Spontaneous Coronary Artery Dissection in an Elderly Postmenopausal Nigerian Woman With Recurrent Chest Pain: A Case Report
Olurotimi J Badero, Oyewole Kushimo, Bamikole Osibowale, Victor Ajayi, Adaobi Ofordile

TL;DR
This case report describes a rare instance of spontaneous coronary artery dissection in an elderly postmenopausal Nigerian woman, highlighting the importance of early diagnosis and management.
Contribution
The paper presents one of the earliest documented cases of postmenopausal SCAD in Nigeria diagnosed via coronary angiography.
Findings
SCAD was diagnosed angiographically in a 75-year-old postmenopausal woman with recurrent chest pain.
The case highlights the rarity of postmenopausal SCAD and the need for increased awareness and suspicion for accurate diagnosis.
Abstract
Spontaneous coronary artery dissection (SCAD) is an unusual etiology of myocardial infarction and sudden cardiac death (SCD) with a different pathophysiological mechanism. Often associated with younger women, where the hormonal milieu of estrogen and progesterone has been implicated, postmenopausal SCAD is, however, uncommon with unknown management outcomes. We report the case of a 75-year-old postmenopausal woman presenting with recurrent chest pain, found to have SCAD on coronary angiography, and managed conservatively. We believe this represents one of the earliest documented cases of postmenopausal SCAD in Nigeria diagnosed angiographically. It seeks to enhance local awareness, review current diagnostic and management modalities, and contribute to the expanding body of literature. SCAD can present as acute coronary syndrome (ACS) in young women, where the hormonal milieu has been…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
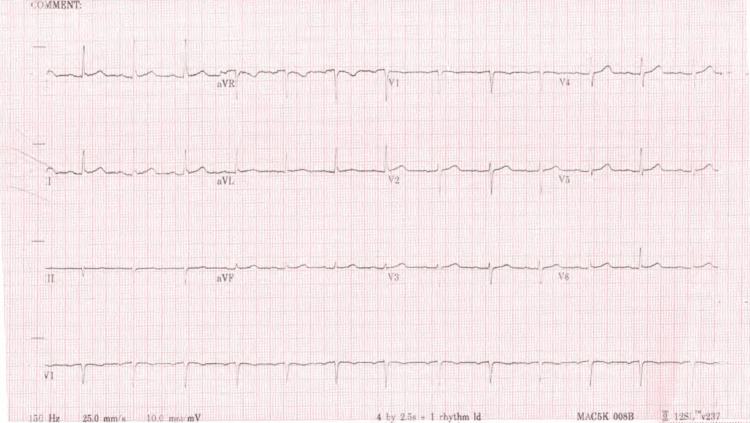 Figure 1
Figure 1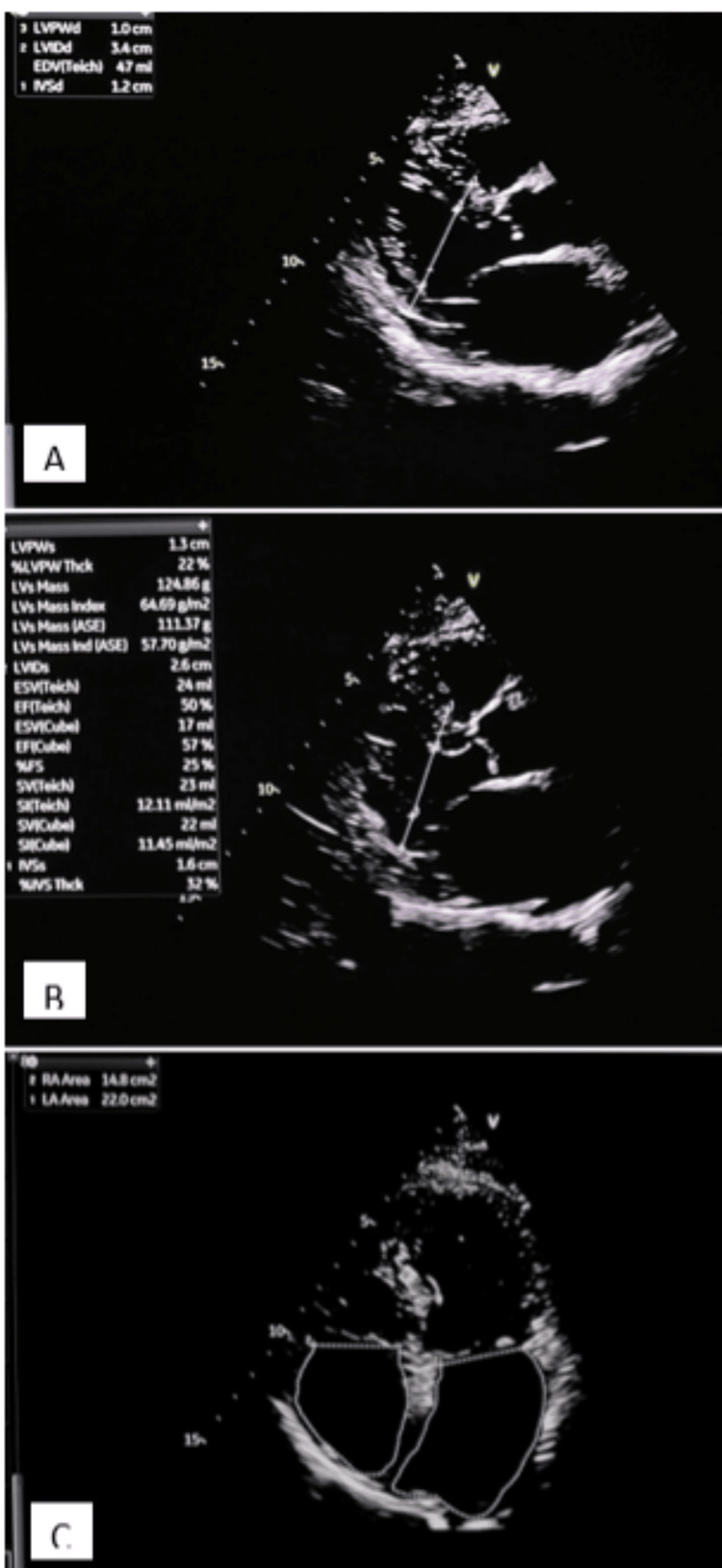 Figure 2
Figure 2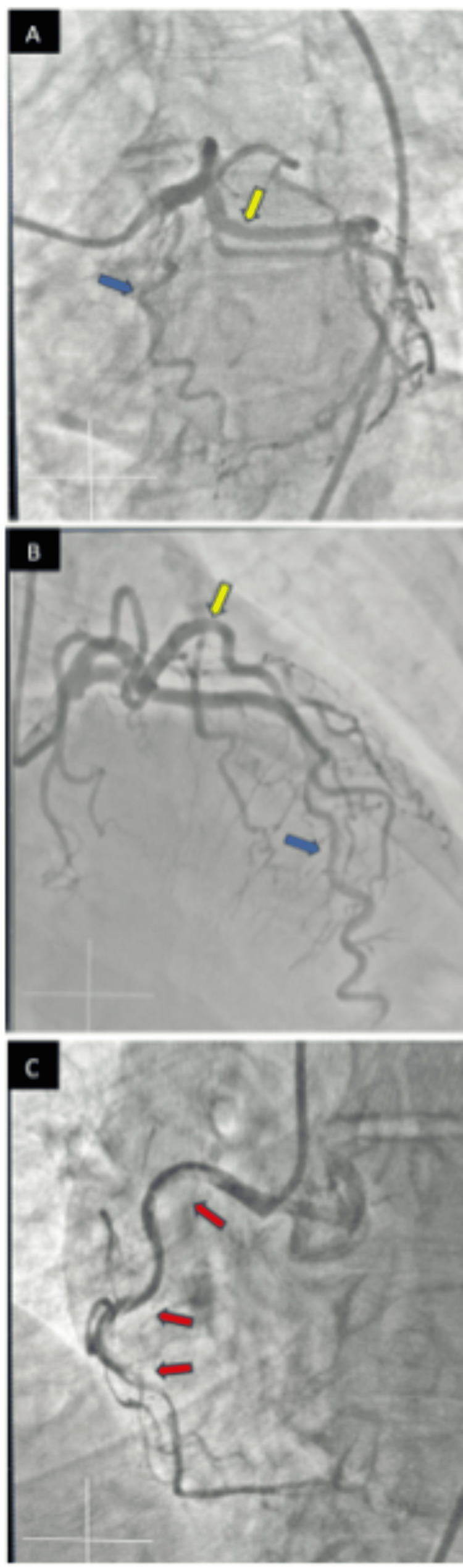 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Issues in Pregnancy · Cardiac Imaging and Diagnostics · Takotsubo Cardiomyopathy and Associated Phenomena
Introduction
Spontaneous coronary artery dissection, a previously presumed rare entity, is now being recognized as an important etiology of acute coronary syndrome (ACS) and sudden cardiac death (SCD) among younger women [1]. It is characterized by a spontaneous, non-atherosclerotic, non-traumatic, and non-iatrogenic separation of the coronary artery wall by an intramural hematoma, which may or may not be associated with an intimal tear. The accumulation of blood within the arterial wall can compress the true lumen, reducing coronary blood flow and potentially leading to myocardial ischemia or infarction [2].
