Myocardial Protection Efficacy of Custodiol, Del Nido, and Cold Intermittent Blood Cardioplegia in Arterial Switch Operation
Mustafa Kemal Avşar, Yasin Güzel, Barış Kırat, İbrahim Özgür Önsel, Cenap Zeybek, Deniz Yorgancılar, İlker Kemal Yücel

TL;DR
This study compares three heart protection methods during a critical heart surgery in newborns, finding that Custodiol and Del Nido offer better outcomes than traditional cold blood cardioplegia.
Contribution
The study provides new comparative evidence on myocardial protection efficacy in neonates undergoing arterial switch operation.
Findings
Custodiol and Del Nido cardioplegia reduced cross-clamp and bypass times compared to cold blood cardioplegia.
Custodiol and Del Nido resulted in lower troponin I levels and reduced inotropic support needs.
Ventilation and ICU stays were shorter with Custodiol and Del Nido compared to cold blood cardioplegia.
Abstract
The arterial switch operation (ASO) is the standard treatment for transposition of the great arteries (TGA), requiring robust myocardial protection due to the neonatal myocardium’s vulnerability to ischaemia. This study compares the myocardial protective efficacy of Custodiol, Del Nido, and cold intermittent blood cardioplegia in neonates undergoing ASO. We retrospectively analysed 133 neonates with TGA undergoing ASO (2013-2024) at 4 Turkish centres, grouped by cardioplegia: cold blood (n = 47), Custodiol (n = 44), or Del Nido (n = 42). Outcomes included aortic cross-clamp and cardiopulmonary bypass times, troponin I, CK-MB, inotropic support, and ventilation duration. Custodiol and Del Nido had shorter cross-clamp (70.4 (8.5) vs 68.7 (7.9) vs 78.2 (9.1) minutes, P < .001) and bypass times (P = .004), lower troponin I (4.2 (1.3) vs 4.0 (1.5) vs 6.8 (1.9) ng/mL, P < .001), reduced…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
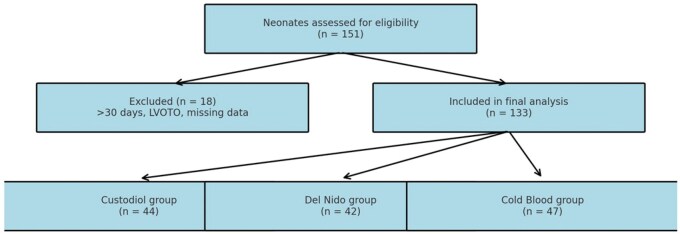 Figure 1
Figure 1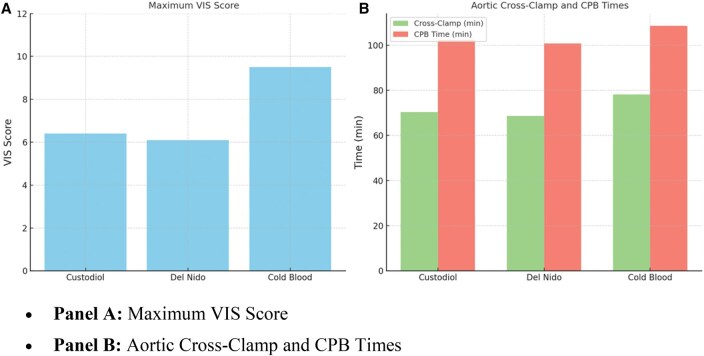 Figure 2
Figure 2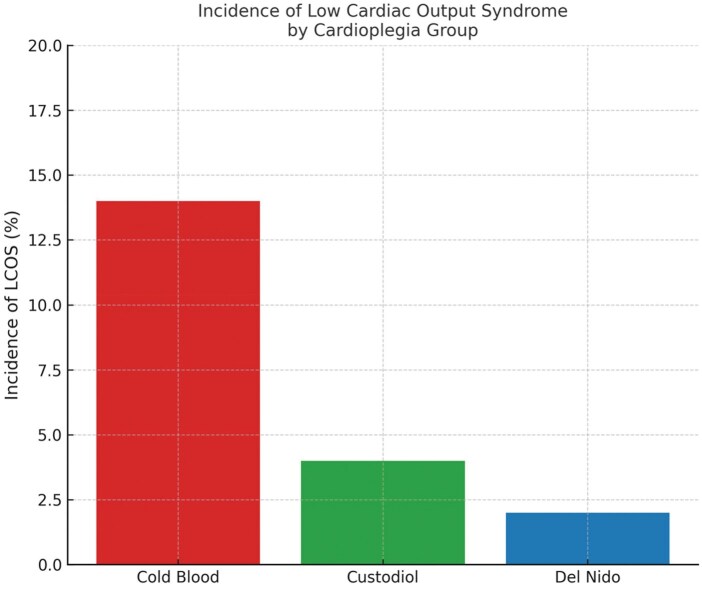 Figure 3
Figure 3| Variable | Custodiol ( | Del Nido ( | Cold blood ( |
|
|---|---|---|---|---|
| Age at surgery (days) | 10.3 (2.2) | 13.9 ± 2.3 | 17.4 (1.5) | <.0001 |
| Birth weight (kg) | 2.7 (0.2) | 3.2 ± 0.2 | 3.3 (0.3) | <.0001 |
| Preoperative oxygen saturation (%) | 58.0 (5.6) | 73.7 ± 5.3 | 84.3 (5.4) | <.0001 |
| Preoperative inotropic support, | 33 (75%) | 27 (64%) | 22 (47%) | .0152 |
| Presence of VSD, | 26 (59%) | 18 (43%) | 25 (53%) | .3347 |
| Presence of ASD or PFO, | 32 (73%) | 26 (62%) | 33 (70%) | .5035 |
| Balloon atrial septostomy, | 15 (34%) | 11 (26%) | 8 (17%) | .1704 |
| Preoperative lactate (mmol/L) | 4.8 (2.0) | 4.6 (1.3) | 3.2 (1.1) | <.0001 |
| Variable | Custodiol ( | Del Nido ( | Cold blood ( |
|
