 8.8 |
| 2001 | 4.9 | 6.6 | 9.8 | 15.7 | 19.5 | 23.1 | 28.5 | 26.4 | 23.2 | 18.7 | 13.1 | 8.4 |
| 2002 | 7.4 | 7.9 | 12.2 | 16.1 | 18.4 | 21.6 | 28 | 28 | 23.1 | 19 | 11.6 | 7.2 |
| 2003 | 5.5 | 6.4 | 8.7 | 15.1 | 18.8 | 23.2 | 22.8 | 26 | 24.2 | 17.8 | 14.4 | 9.2 |
| 2004 | 6.3 | 8.5 | 9.8 | 16.4 | 19.6 | 23.7 | 28.5 | 27.2 | 25.1 | 17.5 | 15.6 | 9.9 |
| 2005 | 6.1 | 6.2 | 9 | 15.1 | 17.7 | 23.2 | 25.6 | 28.1 | 24.7 | 19.2 | 13.3 | 6.4 |
| 2006 | 5.1 | 6.7 | 9.8 | 13.6 | 19 | 22.5 | 25.6 | 27.5 | 23.5 | 19.5 | 14.4 | 9.5 |
| 2007 | 7.6 | 8.6 | 10.8 | 13.7 | 19.8 | 23.2 | 24.4 | 29 | 25.2 | 19 | 13.3 | 9 |
| 2008 | 5.9 | 5.5 | 10.7 | 14.7 | 18.5 | 21.3 | 27 | 26.8 | 24.4 | 19.4 | 13.1 | 9.8 |
| 2009 | 6.8 | 7.8 | 10 | 15.7 | 20.1 | 22.5 | 26.3 | 26.6 | 23 | 19 | 13.5 | 9 |
| 2010 | 7 | 6.5 | 9.1 | 12.4 | 19 | 23.6 | 28 | 29.6 | 25.1 | 18.9 | 13.5 | 9.9 |
| 2011 | 5.1 | 7 | 8.1 | 14.5 | 18.5 | 22.8 | 27.3 | 27.5 | 25.1 | 19.5 | 14.9 | 7.5 |
| 2012 | 4.8 | 5.4 | 8.8 | 14.5 | 19.6 | 21.4 | 26.4 | 29.1 | 26.2 | 19.4 | 12.7 | 7.3 |
| 2013 | 5.5 | 6.2 | 12.1 | 15.2 | 19.8 | 22.9 | 27.3 | 29.2 | 25.2 | 19.8 | 13.5 | 8.3 |
| 2014 | 6.3 | 5.9 | 10.4 | 15 | 20.3 | 23.4 | 26.8 | 27.7 | 23.2 | 19.1 | 14.2 | 6.7 |
| 2015 | 5.8 | 5.7 | 10.3 | 14.5 | 21.1 | 22.1 | 26.2 | 26.7 | 22.6 | 18.4 | 13.9 | 9.3 |
| 2016 | 6.1 | 7.2 | 10.1 | 15.4 | 20.2 | 22.4 | 25.4 | 27.1 | 24.4 | 18.7 | 11.4 | 8.9 |
| 2017 | 5.8 | 6.9 | 8.5 | 14.7 | 20 | 22 | 27.3 | 26.4 | 22.8 | 16.8 | 11.9 | 6.6 |
| 2018 | 4.7 | 5.4 | 11.5 | 17 | 19.8 | 22.4 | 28.3 | 28.1 | 22.9 | 19.1 | 14 | 8.3 |
| 2019 | 5.6 | 7.2 | 10.6 | 13.6 | 20 | 21.8 | 24.1 | 28.4 | 25.1 | 19.4 | 13.1 | 8.5 |
| 2020 | 7.1 | 8.3 | 10.7 | 12.8 | 19.5 | 23.2 | 24.3 | 29.1 | 24.2 | 17.5 | 14 | 7.7 |
| 2021 | 5.4 | 8.5 | 12.8 | 15.1 | 19.6 | 22.7 | 25.9 | 27.4 | 22.3 | 18.2 | 13.7 | 7.9 |
| 2022 | 4.9 | 5.2 | 10.9 | 15.3 | 18.8 | 23 | 27.4 | 27.5 | 24.4 | 17.2 | 14.5 | 7.5 |
| 2023 | 5.7 | 7.3 | 12.9 | 16.3 | 19 | 23.2 | 28.7 | 29.2 | 26.7 | 18.9 | 14.4 | 9.4 |
| Average ambient temperature (℃) | 6.0 | 6.8 | 10.3 | 14.9 | 19.4 | 22.7 | 26.6 | 27.8 | 24.3 | 18.7 | 13.6 | 8.4 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Bladder and Prostate Research · Urinary Tract Infections Management · Pelvic floor disorders treatments
Introduction
Nocturnal enuresis (NE) is a disorder characterized by urination during nighttime sleep at least once a month after the age of five. NE is a common pediatric condition, affecting 15% of 6-year-olds and 6.4% of all children [1]. Although NE is not associated with physical symptoms, such as pain or fatigue, it markedly impacts a child’s mental well-being, contributing to low self-esteem, poor self-image, and a decline in school life quality and friendships [2, 3]. NE also reduces the overall quality of life for both affected children and their parents [4]. As a complex disorder, NE involves multiple factors, including increased urine production, urinary muscle overactivity, and sleep disturbances, with disorders of the autonomic nervous system believed to contribute to its onset [5-11]. Although several studies have explored the correlation between autonomic neuropathy and weather, the relationship between NE and weather remains unclear [12].
