Impact of a Reproductive Health Survivorship Care Plan on Fertility, Pregnancy Concerns, and Accessing Reproductive Healthcare Among Young Nulliparous Breast Cancer Survivors
Ksenya Shliakhtsitsava, Shaylyn S. Stark, Tanushree Prasad, Sarah Boles, Diana Chingos, Jennifer Ehren, Jessica R. Gorman, Sally A. D. Romero, Jun J. Mao, Paul Nathan, Saro H. Armenian, H. Irene Su

TL;DR
A web-based care plan improved reproductive health concerns and specialist access for young breast cancer survivors who haven't had children.
Contribution
A web-based survivorship care plan was shown to effectively address unmet reproductive health needs in young nulliparous breast cancer survivors.
Findings
35.3% of intervention participants improved fertility and pregnancy concerns versus 10.0% in the control group.
Intervention participants were more likely to access fertility specialists (37.5% vs. 6.7%).
Abstract
Young patients with breast cancer frequently receive chemotherapy and/or endocrine therapy that adversely affect ovarian function, leading to fertility, pregnancy, and other reproductive health concerns. Despite available evidence‐based management strategies, dissemination to survivors and healthcare providers remains limited, resulting in substantial unmet informational and care needs. Web‐based survivorship care plans may offer an effective approach to address these gaps. To evaluate the effect of a web‐based Reproductive Health Survivorship Care Plan (SCP‐R) on reproductive concerns and reproductive healthcare access among nulliparous young breast cancer survivors (YBCS). This is a secondary analysis of a 24‐week randomized controlled trial on the effectiveness of a web‐based SCP‐R addressing unmet informational and clinical management needs for breast cancer survivors aged 18–50…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
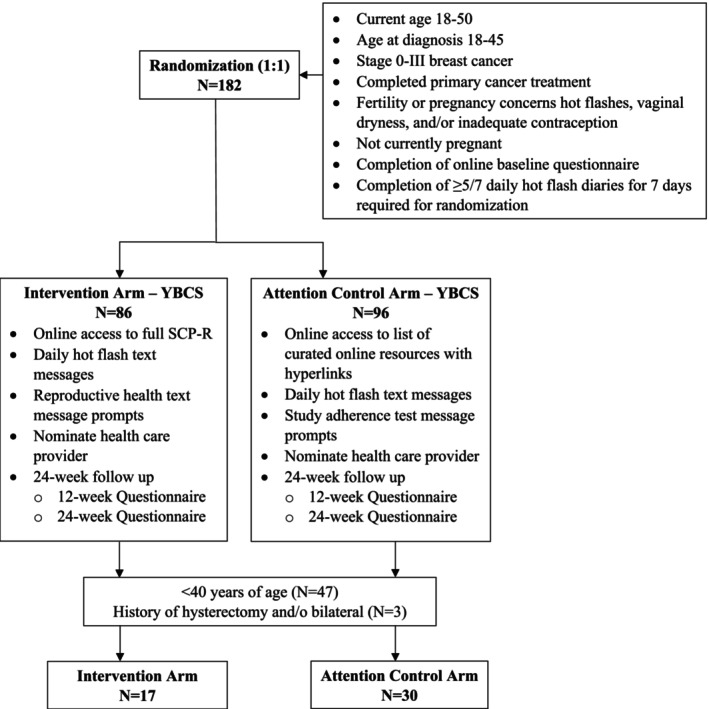 FIGURE 1
FIGURE 1| Characteristic | Overall | Intervention | Control |
|
|---|---|---|---|---|
|
|
|
| ||
|
|
|
| ||
| Age at enrollment (years), mean [SD] | 34 ± 3.8 | 34.3 ± 3.2 | 33.8 ± 4.1 | |
| 25–35 | 34 (72.3) | 13 (76.5) | 21 (70.0) | 0.76 |
| 36–40 | 13 (27.7) | 4 (23.5) | 9 (30.0) | 0.74 |
| Race | ||||
| White | 39 (83.0) | 16 (94.1) | 23 (76.7) | 0.29 |
| Black or African American | 1 (2.1) | 0 (0.0) | 1 (3.3) | |
| Other | 7 (14.9) | 1 (5.9) | 6 (20.0) | |
| Hispanic ethnicity | 2 (4.3) | 0 (0.0) | 2 (6.7) | 0.53 |
| Partnered relationship status | 31 (66.0) | 10 (58.8) | 21 (70.0) | 0.44 |
| College graduate | 44 (93.6) | 17 (100.0) | 27 (90.0) | 0.29 |
| Income | ||||
| < $51 000 | 12 (26.1) | 4 (23.5) | 8 (27.6) | 1.00 |
| ≥ $51 000 | 34 (73.9) | 13 (76.5) | 21 (72.4) | |
| Current smoker | 2 (4.3) | 1 (5.9) | 1 (3.3) | 1.00 |
| BMI | ||||
| < 18.5 | 3 (6.4) | 1 (5.9) | 2 (6.7) | 0.15 |
| 18.5 to < 25 | 20 (42.6) | 5 (29.4) | 15 (50.0) | |
| 25 to < 30 | 15 (31.9) | 9 (52.9) | 6 (20.0) | |
| ≥ 30 | 9 (19.2) | 2 (11.8) | 7 (23.3) | |
| Mean age at breast cancer diagnosis [SD] | 30.7 ± 3.5 | 30.5 ± 3.2 | 30.7 ± 3.8 | 0.92 |
| Age at diagnosis | ||||
| 18–24 | 3 (6.4) | 1 (5.9) | 2 (6.7) | 1.00 |