|---|---|---|---|---|
| Presence of VSD (%) | 59.0 | 43.0 | 53.0 | .33 |
| Aortic coarctation (%) | 9.0 | 2.0 | 4.0 | .18 |
| Intramural LMCA (%) | 4.5 | 4.8 | 4.2 | .96 |
| Single coronary origin (%) | 11.4 | 7.1 | 6.3 | .59 |
| Retroaortic circumflex (%) | 4.5 | 4.8 | 2.1 | .60 |
| Aortic root orientation: AP (%) | 86.0 | 86.0 | 89.0 | .87 |
| Aortic root orientation: side-by-side (%) | 14.0 | 14.0 | 11.0 | .87 |
| Single coronary ostium (%) | 11.4 | 7.1 | 6.3 | .59 |
| Intramural coronary course (%) | 4.5 | 4.8 | 4.2 | .96 |
| Aortic arch anomaly (%) | 9.0 | 2.0 | 4.0 | .23 |
| Parameter | Cold blood ( | Custodiol ( | Del Nido ( |
|
|---|---|---|---|---|
| Aortic cross-clamp time (minutes) | 78.2 (9.1) | 70.4 (8.5) | 68.7 (7.9) | <.001 |
| CPB time (minutes) | 108.6 (11.2) | 102.3 (10.5) | 100.8 (9.8) | .004 |
| Cardioplegia volume (mL) | 320 (60) | 500 (50) | 400 (40) | <.001 |
| Need for repeat cardioplegia dose, | 47 (100%) | 0 (0%) | 4 (8%) | <.001 |
| Need for defibrillation upon reperfusion, | 9 (18%) | 3 (6%) | 2 (4%) | .034 |
| Time to spontaneous sinus rhythm (minutes) | 4.6 (2.2) | 3.1 (1.6) | 2.9 (1.7) | .002 |
| Postoperative sixth hour troponin I (ng/mL) | 6.8 (1.9) | 4.2 (1.3) | 4.0 (1.5) | <.001 |
| Postoperative sixth hour CK-MB (U/L) | 72.5 (15.6) | 51.3 (12.1) | 48.9 (10.4) | <.001 |
| Lactate (postoperative sixth hour, mmol/L) | 3.8 (1.0) | 2.9 (0.8) | 2.7 (0.7) | <.001 |
| Maximum inotropic score (first 24 hours) | 9.5 (3.1) | 6.4 (2.2) | 6.1 (2.0) | <.001 |
| Duration of mechanical ventilation (hour) | 16.8 (4.5) | 13.2 (3.9) | 12.9 (3.6) | .001 |
| Reintubation after extubation, | 5 (10%) | 1 (2%) | 1 (2%) | .09 |
| Length of ICU stay (days) | 4.2 (1.3) | 3.5 (1.2) | 3.4 (1.0) | .010 |
| Hospital stay (days) | 9.1 (2.5) | 8.3 (2.3) | 8.2 (2.0) | .071 |
| Low cardiac output syndrome, | 7 (14%) | 2 (4%) | 1 (2%) | .048 |
| 30-day mortality, | 3 (6.4%) | 1 (2.4%) | 2 (4.5%) | .47 |
| Delayed sternal closure | 14 (29.8%) | 9 (20.5%) | 7 (16.7%) | .308 |
| Variable | Overall | Custodiol vs Del Nido | Custodiol vs Cold blood | Del Nido vs Cold blood |
|---|---|---|---|---|
| Age | <.001 | NS |
|
|
| Weight | .008 | NS |
|
|
| VIS Score | .006 | NS ( |
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management
INTRODUCTION
Transposition of the great arteries (TGA) is a critical congenital heart defect requiring arterial switch operation (ASO).1 Performed within the first 2 weeks, ASO demands robust myocardial protection due to the neonatal myocardium’s susceptibility to ischaemia from immature metabolic pathways.2^,^3 Cardioplegia solutions minimize ischaemia-reperfusion injury during cardiopulmonary bypass (CPB), but the optimal strategy for neonates remains debated.4^,^5
