Knocking stent release technique to deploy lumen-apposing metal stents during endoscopic ultrasound-guided gallbladder drainage
Takeshi Ogura, Junichi Nakamura, Takafumi Kanadani, Kimi Bessho, Hiroki Nishikawa

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
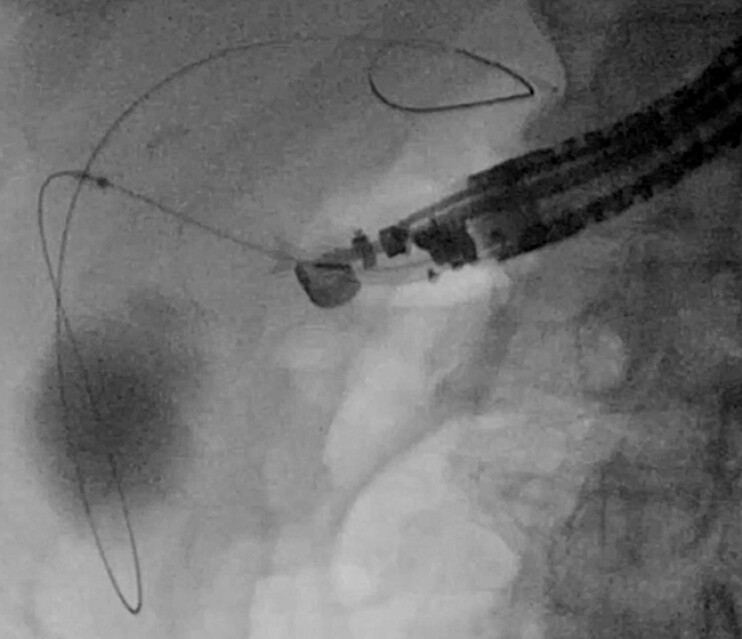 Fig. 1
Fig. 1 Fig. 2
Fig. 2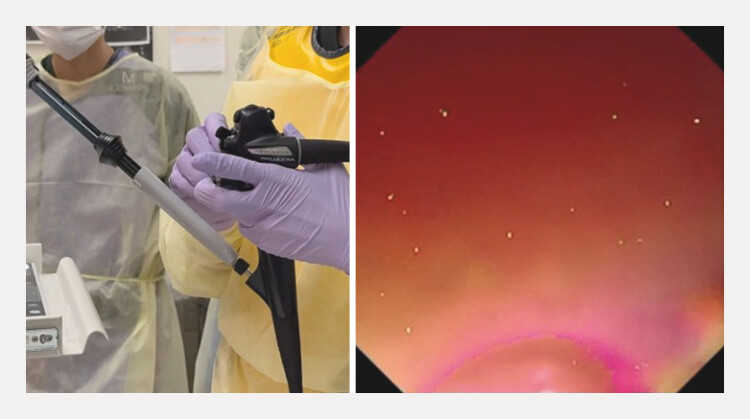 Fig. 3
Fig. 3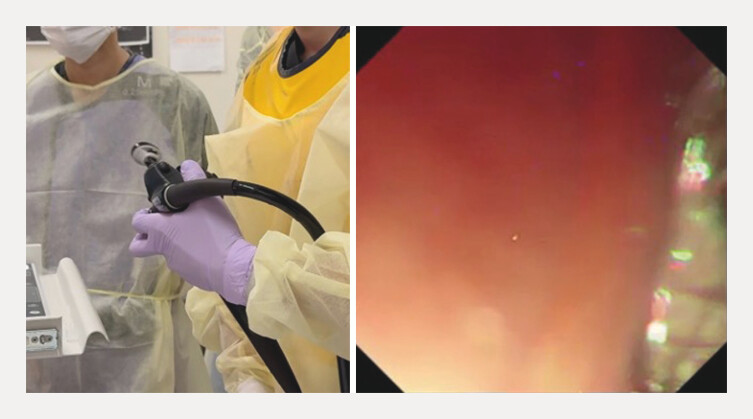 Fig. 4
Fig. 4 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Organ Transplantation Techniques and Outcomes · Esophageal and GI Pathology
Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) using a lumen-apposing metal stent (LAMS; Hot AXIOS, Boston Scientific, Tokyo, Japan) can be performed in patients with contraindications for surgical resection 1 2 3 4 . EUS-GBD can be performed either from the stomach or the duodenum. Although no randomized trial has compared the optimal drainage route, a recent meta-analysis suggests that the duodenal approach may be safer. Compared with the drainage of walled-off necrosis or a pancreatic pseudocyst, the diameter of the target lesion is usually smaller in EUS-GBD. Therefore, a 10- or 15-mm-diameter LAMS is generally selected. However, compared with a 20-mm-diameter LAMS, the anchoring force may be lower. As a result, if stent deployment is performed using the scope-pulling technique, stent dislocation may occur as a complication ( Fig. 1 ). To overcome this adverse event, we usually deploy the LAMS using the “knocking stent release technique.” Technical tips for the knocking stent release technique are presented.
If stent deployment is performed using the scope-pulling technique, stent dislocation may occur as a complication.
An echoendoscope was inserted into the duodenum, and the gallbladder was identified. To prevent double mucosal penetration, the delivery system was advanced to the duodenal wall using the water-filling technique. Then, the delivery system insertion with electrocautery dilation was performed, with successful insertion into the gallbladder. Subsequently, the distal flange was released, and the delivery system was pulled back to the proximal gallbladder wall. Finally, the proximal flange was released using the intra-scope channel release technique ( Fig. 2 ). Next, if the stent release was performed by pulling the echoendoscope, stent dislocation can occur; therefore, first, the right angle of the echoendoscope was applied ( Fig. 3 ), and the scope was then rotated clockwise ( Fig. 4 ). By doing so, the LAMS was partially visualized. Finally, the stent delivery system was knocking, and the stent was finally extracted from the echoendoscope without any adverse events ( Fig. 5 ; Video 1 ).
The proximal flange is released using the intra-scope channel release technique.
The right angle of the echoendoscope is applied.
The scope is rotated clockwise.
The stent delivery system is knocking, and the stent is extracted from the echoendoscope.
The stent delivery system is knocking, and the stent is extracted from the echoendoscope.Video 1
In conclusion, the knocking stent release technique to deploy a LAMS during EUS-GBD might be useful.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hayat M Xiao Y Arain MA Endoscopic Gallbladder Drainage EUS LAMS vs. ERCP Trans-papillary Drainage Curr Gastroenterol Rep 202527510.1007/s 11894-024-00948-239549140 · doi ↗ · pubmed ↗
- 2Canakis A Tugarinov N Deliwala S Clinical outcomes of EUS-guided gallbladder drainage in patients with acute cholecystitis with ≥1 year of follow-up: a systematic review and meta-analysis Gastrointest Endosc 2026103485.6E 1210.1016/j.gie.2025.07.02540706905 · doi ↗ · pubmed ↗
- 3Marasco M Signoretti M Esposito G Endoscopic ultrasonography guided gallbladder drainage: “how and when”Expert Rev Gastroenterol Hepatol 20251939941240082085 10.1080/17474124.2025.2478213 · doi ↗ · pubmed ↗
- 4Fok JCY Teoh AYB Chan SM Endoscopic ultrasound-guided gallbladder drainage for acute cholecystitis Dig Endosc 2025379310210.1111/den.1494639552245 PMC 11718140 · doi ↗ · pubmed ↗