Standard treatments for NE include behavioral, medication, and alarm therapies [13, 14], with therapy choice tailored to the individual needs of the child and their family. However, treatment effectiveness varies markedly, and many cases remain unresponsive. Additionally, there is considerable variation in treatment duration, ranging from several weeks to years. Furthermore, NE recurrence is common, and many cases require ongoing follow-up and support. Despite the need for long-term treatment, few studies have investigated the actual long-term treatment practices. Therefore, this study aimed to identify combined risk factors for NE, including the influence of weather variables, and assess their long-term impact on the condition.
Materials and methods
This study was approved by the Ethics Committee of Showa Medical University Hospital (approval number: 22-161-B), and written informed consent was obtained from all participants and their parents. This study established participant inclusion and exclusion criteria (Table 1).
The study included pediatric patients aged 6-15 years diagnosed with NE based on International Paediatric Continence Society guidelines [13, 14]. The study period spanned from December 15, 2022, to February 1, 2024. Daily records of bedwetting occurrence were collected, resulting in 3,222 daily records. One participant with incomplete data on the outcome variable and/or dependent variable was excluded. Because the study also aimed to observe treatment interactions, we concluded that this case did not meet the criteria for inclusion as an observational participant. Consequently, 3,194 daily records from 19 individuals were included in the analysis (Figure 1).
Flow diagramsFlowchart for this study
This study utilized daily records for analysis to evaluate the impact of weather variables. Treatment duration varied widely, ranging from 1 day to 1,469 days, which allowed for the assessment of long-term treatment effects. The dataset included seven baseline variables, namely sex, age, residential region, height, weight, record date, and NE status (presence of incontinence). Five treatment dummy variables were included, namely desmopressin, solifenacin succinate, alarm therapy, and osmotic laxatives, which are recognized in the nocturnal enuresis guidelines, along with vibegron, which is not currently listed. Additionally, six major weather variables were extracted from Japan Meteorological Agency data [15] and included in the analysis: daily average ambient temperature, daily ambient temperature difference, total precipitation, sunshine hours, average atmospheric pressure, and average humidity. Meteorological data were matched with clinical records to create pooled data.
Given that the effects of weather variables and treatment duration on NE risk are nonlinear, and specific changes within a range can markedly affect NE outcomes, the classification and regression trees (CART) model was employed to account for the nonlinearity and complex patterns within the data. The CART model was adopted as the analytical method because it effectively ranks the importance of variables and identifies thresholds among multivariate causal analysis methods. Statistical analyses were performed using R version 4.3.3 (R Core Team). For the CART model analysis, the “rpart” function from the “rpart” package was used. Initially, the complexity parameter (cp) was set at 0.0001 to generate the largest possible tree. Cross-validation error (xerror) was then examined for tree pruning, and the final model was established using the cp value corresponding to the minimum xerror. Consequently, the final parameters were set to minbucket = 32 and cp = 0.0064.