SCAD predominantly affects younger premenopausal women, with the mean age of diagnosis spanning 44-55 years [3]; hence, SCAD in an older postmenopausal woman is unusual. The overall prevalence of SCAD is reported to be about 4% of all ACS and is responsible for about 35% of ACS seen in women younger than 50 years [4].
The clinical presentation of SCAD mirrors that of atherosclerotic plaque rupture-induced ACS, typically manifesting as classic chest pain accompanied by diagnostic ECG abnormalities and elevated cardiac biomarkers. However, traditional cardiovascular risks are usually absent. The diagnosis of SCAD has been enhanced by advanced imaging techniques, including optical coherence tomography (OCT) and intravascular ultrasound (IVUS), especially in patients with unusual angiographic patterns. However, their availability remains limited in developing countries.
Older patients with SCAD exhibit a distinct clinical and angiographic phenotype compared to their younger counterparts, with different initial treatment strategies, but similar in-hospital outcomes [4].
We present a 75-year-old Nigerian woman with hypertension, diabetes, and chronic kidney disease (CKD) who was diagnosed with SCAD. This case highlights the need for a high index of suspicion among older women presenting with ACS.
Case presentation
A 75-year-old woman with past medical history significant for type 2 diabetes mellitus, hypertension, and chronic kidney disease (CKD) stage 4 with an estimated glomerular filtration rate (eGFR) of 25 cc/minute per chronic kidney disease-epidemiology collaboration (CKD-EPI), was evaluated at the cardiology clinic for chest pain. The chest pain was described as stabbing in nature, mid-sternal in location, exertional, and associated with nausea and shortness of breath. The symptoms had progressively worsened in frequency and severity over the previous weeks, with symptoms now occurring at rest.
An electrocardiogram showed a normal sinus rhythm with no acute ST-T wave changes (Figure 1). Echocardiography demonstrated left ventricular (LV) concentric hypertrophy with a low normal LV ejection fraction of 50% and a dilated left atrium (Figure 2). There was no significant valvular disease. A diagnosis of unstable angina was made with a thrombolysis in myocardial infarction (TIMI) risk score of 3. She was planned for an early invasive strategy with a coronary angiogram.
Electrocardiographic image showing normal sinus rhythm
Echocardiographic images showing concentric left ventricular hypertrophy and dilated left atriumA: Parasternal long-axis view in systole, with EF of 50%. B: Parasternal long-axis view in diastole; the interventricular septal wall thickness in diastole measures 1.2 cm. C: Apical four-chamber view showing dilated left atrium; the left atrial area measures 22 cm2.EF: ejection fraction
Coronary angiography in multiple orthogonal views was performed the next day under moderate sedation via right common femoral access using JL-4 and JR-4 diagnostic catheters. Coronary angiogram findings revealed angiographically normal left main, tortuous left anterior descending artery with mild luminal irregularities, and angiographically normal left circumflex artery (Figure 3A and Figure 3B). The right coronary artery showed a type 1 SCAD involving the proximal, mid, and distal segments of the artery (Figure 3C). She was managed medically with aspirin and beta-blockers with close follow-up.
Angiographic imagesA: Coronary angiogram showing left anterior descending (blue arrow) and left circumflex (yellow arrow). B: Coronary angiogram showing left anterior descending (blue arrow) and left circumflex (yellow arrow). C: Coronary angiogram showing right coronary artery with spontaneous coronary artery dissection (red arrows).
Our patient has been doing well on follow-up but continues to experience intermittent episodes of chest pain with decreased frequency and intensity from the initial presentation. She has not reported any chest pain at rest. She is being continued on beta-blockers and aspirin with risk factor and lifestyle modification.