| 25–35 | 40 (85.1) | 15 (88.2) | 25 (83.3) | |
| 36–45 | 4 (8.5) | 1 (5.9) | 3 (10.0) | |
| Years since diagnosis | ||||
| < 1 | 7 (14.9) | 2 (11.8) | 5 (16.7) | 0.30 |
| 1–2 | 16 (34.0) | 7 (41.2) | 9 (30.0) | |
| 3–5 | 15 (31.9) | 3 (17.7) | 12 (40.0) | |
| > 5 | 9 (19.2) | 5 (29.4) | 4 (13.3) | |
| Cancer treatment | ||||
| Surgery | 47 (100.0) | 17 (100.0) | 30 (100.0) | 1.0 |
| Radiation | 31 (66.0) | 10 (58.8) | 21 (70.0) | 0.44 |
| Chemotherapy | 42 (89.4) | 16 (94.1) | 26 (86.7) | 0.64 |
| Biologic therapy | 14 (29.8) | 7 (41.2) | 7 (23.3) | 0.19 |
| Hormonal treatment | 37 (78.7) | 10 (58.8) | 27 (90.0) |
|
| Current GnRH agonist | 9 (19.2) | 3 (17.7) | 6 (20.0) | 1.00 |
| Cancer stage | ||||
| 1 | 14 (30.4) | 3 (18.7) | 11 (36.7) | 0.15 |
| 2 | 22 (47.8) | 11 (68.8) | 11 (36.7) | |
| 3 | 10 (21.7) | 2 (12.5) | 8 (26.6) | |
| Comorbidities | ||||
| Hypertension | 3 (6.4) | 1 (5.9) | 2 (6.7) | 1.00 |
| Diabetes | 0 (0.0) | 0 (0.0) | 0 (0.0) | — |
| Mental illness | 14 (29.8) | 3 (17.7) | 11 (36.7) | 0.17 |
| Osteopenia or osteoporosis | 4 (8.5) | 2 (11.8) | 2 (6.7) | 0.61 |
| Menstruation frequency over the past year | ||||
| 0 | 14 (29.8) | 5 (29.4) | 9 (30.0) | 0.39 |
| 1–3 | 11 (23.4) | 4 (23.5) | 7 (23.3) | |
| 4–9 | 8 (17.0) | 1 (5.9) | 7 (23.3) | |
| 10–12 | 14 (29.8) | 7 (23.3) | 7 (23.3) | |
| Desires another baby in the future | ||||
| No or probably no | 9 (19.1) | 4 (23.5) | 5 (16.7) | 0.71 |
| Yes or probably yes | 38 (80.9) | 13 (76.5) | 25 (83.3) | |
| When will start trying to have a child? | ||||
| Not planning | 9 (20.0) | 3 (17.7) | 6 (21.4) | 0.92 |
| Attempting now | 4 (8.9) | 2 (11.8) | 2 (7.1) | |
| < 2 years | 17 (37.8) | 7 (41.2) | 10 (35.7) | |
| > 2 years | 15 (33.3) | 5 (29.4) | 10 (35.7) | |
| Trying to become pregnant now | ||||
| Yes | 4 (8.5) | 2 (11.8) | 2 (6.7) | 0.89 |
| No | 32 (68.1) | 11 (64.7) | 21 (70.0) | |
| Neither trying nor avoiding | 11 (23.4) | 4 (23.5) | 7 (23.3) | |
| Healthcare provider talked with me about trying to become pregnant | ||||
| Never | 7 (14.9) | 4 (23.5) | 3 (10.0) | 0.24 |
| At least once | 40 (85.1) | 13 (76.5) | 27 (90.0) | |
| Healthcare provider advice on pregnancy | ||||
| Avoid | 4 (10.0) | 0 (0.0) | 4 (14.8) | 0.35 |
| Attempt now | 2 (5.0) | 0 (0.0) | 2 (7.4) | |
| Attempt later | 30 (75.0) | 11 (84.6) | 19 (70.4) | |
| Conflicting advice | 4 (10.0) | 2 (15.4) | 2 (7.4) | |
| Healthcare provider advice on timing | ||||
| No rec | 4 (10.0) | 1 (7.7) | 3 (11.1) | 0.71 |
| < 1 year to < 2 years | 6 (15.0) | 3 (23.1) | 3 (11.1) | |
| 2–4 years | 9 (22.5) | 2 (15.4) | 7 (25.9) | |
| 5–10 years | 19 (47.5) | 7 (53.9) | 12 (44.4) | |
| > 10 years | 2 (5.0) | 0 (0.0) | 2 (7.4) | |
| Infertility before cancer | 1 (2.1) | 0 (0.0) | 1 (3.3) | 1.00 |
| Fertility specialist | ||||
| No | 14 (29.8) | 6 (35.3) | 8 (26.7) | 0.53 |
| Before cancer | 3 (6.4) | 1 (5.9) | 2 (6.7) | 1.00 |
| After cancer before treatment | 28 (59.6) | 9 (52.9) | 19 (63.3) | 0.49 |
| During treatment | 3 (6.4) | 0 (0.0) | 3 (10.0) | 0.29 |
| After completing treatment | 6 (12.8) | 2 (11.8) | 4 (13.3) | 1.00 |
| Fertility concerns subscale | ||||
