Non-invasive Ventilation in Adult Cancer Patients With Acute Respiratory Failure: A Systematic Review of Clinical Outcomes and Predictors of Failure
Mohamad Abu Zaher, Osman El Jundi, Hanan Arain

TL;DR
This review evaluates the effectiveness of non-invasive ventilation in cancer patients with acute respiratory failure, finding that benefits depend on the specific clinical context.
Contribution
The study provides a systematic review of NIV outcomes in cancer patients with ARF, identifying context-specific predictors and effectiveness in the high-flow nasal cannula era.
Findings
NIV showed no significant benefit over oxygen or HFNC in de novo hypoxemic respiratory failure.
NIV failure rates were high in cancer-related ARDS, with strong association to mortality.
Early NIV in cancer patients with cardiac dysfunction was linked to lower ICU mortality.
Abstract
Acute respiratory failure (ARF) is a leading cause of unexpected admissions to the ICU in adults with active solid or haematologic cancer. Early trials highlighted some benefits of non-invasive ventilation (NIV) delivered with supplemental oxygen versus conventional oxygen. Whether this is still maintained in the high-flow nasal cannula (HFNC) era is doubtful. Therefore, a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-guided, scenario-based systematic review was conducted to evaluate the effectiveness and harms of NIV versus oxygen/HFNC and to identify predictors and outcomes of NIV failure in adult cancer patients with ARF. Searches on PubMed from inception to 31 August 2025, Scopus, and the Cochrane Library from 2010 to 31 August 2025 were completed. In this review of trials and studies, primary outcomes were NIV failure, defined as intubation during the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
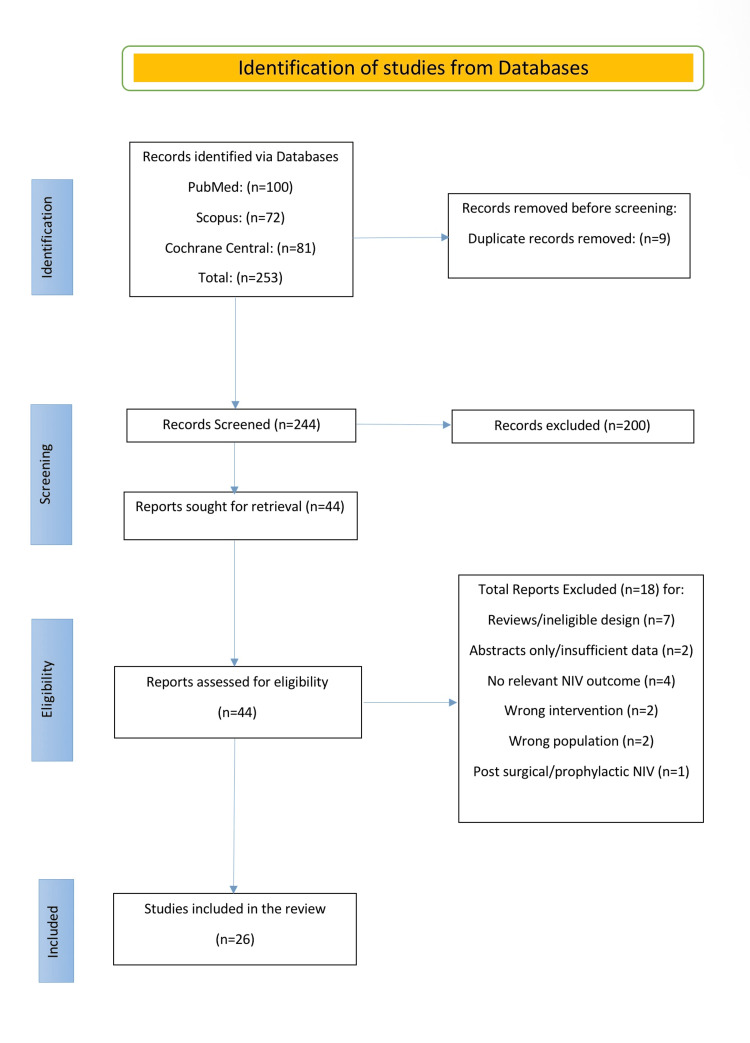 Figure 1
Figure 1| Study | Year | Country | Design | Setting | ARF phenotype | N (NIV) | Population (HM vs solid) | Contrast type | DNI included? | NIV approach (mode/interface; timing) |
| Liu et al. [ | 2017 | Canada | Retrospective cohort | ICU | ARDS | 79 | Haematologic | Single-arm NIV cohort | Included | First line; mask; median, 41 minutes after arrival to ITU |
| Bris et al. [ | 2024 | France | Retrospective cohort | ICU | ARDS | 1,373 | Mixed | Descriptive ARDS cohort (national; NIV subgroup) | Not specified | Non-invasive ventilation applied in 1,373 cancer patients. Within index ICU admission; exact timing not captured |
| Contejean et al. [ | 2016 | France and Belgium | Post hoc analysis of a prospective multicentre cohort | ICU | De novo hypoxemia | 205 | Haematologic | ARF aetiology, determined vs undetermined | Not specified | Started in 205/604 patients (33.9%) at (or within hours of) ICU admission |
| Azoulay et al. [ | 2017 | Multinational | Prospective cohort | ICU | De novo hypoxemia | 232 | Mixed | NIV vs HFNC | Not specified | Initiated in 232/915; at ICU admission (initial oxygenation strategy) |
| Hilbert et al. [ | 2001 | France | Randomised controlled trial | ICU | De novo hypoxemia | 26 | Mixed | NIV vs oxygen | Not specified | First line; face mask; within hours of ICU admission |
| Lemiale et al. [ | 2015 | France and Belgium | Randomised controlled trial | ICU | De novo hypoxemia | 191 | Mixed | NIV Vs oxygen/HFNC | Excluded | 191 patients randomised to immediate NIV as first-line support; ICU ventilator + face mask (majority), pressure-support mode; immediately post-randomisation |
| Lemiale et al. [ | 2015 | Multicentre | Post hoc analysis of a prospective, multicentre cohort | ICU | De novo hypoxemia | 142 | Haematologic | NIV vs HFNC | Included | Initiated in 142/380 ; at ICU admission (first-line ICU strategy, assessed over first 48 hours) |
| Mokart et al. [ | 2020 | Multinational | Prospective cohort | ICU | Ward/pre-ICU | 202 | Mixed | Neutropenia vs non-neutropenia | Not specified | Initiated in 202/1,481 patients; at ICU admission (initial oxygenation strategy) |
| Coudroy et al. [ | 2016 | France | Retrospective cohort | ICU | De novo hypoxemia | 55 | Mixed | NIV vs HFNC | Excluded | Initiated in 55/115 (first-line); at ICU admission/within 6 hours of ARF onset (median 1 hour from ICU admission) |
| Lima et al. [ | 2021 | Brazil | Retrospective cohort | ICU | De novo hypoxemia | 226 | Solid | Single-arm NIV cohort | Not specified | First line; mask |
