A novel approach: a pancreatic duct stent removable with the nasobiliary catheter
Haiyong Long, Ping Wang, Wenguang Yang, Yuhong Ren, Bin Yang, Sichao Wen, Mingwen Guo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
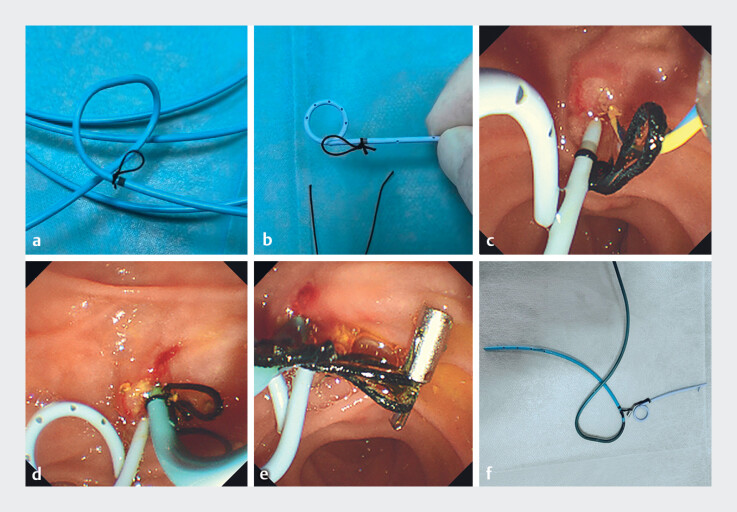 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pancreatitis Pathology and Treatment · Pancreatic and Hepatic Oncology Research
Post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis (PEP) is one of the most common complications of ERCP. Prophylactic pancreatic duct (PD) stent placement is an effective measure to reduce its incidence 1 . However, conventional PD stents require follow-up X-rays for the confirmation of spontaneous dislodgement or a second endoscopy for removal, which imposes additional patient discomfort and financial burden 2 . We designed a novel method that allows for the simultaneous removal of a PD stent along with a nasobiliary catheter (NBC) at the bedside, based on clinical needs.
A 36-year-old woman presented with abdominal pain. Magnetic resonance cholangiopancreatography confirmed choledocholithiasis, and she was scheduled for ERCP ( Video 1 ). Pre-procedure preparation: The NBC and PD stent were pre-modified by tying a surgical suture at their marked positions, forming a loop of approximately 1.5 cm in diameter ( Fig. 1 a, b ). During the ERCP procedure, the guidewire was first advanced into the pancreatic duct and was subsequently retained.
Demonstration of the novel technique for the simultaneous removal of the pancreatic duct stent and nasobiliary catheter after endoscopic retrograde cholangiopancreatography.Video 1
An innovative method: a pancreatic duct stent for removal alongside the nasobiliary catheter. a The surgical suture tied at the marked site of the nasobiliary catheter, and the suture loop diameter is 1.5 cm. b The surgical suture tied at the marked site of the pancreatic duct stent, and the suture loop diameter is 1.5 cm. c Placement of the pancreatic duct stent with the tied suture. d Placement of the nasobiliary catheter with the tied suture. e Titanium clips used to connect the nasobiliary catheter and pancreatic duct stent. f The nasobiliary catheter and pancreatic duct stent connection device.
Using the double-guidewire technique, the bile duct was successfully cannulated ( Video 1 ). The modified PD stent was deployed over the pancreatic guidewire ( Fig. 1 c ). Following balloon extraction of the common bile duct stones ( Video 1 ), the modified NBC was placed ( Fig. 1 d ). A titanium clip was used to securely link the suture loops of the NBC and the PD stent ( Fig. 1 e ). At 48 hours post-procedure, the patient recovered well with no complications such as PEP, bleeding, or infection. The connected NBC-PD stent assembly was removed gently and completely at the bedside ( Video 1 , Fig. 1 f ).
This connected NBC-PD stent assembly offers dual benefits: it secures the PD stent to prevent premature migration and enables its convenient, simultaneous removal with the NBC. This technique effectively obviates the need for additional imaging studies or a repeat endoscopy, presenting a representing and clinically advantageous approach worthy of broader adoption.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dumonceau JM Kapral C Aabakken LERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20205212714910.1055/a-1075-408031863440 · doi ↗ · pubmed ↗
- 2Kahaleh M Freeman M Prevention and management of post-endoscopic retrograde cholangiopancreatography complications Clin Endosc 20124530531210.5946/ce.2012.45.3.30522977824 PMC 3429758 · doi ↗ · pubmed ↗