Discussion
SCAD is a non-traumatic and non-iatrogenic coronary event that involves the formation of a hematoma within the tunica media complex, resulting in the splitting of the innermost layer of the blood vessel wall (intima) from the rest of the wall, forming a flap that squeezes the main channel and restricts blood flow, causing ischemia or a myocardial infarction [3,5]. SCAD is reported more commonly in the cohort of premenopausal women with an ACS. A case of SCAD has been reported in a premenopausal Nigerian woman with pregnancy-associated acute myocardial infarction [6]. We, however, report the first case of SCAD in an elderly postmenopausal woman in Nigeria [6]. The occurrence of SCAD in postmenopausal women highlights the multifactorial nature of the conditions and the need to consider other non-hormonal factors, such as connective tissue disorders (fibromuscular dysplasia, Marfan’s syndrome, and Ehlers-Danlos syndrome), and genetic predisposition [3,5].
Some differences in SCAD characteristics have been identified in postmenopausal women. A Spanish multicenter registry noted that postmenopausal women had a previous history of acute coronary syndrome more often but presented less frequently as ST-segment elevation myocardial infarction on admission and less frequently with left ventricular dysfunction compared with premenopausal women [7]. These characteristics were noted in our index patient, who presented with unstable angina and preserved LV systolic function. Older patients were also observed to have hypertension and dyslipidemia, with an identifiable trigger less often present. They also more often had severe coronary tortuosity (like our patient) and coronary ectasia. There was no significant difference in major adverse cardiac events, heart failure, or in-hospital stay during the index admission compared to younger patients [7].
The diagnosis of SCAD is often made by invasive coronary angiography. Additional intravascular imaging with OCT or IVUS is reserved for cases of diagnostic uncertainty or when percutaneous coronary intervention (PCI) is anticipated. Most cases of SCAD are managed conservatively in view of the high probability of spontaneous healing and the high risks of revascularization. A study that analyzed patients with SCAD who had a subsequent coronary angiography for diverse indications showed that 95% had angiographic healing 30 days post-event [8]. In as many as one-third of PCI procedures, the intramural hematoma propagates frequently, necessitating the use of several unplanned stents [9]. As the hematoma resorbs, it may lead to late strut misalignment [3].
Conservative management, especially in the acute phase, can lead to complete healing and is usually recommended, as percutaneous coronary intervention (PCI) is associated with high failure rates and iatrogenic dissections. We adopted a conservative approach in our patient, given preserved vessel flow and the absence of ongoing ischemia.
Conclusions
Spontaneous coronary artery dissection (SCAD) remains an infrequent, elusive, and challenging clinical entity of multifactorial etiology, many years after it was first described. Intravascular imaging may be necessary when the diagnosis is uncertain, and a conservative approach has been shown to give the best outcomes. Increased awareness of this condition, particularly in developing countries, is crucial, and more research needs to be done to further understand this entity and add to the growing body of literature.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spontaneous coronary artery dissection (SCAD): a contemporary review Clin Cardiol Offen S Yang C Saw J 047202410.1002/clc.24236 PMC 1116516938859725 · doi ↗ · pubmed ↗
- 2Canadian spontaneous coronary artery dissection cohort study: 3-year outcomes J Am Coll Cardiol Saw J Starovoytov A Aymong E 158515978020223626595310.1016/j.jacc.2022.08.759 · doi ↗ · pubmed ↗
- 3Spontaneous coronary artery dissection: JACC state-of-the-art review J Am Coll Cardiol Hayes SN Tweet MS Adlam D Kim ES Gulati R Price JE Rose CH 9619847620203281947110.1016/j.jacc.2020.05.084 · doi ↗ · pubmed ↗
- 4Spontaneous coronary artery dissection unveiled: pathophysiology, imaging, and evolving management strategies J Cardiovasc Dev Dis Rusali CA Lupu IC Rusali LM Cojocaru L 12202510.3390/jcdd 12080286 PMC 1238709140863352 · doi ↗ · pubmed ↗
- 5Spontaneous coronary artery dissection-a review Cardiovasc Diagn Ther Yip A Saw J 3748520152577434610.3978/j.issn.2223-3652.2015.01.08PMC 4329168 · doi ↗ · pubmed ↗
- 6Pregnancy-associated acute myocardial infarction (PAMI): case report West Afr J Med Ogah OS Osibowale BT Adebayo O 596598382021 https://pubmed.ncbi.nlm.nih.gov/34180213/34180213 · pubmed ↗
- 7Spontaneous coronary artery dissection and menopause Am J Cardiol Díez-Villanueva P García-Guimaraes MM Macaya F 535914820213361781310.1016/j.amjcard.2021.02.007 · doi ↗ · pubmed ↗
- 8Spontaneous coronary artery dissection and menopause JACC Cardiovasc Interv Hassan S Prakash R Starovoytov A Saw J 5185271220193117128510.1016/j.jcin.2019.04.023 · doi ↗ · pubmed ↗