| Rathi et al. [ | 2017 | United States | Retrospective cohort | ICU | De novo hypoxemia | 793 | Mixed | NIV vs IMV | Not specified | First-line support in 793/1,614 patients; face mask; at ICU admission |
| Belenguer-Muncharaz et al. [ | 2013 | Spain | Retrospective cohort | ICU/ward | ARDS | 35 | Haematologic | IMV vs NPPV | Not specified | Initiated in 35/41 (85%); first-line at ICU admission (CPAP sometimes used on ward pre-ICU) |
| Azoulay et al. [ | 2014 | Multinational | Multicentre cohort | ICU | ARDS | 387 | Mixed | Descriptive ARDS cohort | Not specified | Initiated in 387/1,004; at ICU admission (first-line ventilatory strategy) |
| Türkoğlu et al. [ | 2013 | Turkey | Semi-prospective cohort | Ward | ARDS | 46 | Haematologic | Descriptive ARDS cohort | Not specified | Initiated in 46/68; in ICU as first-line ARDS support with intubation on prespecified failure criteria |
| Grgić Medić et al. [ | 2015 | Croatia | Prospective cohort | ICU | De novo hypoxemia | 28 | Haematologic | Descriptive ICU cohort | Included | Initiated in 28/170 patients with ARF; face mask or helmet system; at presentation with ARF, before intubation criteria were met |
| Siddiqui et al. [ | 2021 | India | Prospective cohort | ICU | De novo hypoxemia | 41 | Haematologic | Descriptive ICU cohort | Excluded | Initiated in 41/101 patients; within 24 hours of ICU admission |
| Adda et al. [ | 2008 | France | Retrospective cohort | ICU | De novo hypoxemia | 99 | Haematologic | Single-arm NIV cohort | Excluded | Median 0 days (IQR: 0-1) from ICU admission |
| Ferreira et al. [ | 2015 | Brazil | Retrospective cohort | ICU | De novo hypoxemia | 114 | Mixed | Single-arm NIV cohort | Included | First line; oro-facial or total face mask; at ICU admission |
| Saillard et al. [ | 2020 | France | Retrospective cohort | ICU | Cardiac dysfunction | 63 | Mixed | NIV vs HFNC | Not specified | NIV used as initial ventilation strategy |
| Meert et al. [ | 2011 | Belgium | Retrospective cohort | ICU | De novo hypoxemia | 41 | Mixed | NIV vs IMV | Excluded | Initiated in 41/164 (25%); first-line trial in ICU prior to IMV |
| Squadrone et al. [ | 2010 | Italy | Randomised clinical trial | ICU/ward | Ward/pre-ICU | 10 | Haematologic | CPAP vs oxygen | Excluded | Initiated in 10/40; rescue NIV at ICU entry after ward CPAP/oxygen failure (ICU admission on prespecified criteria) |
| Wermke et al. [ | 2012 | Germany | Randomised controlled trial | Ward | Ward/pre-ICU | 42 | Haematologic | Intermittent NIV vs oxygen | Included | Early intermittent NIV delivered on the ward in arm B; full face mask; immediately after randomisation |
| Alptekinoglu Mendil et al. [ | 2021 | Turkey | Randomised controlled trial | Ward | De novo hypoxemia | 34 | Haematologic | Context only: no NIV arm | Not specified | Initiated in 34/100 patients; after ward treatment failure |
| Lemiale et al. [ | 2014 | France 16 medical | Multicentre post hoc cohort analysis of a previous RCT dataset | Ward | De novo hypoxemia | 81 | Mixed | NIV vs oxygen vs IMV; NIV success vs failure | Excluded | First-line face mask; at ICU admission |
| Barreto et al. [ | 2020 | Brazil | Prospective cohort | ICU | De novo hypoxemia | 59 | Haematologic | Single-arm NIV cohort | Not specified | Initiated in 59/82 patients as first-line support; facial or nasal mask; immediately at ICU admission (within first 24 hours) |
| Gristina et al. [ | 2011 | Italy | Retrospective analysis of a prospectively collected | ICU | De novo hypoxemia | 274 | Haematologic | NIV vs IMV | Not specified | Initiated in 274/1,302; at ICU admission (first-line; continuous for first 24 hours) |
| Study | Scenario | Outcome modelled | Model | Independent predictors (direction) | Adjusted effect (metric, 95% CI) | Key covariates |
| Azoulay et al. (2017) [ | De novo hypoxemia | NIV failure/need for intubation (during index ARF) | Cause-specific Cox (competing risk = death) | Higher SOFA (↑); PaO₂/FiO₂ < 300 (↑); | SOFA per point HR: 1.09 (1.06-1.13); PaO₂/FiO₂ < 300 HR: 1.47 (1.05-2.07); PJP HR: 2.11 (1.42-3.14); IPA HR: 1.85 (1.21-2.85); Undetermined aetiology HR: 1.46 (1.09-1.98); Age per year HR: 0.92 (0.86-0.99). | Age; day 1 SOFA; PaO₂/FiO₂ class; ARF aetiology; initial oxygenation strategy (HFNC/NIV). |