| Mean [SD] | 3.9 ± 1.0 | 4.1 ± 0.7 | 3.8 ± 1.1 | |
| Mild (≤ 3) | 13 (27.7) | 2 (11.8) | 11 (36.7) | 0.58 |
| Moderate/severe (> 3) | 34 (72.3) | 15 (88.2) | 19 (63.3) | 0.09 |
| Pregnancy concerns subscale | ||||
| Mean [SD] | 3.2 ± 0.9 | 3.3 ± 0.6 | 3.2 ± 1.0 | |
| Mild (≤ 3) | 24 (51.1) | 7 (41.2) | 17 (56.7) | 0.52 |
| Moderate/severe (> 3) | 23 (48.9) | 10 (58.8) | 13 (43.3) | 0.31 |
| Personal health subscale | ||||
| Mean [SD] | 3.3 ± 0.9 | 3.2 ± 0.9 | 3.3 ± 0.9 | |
| Mild (≤ 3) | 18 (38.3) | 7 (41.2) | 11 (36.7) | 0.54 |
| Moderate/severe (> 3) | 29 (61.7) | 10 (58.8) | 19 (63.3) | 0.76 |
| Child health subscale | ||||
| Mean [SD] | 3.8 ± 0.8 | 3.8 ± 0.9 | 3.7 ± 0.8 | |
| Mild (≤ 3) | 12 (25.5) | 5 (29.4) | 7 (23.3) | 0.84 |
| Moderate/severe (> 3) | 35 (74.5) | 12 (70.6) | 23 (76.7) | 0.73 |
| Characteristic | Overall | Intervention | Control |
|
|---|---|---|---|---|
|
|
|
| ||
|
|
|
| ||
| Change in desire to have a baby | ||||
| No change | 39 (84.8) | 16 (100.0) | 23 (76.7) | 0.10 |
| Yes to no | 6 (13.0) | 0 (0.0) | 6 (20.0) | |
| No to yes | 1 (2.2) | 0 (0.0) | 1 (3.3) | |
| Improvement in fertility or pregnancy concerns at 24 weeks (changed from > 3 to ≤ 3) | 9 (19.2) | 6 (35.3) | 3 (10.0) |
|
| Improvement in personal health or child health concerns at 24 weeks (changed from > 3 to ≤ 3) | 12 (25.5) | 4 (23.5) | 8 (26.7) | 1.00 |
| Fertility specialist referral, visit, or treatment | ||||
| No referral, visit, or treatment | 38 (82.6) | 10 (62.5) | 28 (93.3) |
|
| Received referral/appointment/treatment | 8 (17.4) | 6 (37.5) | 2 (6.7) | |
| Talked with a healthcare provider about managing women's health issues? | ||||
| No, thinking about it | 4 (8.7) | 0 (0.0) | 4 (13.3) |
|
| No, but plan | 6 (13.0) | 5 (31.3) | 1 (3.3) | |
| Yes | 36 (78.3) | 11 (68.8) | 25 (83.3) | |
- —California Breast Cancer Research Program10.13039/100004802
- —Dedman Family Scholar in Clinical Care
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Biology and Fertility · Cancer Risks and Factors · Reproductive Health and Technologies
Introduction
1
There are over 4 million breast cancer survivors in the United States [1]. At diagnosis, 7% of new cases occur in women aged 50 and younger [1]. To be cured, most young breast cancer survivors (YBCS) receive chemotherapy and/or endocrine therapy, treatments that can have a significant impact on reproductive health. Chemotherapy and endocrine therapy may damage ovarian function, resulting in significant reproductive health problems [2, 3]. Hot flashes, sexual dysfunction, limited contraception choices, and infertility may negatively impact survivors' quality of life [4, 5, 6, 7, 8]. Infertility is a distressing consequence of breast cancer treatment among YBCS who desire to have biological children in the future [9, 10]. Evidence‐based clinical strategies geared toward management of reproductive late effects have been developed, but dissemination is limited among YBCS and their healthcare providers [8, 11, 12, 13, 14], leading to significant unmet informational needs among YBCS [15, 16].