Cold blood cardioplegia has long been a reliable standard, despite its drawbacks of frequent dosing and prolonged operative times.6 In contrast, Custodiol and Del Nido solutions, designed for single-dose administration and prolonged myocardial protection, have emerged as promising alternatives in both paediatric and adult cardiac surgery.6–8 However, their efficacy in neonates is controversial.8–13 This study compares Custodiol, Del Nido, and cold blood cardioplegia in 133 neonates undergoing ASO, assessing intraoperative and postoperative outcomes to guide myocardial protection strategies.
METHODS
Study design and centres
This retrospective cohort study compared Custodiol, Del Nido, and cold blood cardioplegia in 133 neonates undergoing ASO for TGA. A single congenital cardiac surgeon performed all operations (2013-2024) across 4 centres. Cardioplegia strategy evolved over time: cold blood (2013-2016), Del Nido (2016-2020), and Custodiol (2020-2024). Patient selection is shown in Figure 1. Patients were grouped by cardioplegia:
Flow Diagram Illustrating the Patient Selection Process for the Comparative Analysis of Cardioplegia Methods in 133 Neonates Undergoing Arterial Switch Operation. Exclusion criteria included age >30 days, missing data, and presence of left ventricular outflow tract obstruction (LVOTO)
Cold blood (n = 47)Custodiol (n = 44)Del Nido (n = 42)
Inclusion criteria
Neonates were included if they met the following criteria:
Confirmed diagnosis of d-TGA, with or without associated intracardiac anomalies (eg, ventricular septal defect [VSD], atrial septal defect [ASD], patent ductus arteriosus [PDA]).Underwent primary ASO performed under CPB with cardioplegic arrest.Surgery timing based on anatomical subtype:
- Simple d-TGA with intact ventricular septum (IVS): surgery within the first 15 days of life
- d-TGA with VSD: surgery within the first 30 days of life Complete intraoperative and early postoperative data available, including aortic cross-clamp time, troponin I, CK-MB, inotropic support, and ventilation duration.
Exclusion criteria
Underwent procedures other than ASO.Received staged palliation instead of primary ASO.Were older than 30 days at the time of surgery.Had major extracardiac anomalies or known genetic syndromes that could affect surgical outcomes.Had incomplete intraoperative or early postoperative data.Had TGA with left ventricular outflow tract obstruction (LVOTO).
Cardioplegia protocols
Cold intermittent blood cardioplegia
A cardioplegic solution composed of oxygenated blood and crystalloid in a 4:1 ratio, containing potassium chloride (25 mmol/L), sodium bicarbonate (10 mmol/L), and mannitol (30 mmol/L). It was administered antegrade at 4-8 °C and repeated every 15 minutes throughout the cross-clamp period.
