Endoscopic stricturoplasty for pyloric stenosis refractory to endoscopic balloon dilation and lumen apposing metal stenting
Jonathan Rozenberg, Rohit Kumar, William F. Abel, Joel Joseph, Vivek Kesar, Patrick I. Okolo, Varun Kesar

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
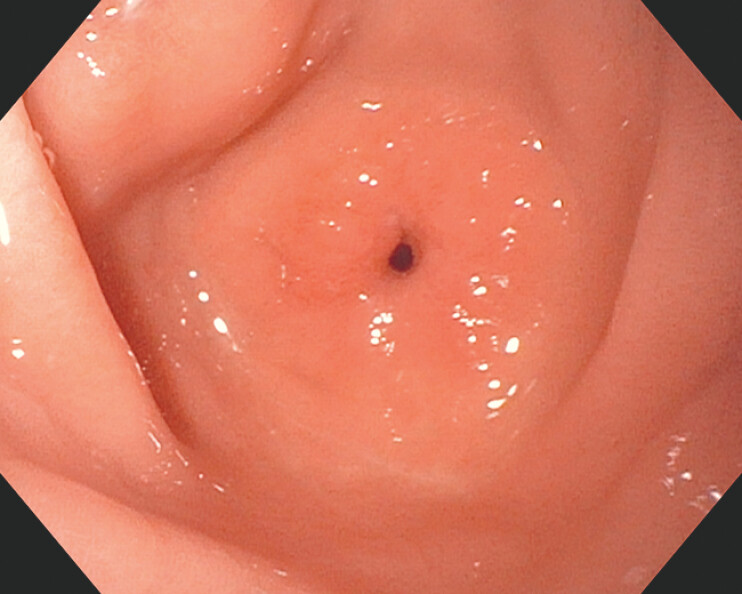 Fig. 1
Fig. 1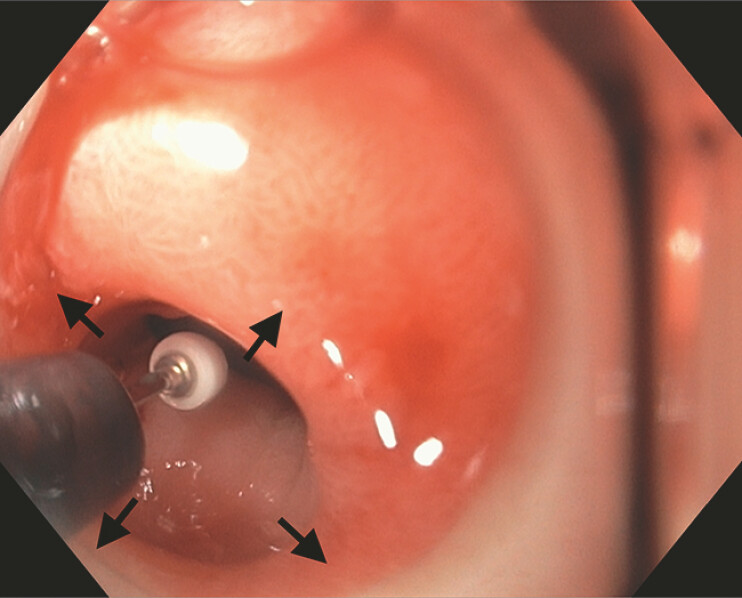 Fig. 2
Fig. 2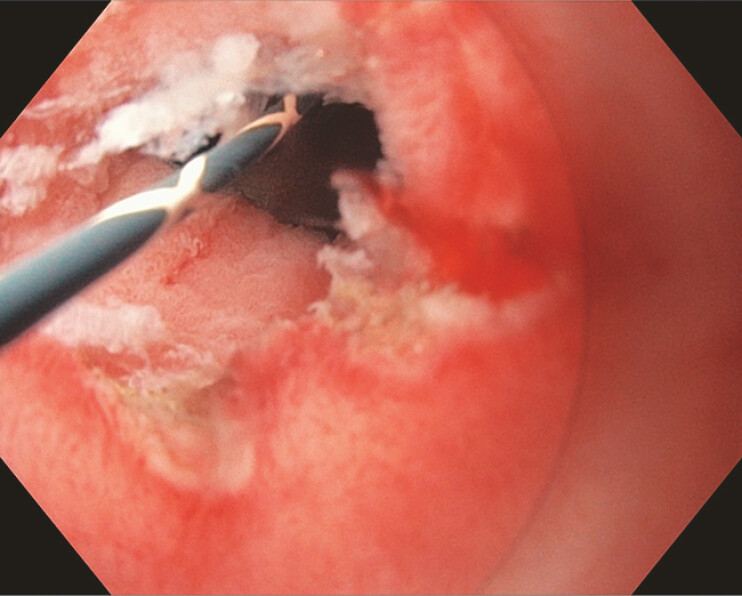 Fig. 3
Fig. 3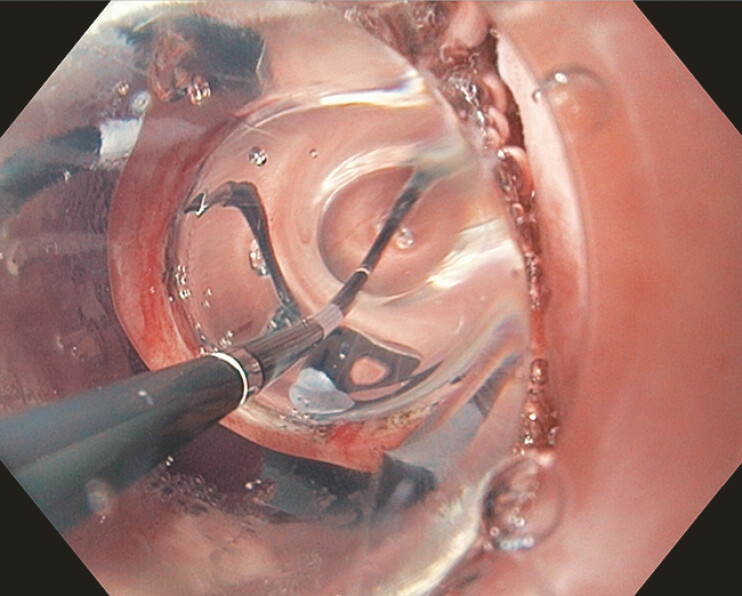 Fig. 4
Fig. 4 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Intestinal Malrotation and Obstruction Disorders · Gallbladder and Bile Duct Disorders
We present a case of a 67-year-old woman with a pertinent past medical history of benign, high-grade pyloric stenosis status after endoscopic balloon dilation (EBD) × 3 and an AXIOS (Boston Scientific, Marlborough, MA, USA) lumen apposing metal stent (LAMS) × 2 who presented for the endoscopic management of symptomatic, recurrent pyloric stenosis. Despite the AXIOS LAMS and EBD therapy, 22- and 7- months prior (respectively), she developed symptomatic recurrence. Esophagogastroduodenoscopy revealed a tight stricture in the distal antrum with associated pyloric stenosis ( Fig. 1 ) that precluded gastroscope passage despite 11–13 mm wire-guided EBD. She underwent endoscopic incisional therapy (EIT) via circumferential stricturoplasty ( Fig. 2 , Fig. 3 ) with an Olympus (Center Valley, PA, USA) insulated tip nano-electrosurgical knife (ITNK). Upon contrast leak absence, 13.5–15.5 mm wire-guided EBD ( Fig. 4 ) was performed which allowed for gastroscope passage ( Fig. 5 ). Intramuscular steroid injections were then performed in the four quadrants of the pylorus. One-month post-EIT, she reported resolution of her symptoms.
Abb. An endoscopic image of a tight stricture in the distal antrum with associated pyloric stenosis.
An endoscopic image depicting insulated tip nano-electrosurgical knife stricturoplasty (ITNKS) in a 3-, 6-, 9- and 12- o’clock or circumferential fashion (black arrows).
An endoscopic image of the pylorus status post-ITNKS revealing extensive underlying fibrotic tissue. ITNKS, insulated tip nano-electrosurgical knife stricturoplasty.
An endoscopic image depicting 13.5–15.5 mm wire-guided endoscopic balloon dilation (EBD) of the pylorus.
A fluoroscopic image depicting the advancement of the gastroscope into the duodenum status post ITNKS. ITNKS, insulated tip nano-electrosurgical knife stricturoplasty.