The web‐based Survivorship Care Plan on Reproductive Health (SCP‐R) intervention was created to address unmet informational and clinical management needs for YBCS regarding reproductive health‐related problems, including hot flashes, fertility‐related concerns, contraception, and sexual health. Research results, professional society guidelines, and clinical expertise on these issues were combined into management strategies for YBCS and their healthcare providers and delivered via web‐based SCP‐R intervention accessible to both YBCS and their healthcare providers [17, 18]. The parent trial, a randomized controlled trial of 182 YBCS ages 18–50 at the time of enrollment, showed that the SCP‐R intervention was associated with an improvement of at least one of the four targeted issues, that is, hot flashes, fertility‐related concerns, contraception, and sexual health, by 24 weeks [19].
Since fertility potential and pregnancy health‐related concerns tend to be more prevalent in younger cancer survivors and those without children, the objective of the current secondary analysis was to estimate the SCP‐R intervention effect on fertility and pregnancy‐related concerns and fertility care access in nulliparous breast cancer survivors younger than 40 years of age. This younger, childless cohort faces unique reproductive decision‐making challenges not captured in the parent trial results. Therefore, this current study builds on the prior parent trial by isolating the reproductive‐health component of the SCP‐R and identifying its impact on care‐seeking behavior and concerns within a high‐risk, understudied population. We hypothesized that the intervention would have a greater impact on reproductive concerns and fertility specialist access compared to usual care.
Materials and Methods
2
We conducted a secondary analysis of a web‐based educational intervention (SCP‐R) on reproductive concerns and fertility care access among nulliparous YBCS younger than 40 years of age. The parent study was a randomized controlled trial on reproductive health issues among YBCS, where study staff, YBCS, and healthcare provider participants were blinded to treatment allocation [17, 19]. Female YBCS were recruited through diverse sources, including cancer advocacy organizations, healthcare providers, patient advocate referrals, Research Match, and previous observational studies conducted by the investigators. The eligibility criteria for the parent trial included current age of 18–50 years, age at diagnosis of 18–45 years, Stage 0–III breast cancer, completion of primary cancer treatment, and one or more of the four women's health issues (fertility or pregnancy concerns, estrogen deprivation symptoms, and/or inadequate contraception). Survivors with ongoing pregnancies were ineligible for the parent trial. After completing an enrollment questionnaire, YBCS participants were randomized in a 1:1 ratio to the intervention and waitlist control arms. All participants were followed longitudinally for 24 weeks and completed questionnaires at 12‐week and 24‐week follow‐ups. The UC San Diego Institutional Review Board approved all study procedures, and the trial was registered at clinicaltrials.gov (NCT02667626).