Custodiol (HTK solution)
A crystalloid-based, intracellular-type cardioplegia composed of histidine (198 mmol/L), potassium chloride (9 mmol/L), magnesium chloride (4 mmol/L), tryptophan (2 mmol/L), α-ketoglutarate (1 mmol/L), and mannitol (30 mmol/l). It was administered antegrade at 4-8 °C as a single dose of 50 ml/kg over 3-5 minutes, providing up to 180 minutes of myocardial protection.
Del Nido cardioplegia
A 4:1 blood-to-crystalloid mixture based on Plasma-Lyte A, containing lidocaine (1 mmol/L), potassium chloride (13 mmol/L), magnesium sulphate (16 mmol/L), mannitol (30 mmol/L), and sodium bicarbonate (13 mmol/L). It was delivered antegrade at 4 °C over 3-5 minutes, offering myocardial protection for 60-90 minutes.
Surgical technique and patient selection
All procedures were performed via median sternotomy under standardized general anaesthesia.
Cardiopulmonary bypass was established using aortic and bicaval cannulation under mild hypothermia (30-32 °C). CPB flow rate was maintained at 150-170 ml/kg/minutes, with a target mean arterial pressure of 30-40 mmHg. Haematocrit was maintained at 28%-32%; MUF was applied post-CPB.
Myocardial protection was achieved via antegrade infusion of 1 of the 3 cardioplegia solutions immediately after aortic cross-clamping: cardioplegia administration was performed as described in Section “Cardioplegia protocols”.
Arterial switch operation was performed using standard techniques, including Lecompte manoeuvre and coronary reimplantation (trap-door technique). Associated intracardiac anomalies (eg, VSD, aortic coarctation) were repaired concurrently. In cases with aortic arch obstruction, an extended end-to-end anastomosis was performed under circulatory arrest or low-flow CPB as needed. Coronary artery transfer used the trap-door technique, except in 6 patients (4.5%) with intramural left main coronary artery (LMCA), where unroofing and patch augmentation (typically autologous pericardium) were applied. Sixteen patients (12%) had single coronary ostium or atypical coronary patterns (eg, retroaortic circumflex, anterior looping), requiring individualized implantation strategies. No intraoperative or early postoperative coronary-related complications were observed.
The mean anaesthetic induction time (from induction to skin incision) was 35 ± 8 minutes, consistent across groups. No significant changes were made to operative or anaesthetic protocols during the study period. Patients with complex anatomical anomalies, such as LVOTO, were excluded to ensure homogeneity in myocardial protection assessment.
Anatomical characteristics included:
VSD in 69 patients (51.8%).Aortic coarctation in 7 patients (5.3%).Coronary anomalies: intramural LMCA in 6 patients (4.5%), single coronary artery origin in 11 patients (8.3%), retroaortic circumflex in 5 patients (3.8%).Great artery orientation: anterior-posterior in 116 patients (87.2%), side-by-side in 17 patients (12.8%).
Echocardiographic assessment
Transthoracic echocardiography (TTE) was performed preoperatively, early postoperatively (within 1 hour), and at hospital discharge using standard imaging protocols. Left ventricular function was assessed qualitatively (normal, mild, moderate, or severe dysfunction) and quantitatively via left ventricular ejection fraction (LVEF) using the Simpson biplane method when feasible. Regional wall motion abnormalities (RWMA) were evaluated in apical 4-chamber, parasternal long-axis, and parasternal short-axis views. Most patients showed prompt ventricular function recovery post-reperfusion, with moderate-to-severe RWMA incidence below 5% at discharge. Three patients developed low cardiac output syndrome (LCOS) requiring inotropic and ventilatory support in the intensive care unit.
Postoperative outcome measures
Postoperative outcomes included cross-clamp and CPB times, troponin I, CK-MB, vasoactive-inotropic score (VIS), ventilation duration, and intensive care unit (ICU) stay. VIS was calculated within 24 hours postoperation based on inotropic doses. VIS was calculated using the following formula: dopamine (μg/kg/minute) + dobutamine (μg/kg/minute) + 100 × epinephrine (μg/kg/minute) + 10 × milrinone (μg/kg/minute) + 10 000 × vasopressin (U/kg/minute) + 100 × norepinephrine (μg/kg/minute). Peak VIS within the first 24 hours postoperatively was recorded. All centres followed similar inotropic protocols based on national paediatric cardiac ICU recommendations.