| Coudroy et al. (2016) [ | De novo hypoxemia | NIV failure/intubation (overall cohort) | Multivariable logistic regression | SAPS II (↑); Vasopressors within 24 hours (↑); NIV as first-line (↑). | SAPS II OR: 1.04 (1.00-1.08); Vasopressors OR: 4.12 (1.32-12.84); First-line NIV OR: 3.25 (1.39-7.60). | Age; PaO₂/FiO₂; immunosuppression type; vasopressors; cause of ARF; PaCO₂; year of ICU admission (forced). DNI excluded. |
| Adda et al. (2008) [ | De novo hypoxemia | NIV failure/need for intubation (index ARF) | Multivariable logistic regression | Respiratory rate under NIV (↑); Delay from ICU admission to first NIV (↑); Vasopressors (↑); Renal replacement therapy (↑); ARDS at time of NIV (↑). | RR under NIV OR: 1.18 per breath/min (1.05-1.33); Delay OR: 2.00 per day (1.02-3.94); Vasopressors OR: 6.50 (1.59-26.53); RRT OR: 18.31 (1.99-168.65); ARDS OR: 77.71 (6.88-878.38). | Variables with p < 0.10 entered; final model as above; Hosmer-Lemeshow p = 0.64. |
| Lemiale et al. (2014) [ | De novo hypoxemia | NIV failure/intubation (during ICU stay) | Multivariable logistic regression with random centre effect | Higher oxygen requirement at ICU admission (↑); More lung quadrants with infiltrates (↑); Haemodynamic dysfunction (↑). | Oxygen requirement OR: 1.11 per L/min (1.04-1.19); Lung quadrants OR: 1.56 per quadrant (1.20-2.02); Haemodynamic dysfunction OR: 2.25 (1.13-4.48). | Centre random effect; organ dysfunctions (LODS domains); infection; imaging extent; admission O₂ flow. |
| Barreto et al. (2020) [ | De novo hypoxemia | NIV failure/intubation (during index ARF) | Multivariable logistic regression | Higher SOFA (↑); Higher respiratory rate (↑); Sepsis on ICU admission (↑). | SOFA OR: 1.35 (1.12-2.10); Respiratory rate OR: 1.10 (1.00-1.22) per bpm; Sepsis OR: 16.9 (1.93-149.26). | Age; SOFA; respiratory rate; P/F ratio; lactate; vasopressors; infection status. |
| Gristina et al. (2011) [ | De novo hypoxemia | NIV failure/need for intubation (index ARF) | Multivariable logistic regression | Higher SAPS II (↑); ALI/ARDS at admission (↑). | SAPS II OR: 2.01 (1.01-4.03); ALI/ARDS OR: 2.27 (1.35-3.82). | Variables with p < 0.1 entered; final model retained SAPS II and ALI/ARDS (good fit: LR, p = 0.0012; HL, p = 0.76; no collinearity). |
| Scenario | Studies (n) | Patients on NIV (approx) | Median NIV failure % (IQR) | Median in-hospital mortality % (IQR) | Signal vs oxygen/HFNC | Notes |
| De novo hypoxemia | 17 | 6,915 | 42.6% (38.0-52.8) | 45.6% (42.2-54.5) | Neutral/harm vs HFNC | Largest RCT neutral; adjusted cohorts neutral/harm; use stop rules |
| Cardiac dysfunction | 1 | 127 | — | 57.0% (57.0-57.0) | Favourable for NIV | Adjusted lower ICU mortality with initial NIV |
| ARDS | 5 | 1,509 | 78.1% (62.0-84.0) | 66.8% (59.5-72.1) | Harm (failure common) | Failure ≈60%-80%; early intubation if no rapid improvement |
| Ward/pre-ICU | 3 | 226 | 60.0% (42.5-77.5) | 15.0% (15.0-15.0) | Possible benefit (helmet CPAP) | Small single-centre, largely pre-HFNC; neutropenic/post-HSCT |
| NOS studies | NOS domain ratings | Overall summary | ||||
| Study details | Selection | Comparability | Outcome | Total | ROB | Justification |
| Liu et al., 2017 [ | *** | * | ** | 6/9 Stars | Moderate | Single-centre retrospective cohort. Clinician-set intubation thresholds. Incomplete adjustment for shock and oxygenation leaves confounding by indication. |
| Bris et al., 2024 [ | **** | ** | ** | 8/9 Stars | Low | Large national cohort with mixed-effects adjustment. Limitations: coding-defined ARDS and no out-of-hospital death capture. |
| Contejean et al., 2016 [ | **** | ** | *** | 9/9 Stars | Low | Large prospective multicentre HM ICU ARF cohort with blinded aetiology adjudication and comprehensive adjustment. Hospital mortality objectively ascertained. |
| Azoulay et al., 2017 [ | **** | ** | *** | 9/9 Stars | Low | Prospective multinational cohort with excellent selection, strong adjustment including PS matching, and objective outcome ascertainment. |
| Lemiale et al., 2015 [ | **** | ** | *** | 9/9 Stars | Low | Prospective multicentre cohort with excellent selection, strong propensity/IPW adjustment and objective outcomes, well suited to compare initial NIV vs oxygen. |