The SCP‐R intervention included four sections on fertility‐related concerns: (1) a survivorship care plan (SCP) presented in a question‐and‐answer format; (2) a systematic review results summary with online references to primary research articles; (3) a summary of clinical guidelines with online references; and (4) a list of curated additional online resources (Appendix S1). The SCP‐R intervention highlighted actionable steps that would prompt participants to schedule appointments with healthcare providers to address concerns and reproductive health needs. Participants in the intervention arm were given access to the web‐based SCP‐R materials and received biweekly text message reminders focused on reproductive health. Participants in the attention control arm were given access to a list of curated online resources and received text messages on study adherence.
The online enrollment questionnaire focused on demographics, cancer and treatment characteristics, reproductive health and health behaviors, fertility and pregnancy concerns, hot flashes, vaginal symptoms, and contraception. Questionnaires administered at 12 and 24 weeks focused on reproductive health and health behaviors, reproductive concerns, hot flashes, vaginal symptoms, and contraception. Fertility‐related concerns were measured using the Reproductive Concerns After Cancer (RCAC) scale, an 18‐item multidimensional scale composed of individual subscales (fertility potential, pregnancy, child's health, partner disclosure of fertility status, personal health, and acceptance of infertility), measuring reproductive health concerns of young adult female cancer survivors [20]. Each subscale consists of three questions, with response options ranging from 1 (strongly disagree) to 3 (neither agree nor disagree) to 5 (strongly agree). A mean score of 3 or greater on a 5‐point Likert scale of RCAC is used to categorize individuals as having moderate to severe reproductive concerns [21]. In this current study, we focused on fertility potential and pregnancy RCAC subscales, since the SCP‐R intervention content addressed these specific areas (Table S1) [21].
Statistical Analysis
2.1
We restricted the analysis to nulliparous YBCS aged 18–40 years. Participants with a history of hysterectomy and/or bilateral oophorectomy were excluded from this analysis (n = 3).
Descriptive statistics were calculated as frequencies and percentages or means and standard deviations (SDs), as applicable. The primary outcome of interest was relative improvement in the mean fertility potential or pregnancy concerns subscale score to ≤ 3 by 24 weeks among participants who had moderate/severe concerns (> 3). Scores for the fertility potential and pregnancy subscales were calculated by averaging responses (range: 1–5), with scores > 3 indicating moderate to severe concerns [21]. The secondary outcomes were fertility specialist referral, consultation, and/or fertility treatment by 24 weeks. Bivariate analysis was performed using Fisher's exact test or chi‐square test of proportions to compare outcomes of interest between the intervention and waitlist control arms. Relative risk was calculated for the primary and secondary outcomes. Statistical significance was set at p < 0.05. All analyses were conducted using the SAS statistical software.
Results
3
Participants were enrolled between March 2016 and April 2017. Among 182 randomized participants, 47 were eligible for the current analysis (Figure 1). The baseline characteristics and reproductive health issues of the intervention and waitlist control arms are presented in Table 1. The mean age (SD) was 34.2 (±3.8) years. Most of the participants were white (83%), college graduates (93%), and reported being in partnered relationships (66%). Mean age at breast cancer diagnosis (SD) was 30.7 (±3.5) years. Over 50% of the participants were 3 or more years after cancer diagnosis. Breast cancer treatment included surgery (100%), chemotherapy (89%), hormonal therapy (78%), radiation therapy (66%), and biologic therapy (29%). No significant differences were observed between the intervention and waitlist control arms at baseline, except for hormonal treatment exposure (more patients in the control arm were exposed to hormonal therapy [90%] vs. intervention [59%], p = 0.02).
Flow diagram for young breast cancer survivors (YBCS) study participants.
Sixty‐three percent of the participants desired to have a baby in the future, and an additional 17% reported, while feeling unsure, that they would probably want a baby in the future. Seventy‐two percent of the participants visited a fertility specialist at the time of diagnosis. At baseline, 72% of the participants reported moderate to high fertility potential concerns, 48% reported elevated pregnancy‐related concerns, 61% reported elevated personal health concerns, and 74% had elevated child health concerns. The baseline characteristics were similar between the two arms.