Troponin I and CK-MB were measured serially postoperation to assess myocardial injury. Low cardiac output syndrome was defined as requiring inotropic and ventilatory support due to inadequate cardiac output, confirmed by echocardiographic ventricular dysfunction.
Postoperative management and sternal closure strategy
Postoperative care protocols were broadly similar across all 4 centres. Early extubation and fast-track ICU discharge were encouraged when haemodynamic stability permitted. Minor differences in timing existed due to institutional practices, but the overall management approach was consistent.
All patients underwent attempted primary chest closure in the operating room. However, delayed sternal closure was performed in cases of haemodynamic instability or excessive bleeding. A total of 30 patients (22.6%) underwent delayed chest closure, including 9 in the Custodiol group (20.5%), 7 in the Del Nido group (16.7%), and 14 in the Cold Blood group (29.8%).
Statistical analysis
Analyses used SPSS 26.0. Continuous variables (mean (SD) or median [IQR]) were compared via ANOVA or Kruskal-Wallis tests; categorical variables (n, %) via chi-square or Fisher’s exact tests (P < .05 significant). Normality was assessed using Shapiro-Wilk test. Normal variables used 1-way ANOVA with Bonferroni correction; non-normal variables used Kruskal-Wallis with Dunn’s post hoc test. AUC for hs-cTnI was calculated to assess myocardial injury and compared using ANOVA or Kruskal-Wallis based on distribution. Complete data for all patients’ primary and secondary outcomes allowed complete-case analysis without imputation.
RESULTS
Baseline characteristics
Of the 133 neonates undergoing ASO for TGA, 44 received Custodiol, 42 Del Nido, and 47 cold blood cardioplegia. Baseline characteristics (Table 1) differed in age, birth weight, preoperative oxygen saturation, and inotropic support (P < .05), reflecting clinical heterogeneity.
Surgical and anatomical complexity variables are summarized in Table 2.
Intraoperative and early postoperative outcomes
Custodiol and Del Nido groups showed shorter cross-clamp (70.4 (8.5) and 68.7 (7.9) vs 78.2 (9.1) minutes, P < .001) and CPB times (102.3 (10.5) and 100.8 (9.8) vs 108.6 (11.2) minutes, P = .004) than cold blood (Table 2). Custodiol had the highest cardioplegia volume (500 (50) ml), followed by Del Nido (400 (40) ml) and cold blood (320 (60) ml, P < .001). Repeat dosing occurred in 100% of cold blood, 8% of Del Nido, and 0% of Custodiol cases (P < .001). Custodiol and Del Nido had faster sinus rhythm recovery (P = .002) and fewer defibrillations (P = .034). Troponin I and CK-MB, measured at 6-72 hours across centres, used standardized assays. Custodiol and Del Nido had lower postoperative troponin I (4.2 (1.3) and 4.0 (1.5) vs 6.8 (1.9) ng/mL, P < .001), CK-MB, lactate, and inotropic scores (P < .001), plus shorter ventilation (13.2 (3.9) and 12.9 (3.6) vs 16.8 (4.5) hours, P = .001) and ICU stays (3.5 (1.2) and 3.4 (1.0) vs 4.2 (1.3) days, P = .010). LCOS was less frequent in Custodiol (4%) and Del Nido (2%) vs cold blood (14%, P = 0.048). Thirty-day mortality was similar (2.4%-6.4%, P = .47). Delayed sternal closure occurred in 30 patients (22.6%) due to low cardiac output or bleeding: Custodiol (n = 9), Del Nido (n = 7), cold blood (n = 14) (Table 3).
