Successful endoscopic submucosal dissection of a large laterally spreading tumor in distal jejunum by the water pressure method using a newly developed double-balloon enteroscope
Shoma Murata, Kaoru Takabayashi, Motoki Sasaki, Kumiko Kirita, Motohiko Kato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1 Fig. 2
Fig. 2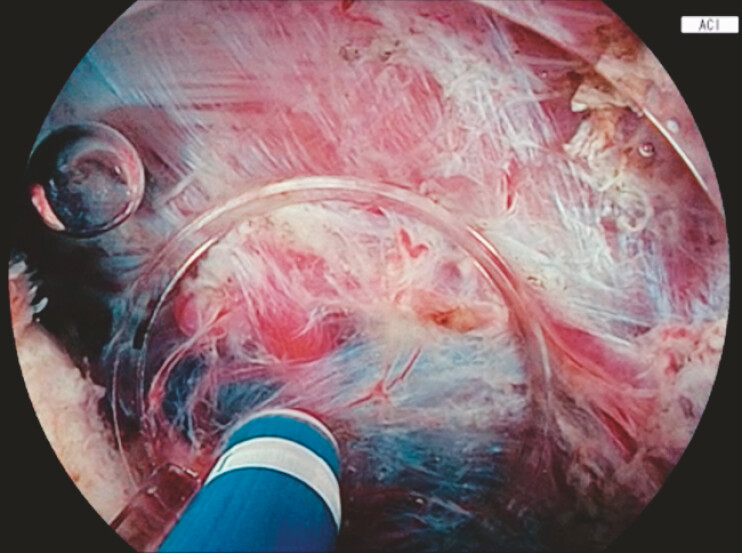 Fig. 3
Fig. 3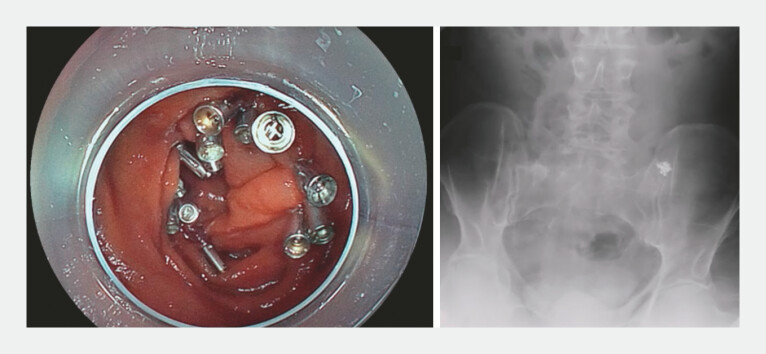 Fig. 4
Fig. 4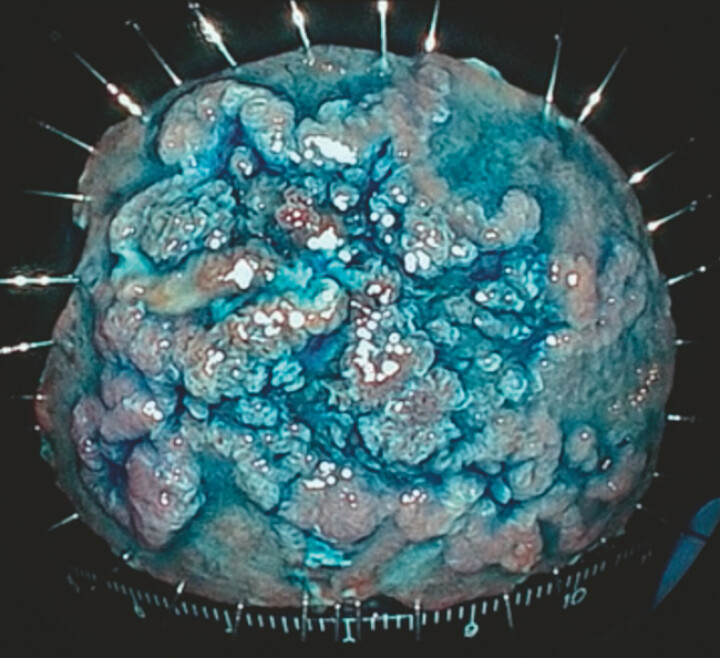 Fig. 5
Fig. 5- —Research grant from Fujifilm Corporation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Gastrointestinal Bleeding Diagnosis and Treatment
Despite advances in therapeutic endoscopy, reports of endoscopic resection in the small intestine remain extremely limited, and only a few cases of endoscopic submucosal dissection (ESD) for proximal small intestinal lesions without deep intubation have been reported 1 . Here, we present a case of distal jejunal ESD performed using a newly developed double-balloon enteroscope ( Video 1 ).