At trial completion, we observed improvement in fertility potential or pregnancy‐related concerns (35.3% improvement in the intervention arm vs. 10.0% improvement in the attention control arm; RR = 3.5, 95% CI = 1.01–12.34, p = 0.05) (Table 2). Additionally, intervention arm participants were more likely to have received a fertility specialist referral, scheduled a fertility consultation appointment, or undergone fertility treatment (37.5% in the intervention arm vs. 6.7% in the attention control arm; RR = 5.6, 95% CI = 1.28–24.73, p = 0.02). Six individuals in the intervention arm saw a fertility specialist (five individuals received a referral before the visit, and one person scheduled an appointment without a referral); three of those six underwent fertility treatment. In contrast, two individuals in the control arm saw a fertility specialist (one person received a referral and one scheduled an appointment without being referred); one of those two underwent fertility treatment. More participants in the control arm planned or talked with their healthcare provider about managing targeted issues than did those in the intervention arm (p = 0.02). We did not observe a significant change in the desire or time horizon to have a baby or personal and child health concerns.
Discussion
4
A web‐based educational intervention focused on reproductive health was shown to be effective in improving fertility potential or pregnancy‐related concerns among nulliparous YBCS aged 18–40 years and prompted YBCS to seek help from a fertility specialist or other healthcare providers to address their reproductive health concerns. These results support a low‐cost evidence‐based intervention strategy geared toward addressing young cancer survivors' reproductive health needs.
Since breast cancer treatment and its duration can shorten the reproductive window and delay the ability to attain family‐building goals, breast cancer may be even more distressing for reproductive‐aged young females than for older individuals [22, 23, 24]. In our nulliparous YBCS cohort, most participants wanted to have children in the future. Previous studies have shown that young adult female cancer survivors have increased reproductive concerns and unmet informational needs, resulting in a poorer quality of life [4]. Moreover, an increased level of reproductive concerns was associated with greater odds of experiencing moderate‐to‐severe depression among 200 young female cancer survivors [25]. Currently, effective methods to alleviate these reproductive health concerns and disseminate evidence‐based information to YBCS are lacking. The SCP‐R parent trial was the first to address these concerns via a web‐based educational intervention that specifically focused on reproductive health issues [19].
In this current secondary analysis, we observed a greater than threefold improvement in fertility potential and pregnancy‐related concerns among participants randomized to the intervention arm, as measured by the RCAC scale. The RCAC scale is an effective tool for identifying young cancer survivors' concerns related to fertility and parenthood and may be useful for long‐term follow‐up care to assess the reproductive health needs of young women with a history of cancer [20]. Since the original publication on the development of the scale in 2014, multiple studies have applied it [26, 27, 28]. Re‐evaluation of the scale in a sample of 238 female reproductive‐aged cancer survivors (younger than 45 years) suggested that the RCAC may be implemented to assess the six subscale domains and allow for tailoring recommendations and interventions to address specific concerns of female reproductive‐aged cancer survivors [21]. Therefore, in our current study, we focused on the RCAC subscales of fertility potential and pregnancy concerns relevant to the SCP‐R intervention effects at 24 weeks.
Intervention materials were provided in a question‐answer format with the ability to conveniently seek more details from the original resources and guidelines, if desired. It is possible that the information provided in the SCP‐R was sufficient to alleviate some of the fertility potential and pregnancy‐related concerns. This may explain why fewer intervention participants planned to or talked with their healthcare provider about managing targeted issues than those in the control arm. Additionally, the SCP‐R highlighted actionable steps that would prompt participants to schedule appointments with fertility specialists to address reproductive health needs, and more participants in the intervention arm received a fertility specialist referral compared to those in the control arm. Guiding young cancer survivors to fertility specialists is an important goal of oncology and primary care providers that could be facilitated by the SCP‐R or a similar intervention.
SCPs have been proposed as a modality to help survivors navigate survivorship and are currently recommended for all cancer survivors [29]. However, reproductive health‐related survivorship needs are not adequately addressed in current SCPs. A systematic review examining the impact of SCPs showed that although SCPs appear to be feasible and may improve healthcare providers' knowledge of late effects and general survivorship care, there is little evidence that SCPs affect cancer survivors' patient‐reported outcomes [30]. In contrast, our SCP‐R intervention had a positive impact on young cancer survivors' reproductive health concerns and prompted reproductive care‐seeking behaviors. The lack of improvement observed among control group participants, who received only curated online resources with hyperlinks, highlights that providing access to information may not be sufficient to address reproductive health concerns. Rather, more specific reproductive health content and self‐management tools with SCPs may be necessary.