Post hoc comparisons for significant variables (Table 4) showed lower age, weight, and VIS scores in Custodiol and Del Nido versus cold blood (P < .05), with no differences between Custodiol and Del Nido. This supports their clinical comparability and reduced inotropic needs. Cardiopulmonary bypass and cross-clamp times differed significantly between cold blood and both the groups, but not between Custodiol and Del Nido. Early postoperative echocardiographic assessments (within 48 hours) showed preserved LVEF (≥55%) in 124 patients (93.2%), with no group differences (Custodiol: 94.4%, Del Nido: 95.5%, cold blood: 89.2%; P = .41). Mild pericardial effusion occurred in 9 patients (6.8%), needing no intervention. Transient ventricular dysfunction (EF <50%) affected 6 patients (4.5%), mostly in cold blood (n = 4, P = .26). Troponin I levels, measured at 6-72 hours (Figure 1), were lower in Custodiol and Del Nido than cold blood (P < .001). Cold blood had higher VIS (P < .001), indicating greater myocardial support need (Figure 2A). Custodiol and Del Nido had shorter operative times (P < .01), likely due to single-dose efficiency (Figure 2B). Figure 3 highlights single-dose strategies’ myocardial protection.
Troponin area under the curve and regression analysis
Troponin AUC, calculated over 72 hours, assessed myocardial injury. Mean AUC values were 14.2 (3.1) ng hour/mL (Del Nido), 14.7 (3.3) ng hour/mL (Custodiol), and 17.6 (3.9) ng hour/mL (cold blood) (P < .001). Post hoc analysis showed lower AUC in Del Nido and Custodiol versus cold blood, with no difference between them. Multivariable regression, adjusting for cross-clamp and CPB times (Table S1), confirmed Custodiol and Del Nido’s association with lower troponin AUC versus cold blood.
Postoperative mortality analysis
Six neonates (4.5%) died within 30 days postoperatively. In the cold blood group, 3 deaths occurred: 2 after emergency surgery and ECMO for severe preoperative acidosis, on days 16 (sepsis, multiorgan dysfunction) and 25 (post-ECMO weaning); 1 on day 4 from ventricular fibrillation despite normal biventricular function. In the Del Nido group, 2 deaths occurred: 1 after ECMO for LCOS, on day 21 (multiorgan dysfunction); another with low birth weight (2.4 kg), on day 16 (sepsis, prolonged ventilation). In the Custodiol group, 1 death occurred after ECMO for severe preoperative acidosis, on day 23 (sepsis, multiorgan failure).
DISCUSSION
Myocardial protection strategies in neonatal cardiac surgery remain heterogeneous, reflecting both the lack of consensus on optimal cardioplegia solutions and the unique challenges of the immature neonatal myocardium.14–16 In 133 neonates undergoing ASO, Custodiol and Del Nido cardioplegia outperformed cold blood cardioplegia, with shorter cross-clamp and CPB times, lower myocardial injury markers, and reduced inotropic needs, likely due to their single-dose design minimizing intraoperative interruptions.
Paediatric cardiac surgery preferences vary: North American centres favour Del Nido for simplicity and cost-effectiveness, European centres use both Custodiol and Del Nido,15 while Chinese hospitals prefer cold blood cardioplegia.17 Our cohort’s Custodiol and Del Nido groups had shorter operative times than blood (Figure 2).
(A) Comparison of maximum vasoactive-inotropic scores (VIS) during the first 24 hours postoperatively among Custodiol, Del Nido, and cold blood cardioplegia groups. (B) Comparison of aortic cross-clamp and cardiopulmonary bypass (CPB) durations across cardioplegia strategies. Single-dose groups (Custodiol and Del Nido) showed shorter operative times. Error bars represent standard deviation
Giordano et al11 reported similar Custodiol-related reductions but higher troponin I levels, unlike our findings. Floh et al18 found no operative time benefits with Del Nido, possibly due to case complexity. The neonatal myocardium’s vulnerabilities require tailored protection.15–16^,^19
Single-dose cardioplegia (Custodiol and Del Nido) reduces coronary manipulation, likely minimizing endothelial trauma in ASO coronary reimplantation. In our series, 19 patients (14.3%) with intramural LMCA and 16 (12%) with other coronary anomalies had no ischaemic events, suggesting single-dose strategies’ advantage in such cases.