| Mokart et al., 2020 [ | **** | ** | *** | 9/9 Stars | Low | Prospective multicentre cohort with excellent selection, strong confounding control using mixed models and propensity matching, and objective hospital mortality ascertainment. |
| Coudroy et al., 2016 [ | *** | ** | *** | 8/9 Stars | Low | Single-centre retrospective ICU cohort with objective outcomes and reasonable adjustment for severity, oxygenation and vasopressors, limiting generalisability. |
| Lima et al., 2021 [ | *** | ** | *** | 8/9 Stars | Low | Well-defined solid-tumour NIV cohort with robust adjustment for shock, oxygenation, and metabolic severity; objective outcomes minimize measurement bias despite single-centre, retrospective design. Well-defined solid-tumour NIV cohort with robust adjustment for shock, oxygenation, and metabolic severity; objective outcomes minimize measurement bias despite single-centre, retrospective design. |
| Rathi et al., 2017 [ | *** | ** | *** | 8/9 Stars | Low | Large consecutive single-centre ICU cohort with objective outcomes and robust severity adjustment. Some residual confounding by indication and aetiology remains. |
| Belenguer-Muncharaz et al., 2013 [ | *** | * | *** | 7/9 Stars | Moderate | Solid outcome ascertainment in a well-defined cohort, but between-group confounding for NIV vs IMV is unadjusted and the single-centre retrospective design limits generalisability. |
| Azoulay et al., 2014 [ | **** | ** | *** | 9/9 Stars | Low | Rigorous multicentre cancer-ARDS cohort using Berlin criteria with strong multivariable control, including ventilation strategy and invasive fungal infection, and objective mortality ascertainment. |
| Türkoğlu et al., 2013 [ | *** | * | *** | 7/9 Stars | Moderate | Clear single-centre HM-ARDS cohort with objective outcomes, but limited adjustment leaves residual confounding despite multivariable analysis. |
| Grgić Medić et al., 2015 [ | *** | ** | *** | 8/9 Stars | Low | Prospective single-centre HM ICU cohort with objective outcomes and robust adjustment for severity and organ failure. Limitations include single centre design and residual confounding. |
| Siddiqui et al., 2021 [ | *** | ** | *** | 8/9 Stars | Low | Prospective consecutive single-centre HLM cohort with objective outcomes and adjustment for severity and organ support. Generalisability limited by single centre. |
| Adda et al., 2008 [ | *** | * | ** | 6/9 Stars | Moderate | Single-centre retrospective cohort with objective outcomes. Limited adjustment for baseline severity and oxygenation leaves confounding by indication. |
| Ferreira et al., 2015 [ | *** | ** | *** | 8/9 Stars | Low | Consecutive ICU NIV cohort with objective outcomes and reasonable adjustment for severity and aetiology. Single-centre design and residual confounding remain limitations. |
| Saillard et al., 2020 [ | *** | ** | *** | 8/9 Stars | Low | Well-defined cohort with robust adjustment (severity, organ failure, aetiology) and propensity matching. Objective outcomes minimise measurement bias despite single-centre design. |
| Meert et al., 2011 [ | *** | * | *** | 7/9 Stars | Moderate | Clear single-centre IMV cohort with objective outcomes. Modest adjustment without key severity or oxygenation covariates leaves confounding by indication. |
| Alptekinoğlu Mendil et al., 2021 [ | *** | ** | *** | 8/9 Stars | Low | Open label ward RCT. Concealment plausible but sequence details sparse. Minor post-randomisation exclusions. Objective outcomes limit measurement bias. |
| Lemiale et al., 2014 [ | *** | ** | *** | 8/9 Stars | Low | Prospective multicentre ICU cohort with prespecified intubation criteria and robust multivariable modelling, including centre effects. Excluding baseline DNI introduces minor selection bias. |
| Barreto et al., 2020 [ | *** | ** | *** | 8/9 Stars | Low | Prospective protocolised single-centre cohort with objective outcomes and solid adjustment, limited by single-centre design. |
| Gristina et al., 2011 [ | **** | ** | *** | 9/9 Stars | Low | Exemplary multicentre cohort with rigorous selection and strong propensity-adjusted comparability, using objective outcomes. Well suited to inform initial NIV versus IMV strategies in HM ARF. |
| Study details | ROB 2 domains | Overall risk of bias | |||||
| Study | Randomisation process | Deviations from intended interventions | Missing outcome data | Measurement of outcomes | Selection of the reported result | Judgment | Reasons |