Therefore, our SCP‐R intervention could potentially be incorporated into general SCPs and serve as an additional dialogue‐initiating, personalized tool between cancer survivors and their healthcare providers. Our study highlights the need for SCPs and other interventions to not only inform cancer survivors but also prompt actions and support survivors through decisions related to their reproductive health, including seeking referrals to fertility care. The incorporation and promotion of supportive care programs dedicated to young women with breast cancer, such as the one presented in the study of fertility preservation in young women with breast cancer in Mexico, may be valuable strategies [31]. In addition, interventions such as SCP‐R can serve as an example of late effect‐specific SCPs for cancer survivors (e.g., for reproductive health, cardiac health, and cancer predisposition screening post‐therapy).
Our findings complement and extend those from the parent trial [19], which reported improvement across multiple women's health domains in a broader cohort of YBCS aged 18–50. By focusing exclusively on nulliparous YBCS under 40 years, we demonstrate that the SCP‐R intervention yields a greater than 3‐fold improvement in fertility potential and pregnancy‐related concerns and a 5.6‐fold increase in fertility specialist referral or treatment. Thus, this work uniquely delineates the reproductive health impact of the SCP‐R among those most likely to experience fertility distress, supporting the clinical value of age‐ and parity‐specific tailoring of SCPs. Further, recent studies highlight the global relevance of these findings and emphasize the importance of addressing fertility needs among young cancer survivors from diverse populations [10, 31, 32].
This study had several limitations. First, most participants were white, highly educated, and recruited from advocacy organizations, limiting the generalizability of the results. However, the SCP‐R content can be adapted for other populations, most recently for Spanish‐speaking, Hispanic breast cancer survivors [32]. Second, a higher percentage of participants in the control group required hormone therapy than in the intervention group. This indicates higher rates of hormone‐negative, more aggressive breast cancer in the intervention group, which may have made the two groups less comparable. Third, we had a small number of participants who were 40 years old and younger, with no history of live births. Additionally, the short follow‐up time of 24 weeks makes it difficult to assess whether more YBCS would follow up with a fertility specialist and utilize fertility treatments. Finally, in this study, we relied on self‐reported intentions or actions regarding fertility care. Strategies to overcome these limitations should be considered when designing future studies to improve reproductive care in YBCS.
Conclusions
5
While the parent trial included all reproductive‐aged YBCS aged 18–50 years, this secondary analysis focused on a high‐risk subgroup of nulliparous YBCS aged 18–40 years. The web‐based SCP‐R intervention improved fertility potential and pregnancy‐related concerns over time and encouraged access to fertility care, highlighting the importance of age‐ and parity‐specific survivorship care interventions. More research is needed to better understand personalized and targeted approaches for optimal fertility care among nulliparous YBCS and dissemination strategies for the SCP‐R intervention.
Author Contributions
Ksenya Shliakhtsitsava: conceptualization (equal), data curation (equal), formal analysis (equal), investigation (equal), methodology (equal), validation (equal), visualization (equal), writing – original draft (lead), writing – review and editing (lead). Shaylyn S. Stark: conceptualization (equal), data curation (equal), formal analysis (equal), funding acquisition (supporting), investigation (supporting), methodology (supporting), project administration (equal), resources (supporting), software (supporting), supervision (equal), validation (equal), visualization (equal), writing – original draft (supporting), writing – review and editing (supporting). Tanushree Prasad: formal analysis (supporting), methodology (supporting), software (supporting), writing – review and editing (equal). Sarah Boles: investigation (supporting), methodology (supporting), resources (supporting), writing – review and editing (supporting). Diana Chingos: conceptualization (equal), data curation (supporting), funding acquisition (supporting), investigation (supporting), methodology (supporting), writing – review and editing (supporting). Jennifer Ehren: conceptualization (equal), funding acquisition (supporting), investigation (supporting), methodology (supporting), supervision (supporting), writing – review and editing (supporting). Jessica R. Gorman: conceptualization (equal), data curation (equal), formal analysis (supporting), funding acquisition (supporting), investigation (supporting), methodology (equal), project administration (supporting), resources (supporting), writing – review and editing (supporting). Sally A. D. Romero: conceptualization (equal), data curation (equal), formal analysis (equal), funding acquisition (supporting), investigation (supporting), methodology (equal), project administration (lead), resources (supporting), software (supporting), supervision (lead), validation (equal), visualization (equal), writing – original draft (supporting), writing – review and editing (supporting). Jun J. Mao: conceptualization (equal), funding acquisition (equal), investigation (equal), methodology (equal), supervision (equal), visualization (equal), writing – review and editing (equal). Paul Nathan: resources (supporting), supervision (supporting), validation (supporting), visualization (supporting), writing – review and editing (supporting). Saro H. Armenian: conceptualization (supporting), methodology (supporting), supervision (supporting), validation (equal), visualization (equal), writing – review and editing (equal). H. Irene Su: conceptualization (lead), data curation (lead), formal analysis (lead), funding acquisition (lead), investigation (lead), methodology (lead), project administration (equal), resources (lead), software (lead), supervision (lead), validation (equal), writing – original draft (equal), writing – review and editing (equal).