Troponin I and CK-MB are key indicators of cardioplegia efficacy. Figure 2 shows lower hs-cTnI levels at 6-72 hours in Custodiol (4.2 ± 1.3 ng/mL at 6 hours) and Del Nido (4.0 ± 1.5 ng/mL) versus cold blood (6.8 ± 1.9 ng/mL, P < .001), indicating better myocardial protection. Cumulative hs-cTnI AUC was lower in Del Nido and Custodiol than cold blood (P = .004), with no difference between them (P = .61).Single-dose cardioplegia’s favourable myocardial effects align with Pérez-Andreu et al20 (reduced enzyme leakage post-ASO with Custodiol) and Mohammed et al13 (lower troponin I with Del Nido). Yet, Bojan et al16 reported higher troponin I with Custodiol versus warm blood cardioplegia, indicating temperature and delivery protocols’ impact.
AUC analysis of troponin levels confirmed less myocardial injury in the Custodiol and Del Nido groups, supporting their clinical benefit. Mylonas et al21 found no troponin difference between blood and crystalloid cardioplegia, suggesting comparable modern techniques. Lower troponin likely indicates better myocardial preservation, evidenced by reduced inotropic needs and LCOS incidence, a key protective effect in high-risk neonates. Linear regression using troponin AUC as the dependent variable, with cardioplegia type, cross-clamp time, and CPB duration as covariates, confirmed Del Nido and Custodiol’s association with lower troponin release versus cold blood.
Single-dose cardioplegia enhances early postoperative recovery. The Custodiol and Del Nido groups showed faster sinus rhythm recovery and lower defibrillation rates, likely due to depolarized arrest (eg, lidocaine in Del Nido) reducing reperfusion arrhythmias.6^,^13
** Figure 3 ** shows lower maximum VIS in Custodiol (6.4 ± 2.2) and Del Nido (6.1 ± 2.0) versus cold blood (9.5 ± 3.1, P < .001), indicating less myocardial support need. This aligns with Mohammed et al13 and Pérez-Andreu et al,20 suggesting single-dose cardioplegia better preserves cardiac function. Figure 3 shows lower LCOS incidence in Custodiol (4%) and Del Nido (2%) versus cold blood (14%, P = .048), highlighting single-dose strategies’ myocardial protection. Early postoperative echocardiographic parameters (LVEF, pericardial effusion, transient dysfunction) were similar across groups, supporting Custodiol and Del Nido’s protective effect. Dolcino et al22 noted prolonged cross-clamp times with Custodiol may increase LCOS risk, not seen in our cohort due to strict ischaemic time control. Floh et al18 found no decrease in ventricular dysfunction with Del Nido, highlighting the need for standardized outcome measures. No 30-day mortality differences (P = .47) across the groups confirm the safety of all 3 strategies. Two emergency surgery/ECMO patients, included to reflect real-world practice, may affect early outcomes but were noted as a limitation. Their inclusion enhances external validity, though future studies may exclude such high-risk cases to reduce confounding.
Incidence of Low Cardiac Output Syndrome (LCOS) Within the First 24 hours Postoperatively. Both Custodiol and Del Nido Groups Demonstrated Significantly Lower LCOS Rates Compared to the Cold Blood Cardioplegia Group (P = .048)
Each cardioplegia strategy has unique strengths and weaknesses. Custodiol’s single-dose protection (up to 120 minutes) simplifies complex coronary transfers.19 Its high volume may cause hemodilution, risking postoperative anaemia, oedema, or hyponatremia, potentially leading to seizures.7^,^19^,^23
Dolcino et al22 noted prolonged cross-clamp times with Custodiol may increase neonatal LCOS risk, requiring careful ischaemic time monitoring. Münch et al24 emphasized Custodiol’s efficacy relies on strict 4-8 °C temperature control to prevent rewarming-induced myocardial arrest failure and reperfusion injury. MUF and precise temperature management mitigate these risks.4^,^5^,^25 Del Nido’s blood-crystalloid mix reduces hemodilution, offering 60-90 minutes of protection,5 with lidocaine-induced hyperpolarized arrest likely minimizing reperfusion injury, supported by our lower troponin levels.12^,^13
Cold intermittent blood cardioplegia, though needing frequent dosing, benefits from oxygenated perfusate and familiarity, suiting prolonged procedures.14 Its repeated coronary manipulations risk endothelial trauma in neonates with small coronary ostia. Our 4.5% mortality rate matches ASO standards,11^,^13 with no coronary-related deaths. Anatomical risk factors (eg, single ostium, intramural coronaries, arch anomalies) were evenly distributed across groups (Table 3), ensuring cohort comparability. This supports the validity of differences in myocardial injury markers and early outcomes. Baseline differences (age, weight) limit findings, warranting multivariate analyses in future studies.