| Hilbert et al., 2001 [ | Some concerns | Some concerns | Low risk | Low risk | Some concerns | Some concerns | Small, single-centre, open-label trial with limited sequence details, objective outcomes, and predefined intubation criteria mitigate. |
| Lemiale et al., 2015 [ | Low risk | Some concerns | Low risk | Low risk | Low risk | Some concerns | Robust randomisation and prespecified SAP, but open-label design with allowable co-interventions (notably HFNC imbalance) introduces potential performance bias. |
| Squadrone et al., 2010 [ | Low risk | Some concerns | Low risk | Low risk | Some concerns | Some concerns | Strong randomisation and objective outcomes, but open-label delivery with potential co-intervention/monitoring differences and lack of a public protocol introduce performance/reporting concerns. |
| Wermke et al., 2012 [ | Some concerns | High Risk | Low risk | Low risk | Some concerns | High risk | The mandated cross-over and open-label design introduce substantial performance/deviation bias despite objective outcome measurement and low missing data. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory Support and Mechanisms · Nosocomial Infections in ICU · Tracheal and airway disorders
Introduction and background
Acute respiratory failure is a prime reason for unplanned ICU admission in adults with active solid tumours or haematologic malignancies. In these cases, short-term mortality is high, and it is even higher when acute respiratory distress syndrome is present [1,2]. In immunocompromised patients with hypoxemic respiratory failure, especially when the cause is uncertain or an opportunistic infection is suspected, both intubation and death remain prevalent [3,4]. Non-invasive ventilation (NIV) delivered as non-invasive positive pressure ventilation with supplemental oxygen via mask is attractive because it can improve oxygenation and reduce the work of breathing, while avoiding some of the harms of invasive ventilation. Early single-centre studies in immunosuppressed patients, including the trial by Hilbert and colleagues, reported lower intubation and mortality rates with early NIV compared to conventional oxygen. This finding helped drive the acceptance of NIV in oncology critical care [5].
Today the care outlook is different. High-flow nasal cannula oxygen therapy is extensively accessible, and supportive care pathways are better standardised. This progress sheds a shadow of uncertainty on the added value of NIV. This is most significant in de novo hypoxemic respiratory failure, that is not due to chronic obstructive pulmonary disease (COPD) exacerbation or acute cardiogenic pulmonary oedema [6,7]. Clinicians need to know which presentations and settings benefit the most from NIV, which are better treated by high-flow nasal cannula, and when persistent application of NIV may delay necessary intubations.
A scenario-based systematic review of adults with cancer and acute respiratory failure was performed for the purpose of this study. We examined five questions: first, the effectiveness of NIV versus oxygen or high-flow nasal cannula in de novo hypoxaemia; second, failure rates and outcomes in established acute respiratory distress syndrome; third, risk factors of NIV failure; fourth, prognosis after NIV failure; and fifth, ward or pre-ICU use of NIV in selected haematology populations with, or at high risk of, acute respiratory failure.
Review
Methods
Study Design and Framework
This systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines under a pre-specified protocol registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD420251102556). The aim was to evaluate the effectiveness and harms of non-invasive ventilation in adults with active cancer and acute respiratory failure, and to identify predictors of NIV failure.
Population, Intervention, Comparator, Outcome (PICO)
Population: Adults aged 18 years or older with active solid or haematologic malignancy and acute respiratory failure in hospital, ICU, haematology, or haematopoietic stem cell transplantation wards.
Intervention: NIV delivered as continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP) via mask or helmet.
Comparators: Conventional oxygen, high-flow nasal cannula, invasive mechanical ventilation, or none.