Funding
This work was supported by the California Breast Cancer Research Program Translational Award 20OB‐0144 (all authors) and the P30‐CA008748 (J.J.M.). The funders had no involvement in the study design, data collection, analysis, and interpretation of data, writing of the manuscript, or decision to submit the article for publication. Additionally, Ksenya Shliakhtsitsava is a Dedman Family Scholar in Clinical Care.
Ethics Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. This study was approved by the Ethics Committee of the University of California, San Diego (IRB Number 140863).
Consent
Informed consent was obtained from all individual participants included in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Appendix S1: Sample of SCP‐R content on fertility‐related concerns for participants randomized to the intervention arm. Similar materials were provided for hot flashes, contraception, sexual health, and cancer genetic risk. Participants randomized to the attention control arm were only able to access the list of curated web‐based resources with hyperlinks. Table S1: The Reproductive Concerns After Cancer (RCAC) scale details. Highlighted in green are the subscales included in this analysis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1N. S. Wagle , L. Nogueira , T. P. Devasia , et al., “Cancer Treatment and Survivorship Statistics, 2025,” CA: A Cancer Journal for Clinicians 75 (2025): 308–340.40445120 10.3322/caac.70011 PMC 12223361 · doi ↗ · pubmed ↗
- 2H. I. Su , M. D. Sammel , J. Green , et al., “Antimullerian Hormone and Inhibin B Are Hormone Measures of Ovarian Function in Late Reproductive‐Aged Breast Cancer Survivors,” Cancer 116 (2010): 592–599.19918920 10.1002/cncr.24746 PMC 2815049 · doi ↗ · pubmed ↗
- 3S. Yildiz , G. Bildik , C. Benlioglu , et al., “Breast Cancer Treatment and Ovarian Function,” Reproductive Biomedicine Online 46 (2023): 313–331.36400663 10.1016/j.rbmo.2022.09.014 · doi ↗ · pubmed ↗
- 4J. R. Gorman , S. Bailey , J. P. Pierce , and H. I. Su , “How Do You Feel About Fertility and Parenthood? The Voices of Young Female Cancer Survivors,” Journal of Cancer Survivorship 6 (2012): 200–209.22179785 10.1007/s 11764-011-0211-9PMC 3667153 · doi ↗ · pubmed ↗
- 5Y. C. Chang , S. R. Chang , and S. C. Chiu , “Sexual Problems of Patients With Breast Cancer After Treatment: A Systematic Review,” Cancer Nursing 42 (2019): 418–425.29621025 10.1097/NCC.0000000000000592 · doi ↗ · pubmed ↗
- 6H. Y. Chang , A. C. Jotwani , Y. H. Lai , et al., “Hot Flashes in Breast Cancer Survivors: Frequency, Severity and Impact,” Breast 27 (2016): 116–121.27065357 10.1016/j.breast.2016.02.013PMC 5893329 · doi ↗ · pubmed ↗
- 7J. Howard‐Anderson , P. A. Ganz , J. E. Bower , and A. L. Stanton , “Quality of Life, Fertility Concerns, and Behavioral Health Outcomes in Younger Breast Cancer Survivors: A Systematic Review,” Journal of the National Cancer Institute 104 (2012): 386–405.22271773 10.1093/jnci/djr 541 · doi ↗ · pubmed ↗
- 8M. Peate , B. Meiser , M. Hickey , and M. Friedlander , “The Fertility‐Related Concerns, Needs and Preferences of Younger Women With Breast Cancer: A Systematic Review,” Breast Cancer Research and Treatment 116 (2009): 215–223.19390962 10.1007/s 10549-009-0401-6 · doi ↗ · pubmed ↗