Initial therapy in the management of gastrointestinal strictures typically involves EBD, especially in patients with inflammatory bowel disease 1 2 and benign pyloric strictures 3 4 . Several sessions of EBD are often required to achieve luminal patency, and strictures can persist/recur despite EBD entailing alternative treatment modalities 1 3 5 . In these cases – namely benign pyloric strictures – LAMS deployment can prove beneficial as it provides sustained dilation 4 ; however, there is a risk of stricture recurrence after LAMS removal. Owing to the possibility of complications (e.g., perforation and stent migration), minimally invasive incisional endoscopic techniques such as ITNK stricturoplasty (ITNKS) have been utilized in the management of benign pyloric strictures with favorable but limited results 3 4 5 . Furthermore, its application in cases that have failed EBD and LAMS therapy are extremely scarce. As such, this case depicts the successful treatment of a pyloric stricture refractory to standard therapy via endoscopic ITNKS ( Video 1 ).
Treatment of symptomatic, recurrent pyloric stenosis refractory to endoscopic balloon dilation and lumen apposing metal stent deployment via insulated tip nano-electrosurgical knife stricturoplasty.Video 1
Endoscopy_UCTN_Code_TTT_1AO_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moroi R Shiga H Kuroha M Endoscopic radial incision and cutting for Crohnʼs Disease-associated intestinal stricture: a pilot study Endosc Int Open 20208 E 81E 8610.1055/a-1027-692131921989 PMC 6949171 · doi ↗ · pubmed ↗
- 2Schulberg JD Hamilton AL Wright EK Repeated endoscopic dilation and needle-knife stricturotomy for Crohnʼs disease strictures Gastrointest Endosc 20251012022.06E 610.1016/j.gie.2024.09.03139343051 · doi ↗ · pubmed ↗
- 3Choi J Endoscopic Incision Therapy for Benign Pyloric Stricture ACG Case Rep J 20229 e 0085510.14309/crj.000000000000085536061254 PMC 9433062 · doi ↗ · pubmed ↗
- 4Chahine A Tavangar A Ho JS 4331 Advanced Endoscopic Techniques for a Refractory Pyloric Stricture Am J Gastroenterol 2023118 S 272610.14309/01.ajg.0000966964.14280.77 · doi ↗
- 5Rahman S Pavan T Agarwal B Mo 1483 Endoscopic Stricturoplasty: a Novel Technique for Symptomatic and Refractory Upper Gastrointestinal Strictures Gastrointest Endosc 201581 AB 43610.1016/j.gie.2015.03.1647 · doi ↗