Outcomes: Intubation or NIV failure, mortality with in-hospital as the primary time point, ICU or time-bound mortality when available, length of stay, complications, and predictors of NIV failure.
Search Strategy
We searched PubMed from inception to 31 August 2025 (no date limits) and Scopus and Cochrane CENTRAL from 2010 to 31 August 2025. Pre-2010 studies were therefore eligible if identified via PubMed. Searches were limited to English. Concepts combined cancer or neoplasms, acute respiratory failure or ARDS, and non-invasive ventilation including CPAP and BiPAP. Reference lists of included studies and relevant reviews were screened. Full database-specific search strings for PubMed, Scopus, and Cochrane CENTRAL are provided in Appendix 1 (Appendix 1a-1c).
Eligibility Criteria
Inclusion: Human studies in English that were randomised trials, cohort studies, or case series with at least five cancer patients treated with NIV for acute respiratory failure, and that reported at least one prespecified outcome.
Exclusion: Paediatric populations, animal studies, case reports, reviews or editorials, studies without outcome data, studies focused only on invasive ventilation, and prophylactic postoperative or post-extubation NIV when acute respiratory failure was not present. Postoperative acute respiratory failure treated with NIV was eligible when the study explicitly defined acute respiratory failure.
Study Selection and Data Extraction
Two reviewers independently screened titles and abstracts and then full texts. Disagreements were resolved by discussion. Data was extracted with a piloted form into a prespecified spreadsheet. We recorded study characteristics, setting, design, sample size, cancer type and status, immunosuppression where reported, acute respiratory failure phenotype and aetiology, details of the intervention and comparator, and outcomes including intubation or NIV failure, mortality, length of stay, and complications. Do-not-intubate status was extracted where available. For predictors we extracted variables entered in multivariable models, adjusted effect sizes with 95% confidence intervals, model type, and covariates.
Risk of Bias Assessment
Two reviewers assessed risk of bias by design using Cochrane Risk of Bias 2 (RoB 2) [8] for randomised trials, and the Newcastle-Ottawa Scale [9]. Discrepancies were resolved by common consent.
Data Synthesis and Analysis
We performed a narrative qualitative synthesis only. We prespecified no meta-analysis because of heterogeneity in populations, acute respiratory failure definitions, NIV strategies and interfaces, and outcome time points. Where scenario-level summaries were presented (e.g., median NIV failure and mortality), these were calculated as simple medians with interquartile ranges across contributing studies. Results are organised by scenario: de novo hypoxaemia, acute respiratory distress syndrome (ARDS), ward or pre-ICU use, and outcomes after NIV failure. For predictors, we reported adjusted associations, noted how consistent they were across studies, and mentioned any thresholds that were reported. Univariate results were treated as hypothesis-generating.
Results
Study Selection and Characteristics
Twenty-six studies (four randomised controlled trials (RCTs), 22 cohorts) were included. The PRISMA flow chart is shown in Figure 1. Across studies, around 12,000 adult cancer patients with acute respiratory failure (ARF) received non-invasive ventilation (NIV). Populations were predominantly suffering from haematologic malignancies (acute leukaemia, lymphoma, myeloma), with additional solid-tumour cohorts. ARF aetiologies were most often infection (bacterial/fungal pneumonia, sepsis), followed by pulmonary oedema, tumour infiltration, or undetermined cause. NIV was commonly used as first-line ICU support via oronasal mask in pressure-support mode and in all included studies it was delivered with supplemental oxygen. Unless declared, “NIV failure” indicates intubation during the index ARF episode and mortality refers to in-hospital mortality. Per-study characteristics and outcomes are shown in Table 1.
PRISMA 2020 study selection for NIV in cancer-related acute respiratory failureRecords were identified from PubMed (n = 100), Scopus (n = 72), and Cochrane CENTRAL (n = 81), yielding 253 records. After removal of nine duplicate records, 244 records were screened by title and abstract, and 200 were excluded. Forty-four reports were sought and assessed for eligibility; 18 were excluded with the following reasons: reviews/ineligible design (n = 7), abstracts only/insufficient data (n = 2), no relevant NIV outcome (n = 4), wrong intervention (n = 2), wrong population (n = 2), and post-surgical/prophylactic NIV (n = 1). Twenty-six studies were included in the qualitative synthesis. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses, NIV = non-invasive ventilation.
Early NIV vs Oxygen or HFNC in de novo Hypoxemic ARF
Pre-HFNC single-centre RCT (Hilbert et al., 2001; n = 52) showed lower intubation (46% vs 77%) and hospital mortality (50% vs 81%) with NIV [5]. In contrast, the largest contemporary RCT (Lemiale et al., 2015; n = 374) showed no reduction in intubation (38% vs 45%) or 28-day mortality (24% vs 27%) with early NIV vs oxygen/HFNC [6]. Large, adjusted cohorts (Efraim 2017, Mokart et al. 2020) found no benefit of initial NIV [4,10], while Coudroy et al. (2016) reported higher adjusted odds of intubation (aOR ≈3.25) and 28-day mortality (aOR ≈3.70) with NIV vs HFNC [11]. Across studies, NIV failure was ~30%-55% and was associated with poor survival [12-14].