Results
Nineteen patients with NE were enrolled, and patient characteristics are provided in Tables 2-3.
CART analysis, incorporating meteorological variables, selected several combined factors contributing to bedwetting in more than 60% of patients: a history of desmopressin use, no history of vibegron use, treatment duration of less than 203 days, a history of alarm therapy, calendar months (January, August, November, and December), treatment duration of ≥83 days, and average daily ambient temperature below 13.5°C (Figure 2).
CART analysisDecision tree derived from this study.DDAVP: desamino-d-arginine vasopressin; CART: classification and regression trees
With respect to vibegron, the risk of NE was 17% in the group with a history of vibegron treatment, whereas it was higher at 38% in the group without vibegron treatment. For desmopressin and alarm therapy, the risk of NE was significantly greater in the groups without a treatment history compared to those with a treatment history: 48% versus 25% for desmopressin, and 50% versus 8% for alarm therapy, respectively. Analysis by treatment duration showed that NE risk increased significantly to 48% with treatment duration of 203 days or more compared with 33% for less than 203 days, and 76% for less than 82.5 days compared with 55% for 82.5 days or more. Additionally, the risk of NE improved to 3% when treatment duration reached 1,348 days or more. For meteorological variables, the risk of NE was significantly higher at 62% when the mean ambient temperature was below 13.5°C compared to 34% at 13.5°C or higher. Notably, meteorological variables were selected as combined risk factors alongside pharmacological and behavioral therapies. Furthermore, vibegron, a β3-adrenergic receptor agonist, was also represented as a combined factor that reduces the risk of NE. Regarding treatment duration, variations in NE risk were suggested around 1,348, 203, and 83 days.
Discussion
This study is the first to suggest that a meteorological factor, namely the daily average ambient temperature, influences the onset of NE. The key findings are as follows: (1) even when using desmopressin or alarm therapy, which are first-line treatments for NE, the risk of urinary incontinence increases as the daily average ambient temperature decreases; (2) although not explicitly recommended in current NE treatment guidelines, vibegron, a β3-adrenergic receptor agonist, was suggested to potentially contribute to reducing NE risk.
Previous studies by Tas et al. and Murillo et al. have shown that the incidence of NE episodes is significantly higher in winter than in summer, with increased failure rates of desmopressin treatment during winter. Our findings support this, suggesting that seasonal factors-specifically January, August, November, and December-increase the risk of NE-related urinary incontinence. Notably, January, November, and December correspond to winter months in Japan, characterized by particularly low ambient temperatures, consistent with prior reports (Table 4).
In contrast, August represents the summer season with the highest ambient temperatures; however, increased fluid intake during this month may disrupt fluid balance and elevate nocturnal urination risk, which likely explains its selection as a risk factor.
Regarding treatment duration, improvements were observed before 83 days and after 1,348 days from treatment initiation, whereas NE risk increased with treatment durations shorter than 203 days. Improvement before 83 days likely reflects the initial therapeutic response. The risk reduction after 1,348 days likely corresponds to the maturation of bladder function with age. Conversely, worsening risk after 203 days may be related to decreased motivation over prolonged treatment periods and seasonal temperature fluctuations. Although the treatment duration thresholds identified in this study serve as reference values, our long-term follow-up revealed that NE symptoms follow a nonlinear course characterized by cycles of exacerbation and remission, ultimately resulting in improvement.
NE guidelines recommend desmopressin and alarm therapy as first-line treatments and suggest anticholinergic agents and tricyclic antidepressants if these are ineffective [13, 14]. The CART analysis in this study confirmed that the therapies recommended in the guidelines reduce NE risk. Notably, vibegron was also suggested to potentially be effective for NE. Vibegron works by stimulating β3 receptors in the bladder smooth muscle [16], leading to muscle relaxation and improved urinary retention. Conversely, anticholinergic drugs inhibit excessive bladder contractions, in contrast to β3 receptor agonists, which relax the bladder, enhancing its ability to hold urine [17]. Previous clinical trials in adult women with an overactive bladder have shown the efficacy of β3 agonists compared to muscarinic receptor antagonists. For example, Vecchioli et al. reported that mirabegron (a β3 receptor agonist) significantly reduced post-void residual urine volume compared with solifenacin (a muscarinic antagonist) in such adults [17]. In contrast, the results of this study merely suggest the potential effectiveness of β3 receptor agonists for NE, and comparative trials to confirm their efficacy for this condition are awaited.