Successful endoscopic submucosal dissection of a large laterally spreading tumor in the distal jejunum by the water pressure method using a newly developed double-balloon enteroscope.Video 1
A man in his fifties with familial adenomatous polyposis was found to have a large tumor in the small intestine. He had a history of total colectomy for rectal cancer. Because of the lesion size, we performed ESD using a double-balloon enteroscope (EN-840T, Fujifilm, Tokyo, Japan). The enteroscope was inserted trans-orally and advanced to the distal jejunum in the pelvis, where a 50-mm laterally spreading tumor was identified. Submucosal injection of hyaluronic acid was initiated from the distal side, followed by complete circumferential mucosal incision. Submucosal dissection was then attempted; however, it was extremely difficult due to poor maneuverability from prior surgery and the narrow submucosal space. Therefore, the enteroscope was withdrawn, and a small-caliber transparent hood (ST hood: DH-33GR, Fujifilm) was attached ( Fig. 1 , Fig. 2 ). The water jet function was then applied for the water pressure method (WPM), which facilitated entry into the narrow submucosal space ( Fig. 3 ) 2 3 . Repeated balloon assisted re-positioning also stabilized maneuverability. Finally, en bloc resection was successfully achieved in 263 minutes without perforation, and the mucosal defect was completely closed with clips ( Fig. 4 , Fig. 5 ). The postoperative course was uneventful except for mild pancreatitis, which resolved conservatively, and the patient was discharged on postoperative day 6.
Appearance of the double-balloon enteroscope with the energy device in place. The energy device used for jejunal ESD was the ORISE 1.5-mm ProKnife (Boston Scientific Japan, Tokyo, Japan). ESD, endoscopic submucosal dissection.
The tip of the double-balloon enteroscope. The ST-hood was modified by cutting off the rubber part and then attached to the tip of the enteroscope, and the balloon tip of the enteroscope also functioned without issues.
Amber-red color imaging (ACI) during the ESD with the water pressure method. ACI enhances the visualization of the dissection plane within the very thin submucosal layer.
A white light image and an abdominal radiography after complete suturing of the mucosal defect. The mucosal defect was completely closed by the origami method using endoscopic clips (SureClip; Boston Scientific Japan, Tokyo, Japan). The radiographic image indicates that the treated lesion was identified in the pelvis, and the procedure was completed without perforation.
A white light image of the specimen with indigo carmine. En-bloc resection was successfully achieved. Pathological diagnosis: Tubular adenoma, intestinal type, pHM0, and pVM0.
To the best of our knowledge, this is the first successful case of distal jejunal ESD. The newly developed double-balloon enteroscope enabled access to the deep small intestine and, with the aid of the water jet function, facilitated precise submucosal dissection using WPM, thereby overcoming the technical difficulties of small intestinal ESD.
Endoscopy_UCTN_Code_TTT_1AP_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iida M Sakamoto H Miura Y Jejunal endoscopic submucosal dissection is feasible using the pocket-creation method and balloon-assisted endoscopy Endoscopy 20185093193210.1055/a-0626-689329954004 · doi ↗ · pubmed ↗
- 2Yahagi N Nishizawa T Sasaki M Water pressure method for duodenal endoscopic submucosal dissection Endoscopy 20174922722810.1055/s-0043-11355628759932 · doi ↗ · pubmed ↗
- 3Kato M Takatori Y Sasaki M Water pressure method for duodenal endoscopic submucosal dissection (with video)Gastrointest Endosc 20219394294932853646 10.1016/j.gie.2020.08.018 · doi ↗ · pubmed ↗