Post hoc analysis revealed cold blood patients were older, heavier, with higher VIS, while the Custodiol and Del Nido groups were similar. This indicates their clinical comparability, suggesting outcome differences are not solely due to baseline variability. An ongoing trial26 could identify optimal strategies.
Custodiol and Del Nido improve ASO efficiency and outcomes. Surgeons should tailor cardioplegia to patient factors with strict protocols for optimal myocardial protection. Our observational design, lacking multivariable adjustment, limits causal inference. Though ventilation duration and ICU stay differences were significant, their individual clinical impact is modest. In neonatal care, small ICU resource savings can yield significant benefits in high-volume centres or fragile populations, balancing our interpretation.
CONCLUSION
Neonatal myocardial protection remains a critical challenge in ASO due to the immature myocardium’s susceptibility to ischaemic injury. This retrospective multicentre study of 133 neonates suggests that Custodiol and Del Nido cardioplegia may offer improved efficiency and outcomes, including shorter cross-clamp times, less myocardial injury, and reduced inotropic needs. Each strategy—Custodiol’s prolonged single-dose protection, Del Nido’s balanced blood-crystalloid composition, and cold blood’s oxygenated perfusate—offers unique advantages, but also limitations such as hemodilution, reperfusion injury risk, or frequent dosing needs. Surgeons should consider tailoring cardioplegia selection to patient-specific factors, including coronary anatomy and anticipated surgical complexity, while ensuring meticulous delivery to optimize myocardial preservation. Given the observational nature of this study, these findings should be interpreted with caution and confirmed in prospective randomized trials.
Strengths and limitations
This study’s strengths include its multicentre design, standardized operative protocols, and comprehensive postoperative biomarker analysis. However, the retrospective nature of the analysis, small sample size, and lack of multivariable adjustment limit the strength of causal inference. Given the inherent limitations of observational design and absence of multivariable adjustment, the results should be interpreted as associative rather than definitive.
Supplementary Material
ivaf215_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cain MT , Cao Y, Ghanayem NS, et al Transposition of the great arteries—outcomes and time interval of early neonatal repair. World J Pediatr Congenit Heart Surg. 2014;5:241-247. 10.1177/215013511352055924668972 · doi ↗ · pubmed ↗
- 2Hamada S , Frick M, Marx N, Brehmer K, Manka R. Severe myocardial ischaemia after neonatal arterial switch operation. Eur Heart J. 2015;36:3214. 10.1093/eurheartj/ehv 14725926561 · doi ↗ · pubmed ↗
- 3Dibardino DJ , Allison AE, Vaughn WK, et al Current expectations for newborns undergoing the arterial switch operation. Ann Surg. 2004;239:588-596. 10.1097/01.sla.0000124293.52814.a 715082962 PMC 1356266 · doi ↗ · pubmed ↗
- 4Talwar S , Jha AJ, Hasija S, et al Paediatric myocardial protection-strategies, controversies and recent developments. Indian J Thorac Cardiovasc Surg. 2013;29:114-123. 10.1007/s 12055-013-0208-2 · doi ↗
- 5Elmahrouk AF , Shihata MS, Al-Radi OO, et al Custodiol versus blood cardioplegia in pediatric cardiac surgery: a randomized controlled trial. Eur J Med Res. 2023;28:404. 10.1186/s 40001-023-01372-437798628 PMC 10552411 · doi ↗ · pubmed ↗
- 6Matte GS , del Nido PJ. History and use of del Nido cardioplegia solution at Boston Children’s Hospital. J Extra Corpor Technol. 2012;44:98-103. PMID:2319838923198389 PMC 4557532 · pubmed ↗
- 7Bibevski S , Mendoza L, Ruzmetov M, et al Custodiol cardioplegia solution compared to cold blood cardioplegia in pediatric cardiac surgery: a single-institution experience. Perfusion. 2020;35:316-322. 10.1177/026765911987800631581896 · doi ↗ · pubmed ↗
- 8Amaç B , Selçuk M, BölükbaşS, et al Use of del Nido cardioplegia in adult cardiac surgery. Eur Res J. 2022;8:139-144. 10.18621/eurj.1059285 · doi ↗