This study has several limitations. First, the small sample size and focus on a specific geographic region may limit the generalizability of the findings. Additionally, the complex interactions among weather variables such as barometric pressure, humidity, and sunlight hours require further investigation to fully understand their effects. A multifaceted approach to NE research is essential, taking into account not only physiological and psychological factors but also the influence of patients’ lifestyles. Furthermore, as this study is exploratory, confirmatory trials with larger sample sizes are needed to validate the efficacy of vibegron and the threshold values for outdoor temperature selected as composite factors.
Our study is the first to report the influence of an external environmental factor, namely the daily average ambient temperature, on NE symptoms, particularly bedwetting. Additionally, the risk of NE was shown to vary nonlinearly with changes in weather, treatment efficacy, and patient motivation. These findings underscore the importance of clinical management strategies that consider seasonality and environmental factors, suggesting practical recommendations such as advising families to maintain warm indoor temperatures during colder seasons, which may effectively reduce bedwetting incidence.
Study strengths and limitations
Strengths
To our knowledge, this is the first study to evaluate the impact of daily average ambient temperature on NE development using long-term treatment data. The CART model highlighted daily average ambient temperature, alongside clinical factors, as a key combined factor associated with NE risk.
Limitations
The study’s small sample size may limit the generalizability of the findings. In the analysis, daily records were used to examine the association between daily meteorological factors and NE; however, these records were based on individual cases and cannot be considered fully independent. Although vibegron, a β3 receptor agonist not currently listed in NE treatment guidelines, was suggested to reduce NE risk, further validation is required. Currently, trials comparing vibegron and muscarinic (M3) receptor antagonists are lacking. This study is exploratory, investigating whether meteorological variables are associated with NE risk. Therefore, further validation of the CART-derived cutoff values is required.
Conclusions
This study proposes potential combined factors, including meteorological variables such as daily average ambient temperature, that influence the risk of urinary incontinence. The findings suggest that seasonal variations in temperature should be considered in the risk assessment of NE. Additionally, the potential efficacy of β3-adrenergic receptor agonists for NE was indicated, warranting future comparative trials. These results contribute to improved risk prediction and the development of more effective treatment strategies for NE.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Improvements in self-concept after treatment of nocturnal enuresis: Randomized controlled trial J Pediatr Moffatt ME Kato C Pless IB 6476521101987355002610.1016/s 0022-3476(87)80572-3 · doi ↗ · pubmed ↗
- 2Self-image and performance in children with nocturnal enuresis Eur Urol Theunis M Van Hoecke E Paesbrugge S Hoebeke P Walle JV 6606674120021207478510.1016/s 0302-2838(02)00127-6 · doi ↗ · pubmed ↗
- 3Assessment of psychosocial function in children with non-monosymptomatic nocturnal enuresis Jpn Soc Pediatr Nephrol Ikeda H Oyake C Onuki Y Hirabayashi C Nunoyama M Watanabe T 1420302017
- 4An evaluation of quality of life of mothers of children with enuresis nocturna Pediatr Nephrol Egemen A Akil I Canda E Ozyurt BC Eser E 93982320081789920610.1007/s 00467-007-0605-0 · doi ↗ · pubmed ↗
- 5Diagnosis and treatment of nocturnal enuresis in children Korean J Pediatr Hong C Baek M Lee S 1140512008
- 6Bladder dysfunction in children with refractory monosymptomatic primary nocturnal enuresis J Urol Yeung C Chiu H Sit F 1049105416219991045843010.1016/S 0022-5347(01)68062-5 · doi ↗ · pubmed ↗
- 7Nocturnal enuresis in children Curr Opin Pediatr Chandra M 167173101998960889510.1097/00008480-199804000-00010 · doi ↗ · pubmed ↗
- 8Clinical characteristics, nocturnal antidiuretic hormone levels, and responsiveness to DDAVP of school children with primary nocturnal enuresis World J Urol Chang JW Yang LY Chin TW Tsai HL 5675713020122189808410.1007/s 00345-011-0753-5 · doi ↗ · pubmed ↗