Summary: In de novo hypoxemic ARF, early NIV did not improve intubation or survival vs oxygen or HFNC, signals of harm appear when NIV is prolonged without predefined stop rules. An exception may be ARF with cardiac dysfunction [4,6,10,11].
NIV in Established Cancer-Related ARDS
NIV failure was frequent and portended worse outcomes. In Azoulay et al. (2014) (n ≈1,000), NIV attempted in 39% with 71% failure (mild 63%, moderate 69%, severe 79%), failure independently predicted higher in-hospital mortality [15]. A nationwide cohort (Bris et al, 2024) confirmed high mortality in haematological malignancy-associated acute respiratory distress syndrome (HM-ARDS), driven by shock, invasive fungal infection, and malignancy type rather than ventilatory mode [2]. Smaller cohorts were concordant in Türkoğlu et al. (2013; failure 78%) [16], Belenguer-Muncharaz et al. (2013; failure 40%, mortality ~70% in failures vs <30% in successes) [14], Grgić Medić et al. (2015; failure 61%) [17], Lima et al. (2021; failure 52%, mortality ~70% vs ~20%) [12], and Siddiqui et al. (2021; failure 53%) [18].
Summary: In cancer-related ARDS, NIV failure is common (~60%-80%) and strongly predicts death; use time-limited NIV with predefined stop rules and intubate early if no prompt improvement.
Independent Predictors of NIV Failure and Mortality
Across multivariable analyses, reproducible independent predictors of NIV failure included higher illness severity (Simplified Acute Physiology Score II (SAPS II)/Sequential Organ Failure Assessment (SOFA)), shock/vasopressors, and more severe hypoxemia (lower arterial oxygen partial pressure to inspired oxygen fraction ratio (PaO₂/FiO₂)) [3,15,17,19,20]. Undetermined ARF aetiology and invasive fungal infection were consistently linked to higher failure and/or mortality [2,3,12,21]. In ARDS cohorts, NIV failure itself independently predicted death; delayed intubation and nosocomial infection further worsened outcomes [2,12,15]. In ARF with cardiac dysfunction, initial NIV was associated with lower adjusted ICU mortality vs oxygen/HFNC only [21]. Study-level predictors and adjustment sets appear in Table 2.
Prognosis After NIV Failure
Across cohorts, invasive mechanical ventilation after NIV failure carried very poor outcomes. Meert et al. (2011) (n = 164) found prior NIV before invasive mechanical ventilation (IMV) was independently associated with lower odds of survival to discharge (aOR ≈0.30) [22]. Rathi et al. (2017) (n = 1,614) reported an ICU mortality of 71%/in-hospital mortality of 80% after NIV failure vs 28%/47% with NIV success [13]. Similar patterns occurred in Lima et al. (2021) and Belenguer-Muncharaz et al. (2013) [12,14].
Summary: NIV failure is a strong negative prognostic marker (mortality often >70%); close monitoring and timely intubation are critical.
Ward/Pre-ICU Preventive Use
Two small single-centre ward RCTs in neutropenic/post-haematopoietic stem cell transplant (HSCT) units evaluated early non-invasive support. Squadrone et al. (2010) (helmet CPAP vs oxygen; n = 40) reported reduced ICU admission, intubation, and in-hospital mortality [23]. Wermke et al. (2012) (intermittent NIV + oxygen vs oxygen; n = 86) showed non-significant trends toward benefit [24].
Summary: Ward-based CPAP/NIV may avert deterioration in selected haematology patients, but evidence is limited (small, single-centre; largely pre-HFNC).
Summary of Results
Table 3 summarises the outcomes for scenarios 1, 2, and 5.
Risk of Bias Within Studies
The four RCTs were open-label: two were small, single-centre ward trials, yielding “some concerns” for deviations from intended interventions. Most cohorts were at moderate risk of bias on the Newcastle-Ottawa Scale [9] due to confounding/selection. Risk of bias for observational studies is summarised in Table 4. Most cohorts were moderate risk due to residual confounding/selection, with a smaller subset at high risk (non-consecutive inclusion and/or substantial do-not-intubate (DNI) proportions). A minority achieved low-risk ratings with robust adjustment and complete follow-up.
Risk of bias for randomised trials is presented in Table 5. Most trials had some concerns, primarily for deviations from intended interventions in open-label designs, while randomisation, outcome measurement, and missing data were generally low risk.
Discussion
Modern evidence does not support routine NIV for every cancer-related ARF. The early single-centre RCT signal [5] has not been replicated in the HFNC era. Contemporary trials and adjusted cohorts show no dependable benefit of NIV over oxygen or HFNC in de novo hypoxemia and may suggest harm when NIV is prolonged in non-responders or used without clear stop rules [4,6,10,11]. In cancer-related ARDS, NIV fails in about 60%-80% of cases and failure strongly predicts death. High-risk features include shock, low PaO₂/FiO₂, invasive fungal infection, higher severity scores, and an undetermined cause of ARF [2,3,12,15,21]. Two ward trials suggested a niche for early helmet CPAP/NIV in selected neutropenic or post-HSCT patients [23,24]. Across settings, NIV failure persistently signals exceedingly higher rates of mortality [12-14,22,25-27].
In short, our findings do not argue against NIV as a modality, but against indiscriminate or prolonged NIV in high-risk de novo hypoxemic ARF. The NIV that looked helpful before HFNC and standardised pathways is now often found to be neutral and may be associated with worse outcomes when NIV delays needed intubation. Where HFNC is limited or unavailable, a brief, protocol driven NIV trial can be reasonable if strict stop rules and rapid access to intubation are applied.
Limitations
No meta-analysis was performed, as the studies were too heterogeneous. The certainty of our results is limited by the mainly observational designs, confounding by indication, variable handling of do-not-intubate (DNI) orders, and differences in NIV protocols, interfaces, and intubation thresholds. Some large cohorts may overlap, so the pooled number of patients is approximate. The included studies were also limited to the English language, so publication and language bias are possible. These issues were reduced by implementing a focus on adjusted analyses and a scenario-based qualitative synthesis; however, they cannot be fully eliminated.
Practice Signals
In de novo hypoxemia, HFNC is preferred. If NIV is trialled, set strict stop rules and reassess at 60-90 minutes. Intubate early if no response [6,11]. In ARDS, do not persist with NIV without rapid improvement. Intubate early [2,15]. In ARF with cardiac dysfunction, NIV may be favourable [21]. For ward treatment (neutropenic/post-HSCT), consider CPAP/NIV only with trained staff, continuous monitoring, and fast ICU access [10,24,25,28].
Pragmatic Stop Rules (60-90 Minutes)
Target peripheral capillary oxygen saturation (SpO₂) ≥92%, respiratory rate ↓ ≥20%, PaO₂/FiO₂ ↑ ≥20%, and no rising work of breathing or new haemodynamic or neurological instability. If targets are not met, or the patient deteriorates, intubate. Do not escalate NIV further.
Harms and Complications
Device complications were uncommon, but delayed intubation after NIV failure was linked to more nosocomial infection and higher mortality. It is advisable to avoid prolonged NIV in non-responders.
Research Priorities
There is a need for further stratified RCTs of HFNC vs NIV (helmet vs mask) with protocolised stop rules and oncology-specific subgroup, ward implementation trials focused on staffing, monitoring, and escalation, and standardised reporting of intubation criteria, DNI status, and ARF aetiology.
Conclusions
In adults with cancer and ARF, NIV’s benefit is scenario dependent. For de novo hypoxemia, NIV offers no clear advantage over oxygen/HFNC and may be harmful if prolonged in non-responders. In ARDS, NIV often fails and failure strongly predicts mortality. A targeted use of NIV remains beneficial for cardiac dysfunction and selected ward populations. When NIV is attempted, tight monitoring and early intubation for non-responders are essential to avoid harm.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Noninvasive ventilation in patients with hematologic malignancy: a retrospective study J Intensive Care Med Liu J Bell C Campbell V De Backer J Tamberg E Lee C Mehta S 88506661769072534201710.1177/088506661769072528142306 · doi ↗ · pubmed ↗
- 2Acute respiratory distress syndrome in patients with hematological malignancies: a one-year retrospective nationwide cohort study Ann Intensive Care Bris PN Pauly V Orleans V 1411420243925934510.1186/s 13613-024-01373-4PMC 11390989 · doi ↗ · pubmed ↗
- 3Increased mortality in hematological malignancy patients with acute respiratory failure from undetermined etiology: a Groupe de Recherche en Réanimation Respiratoire en Onco-Hématologique (Grrr-OH) study Ann Intensive Care Contejean A Lemiale V Resche-Rigon M 102620162778338110.1186/s 13613-016-0202-0PMC 5080277 · doi ↗ · pubmed ↗
- 4Acute hypoxemic respiratory failure in immunocompromised patients: the Efraim multinational prospective cohort study Intensive Care Med Azoulay E Pickkers P Soares M 180818194320172894836910.1007/s 00134-017-4947-1 · doi ↗ · pubmed ↗
- 5Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure N Engl J Med Hilbert G Gruson D Vargas F 48148734420011117218910.1056/NEJM 200102153440703 · doi ↗ · pubmed ↗
- 6Effect of noninvasive ventilation vs oxygen therapy on mortality among immunocompromised patients with acute respiratory failure: a randomized clinical trial JAMA Lemiale V Mokart D Resche-Rigon M 1711171931420152644487910.1001/jama.2015.12402 · doi ↗ · pubmed ↗
- 7Acute respiratory failure in patients with hematological malignancies: outcomes according to initial ventilation strategy: a groupe de recherche respiratoire en réanimation onco-hématologique (Grrr-OH) study Ann Intensive Care Lemiale V Resche-Rigon M Mokart D 28520152642935510.1186/s 13613-015-0070-z PMC 4883632 · doi ↗ · pubmed ↗
- 8Ro B 2: a revised tool for assessing risk of bias in randomised trials BMJ Sterne JA SavovićJ Page MJ 0366201910.1136/bmj.l 489831462531 · doi ↗ · pubmed ↗