The effectiveness of smart healthcare for patients with rheumatoid arthritis: A systematic review and meta-analysis
Yin Yu, Meijiao Wang, Hejing Pan, Lin Huang, Haichang Li, Xuanlin Li

TL;DR
Smart healthcare helps reduce disease activity and improve quality of life for rheumatoid arthritis patients, according to a review of clinical trials.
Contribution
This study provides a meta-analysis of randomized controlled trials evaluating the effectiveness of smart healthcare interventions in rheumatoid arthritis patients.
Findings
Smart healthcare significantly reduced disease activity (DAS28) in rheumatoid arthritis patients.
Quality of life and functional capacity improved significantly with smart healthcare interventions.
No significant effects were observed on self-efficacy, self-management, or RA knowledge.
Abstract
This study aimed to evaluate the impact of smart healthcare interventions on disease activity, self-efficacy, self-management, functional levels, and quality of life in rheumatoid arthritis (RA) patients, as well as any associated adverse events. A systematic search was conducted in PubMed, EMBASE, and Cochrane Library for randomized controlled trials (RCTs) from inception to August 2024, using relevant medical subject headings and keywords. The Cochrane risk of bias tool was employed to assess bias risk. A random effects model was used, calculating the standardized mean difference (SMD) and 95% confidence intervals (CIs). Heterogeneity was assessed with Chi-square and I2 tests. This meta-analysis included 18 RCTs published between 2015 and 2024, with follow-up periods ranging from 3 months to 1 year. Results revealed a significant reduction in Disease Activity Score 28 (DAS28) in the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
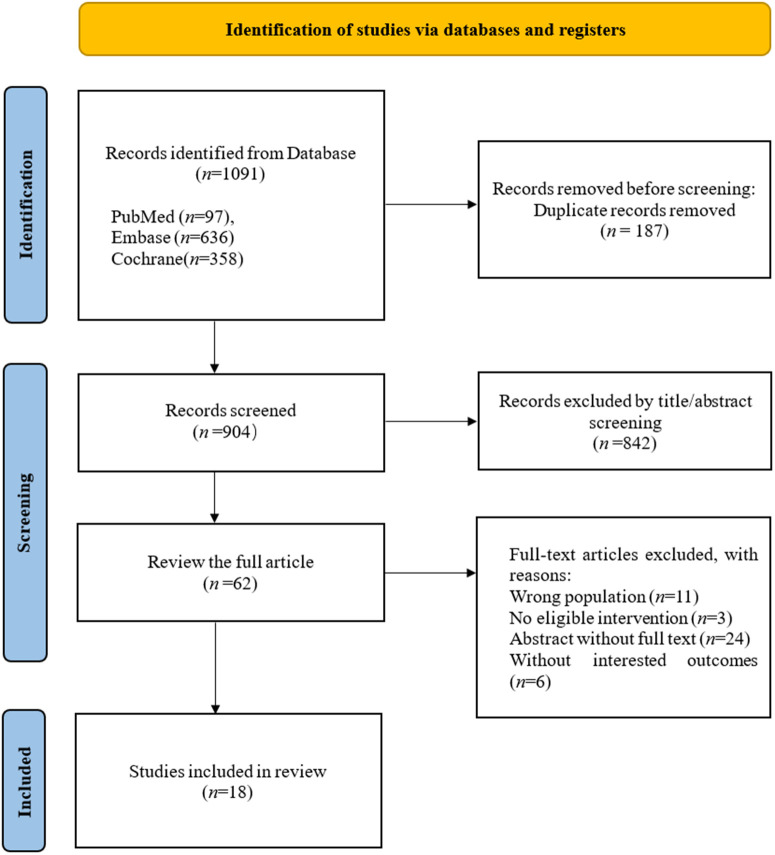 Fig 1
Fig 1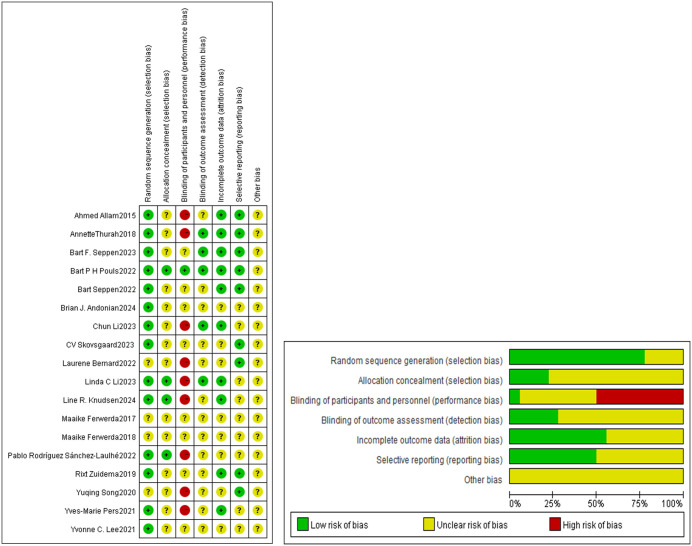 Fig 2
Fig 2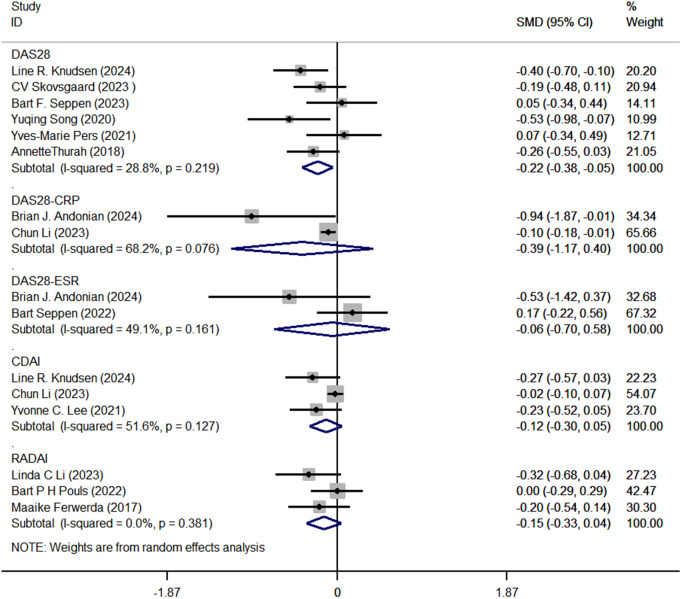 Fig 3
Fig 3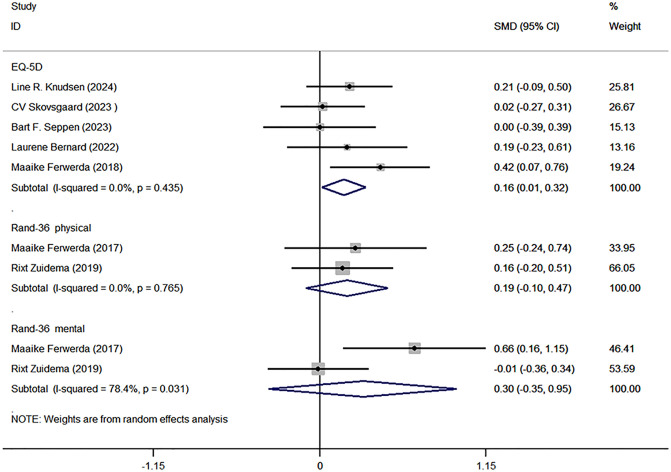 Fig 4
Fig 4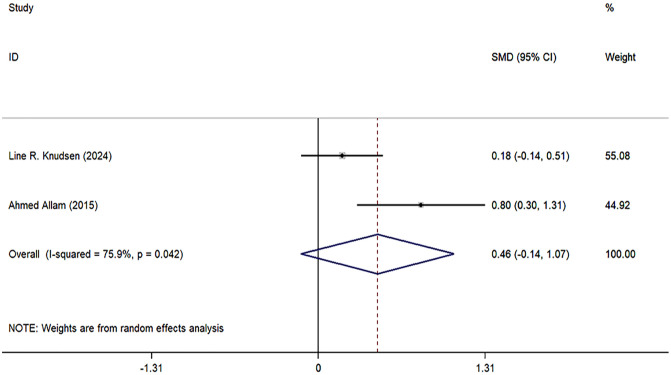 Fig 5
Fig 5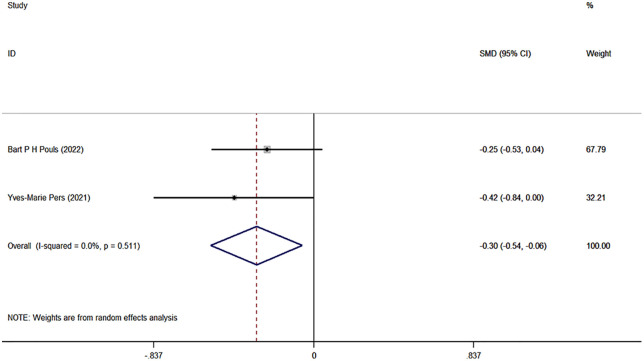 Fig 6
Fig 6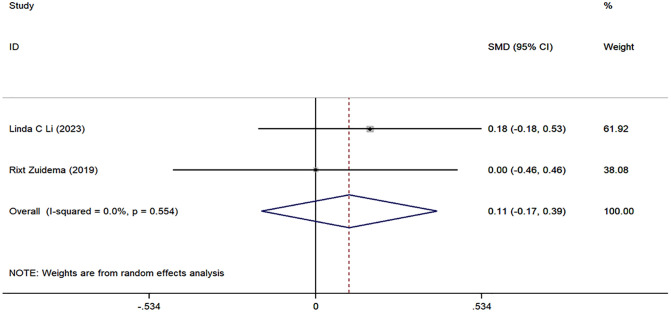 Fig 7
Fig 7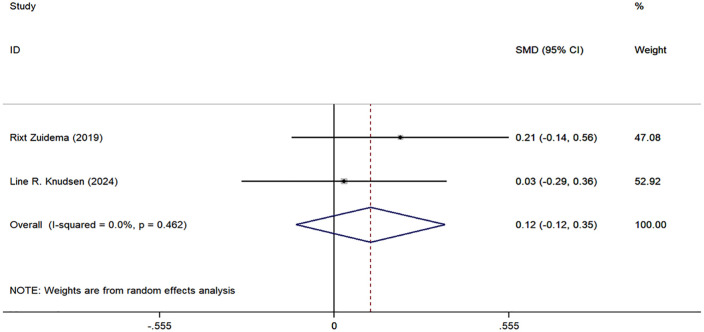 Fig 8
Fig 8- —Natural Science Foundation of Zhejiang Province, China
- —Natural Science Foundation of Zhejiang Province, China
- —Joint project of the State Administration of Traditional Chinese Medicine Science and Technology Department and the Zhejiang Provincial Administration of Traditional Chinese Medicine
- —Zhejiang Province Traditional Chinese Medicine Science and Technology Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRheumatoid Arthritis Research and Therapies · Multiple Sclerosis Research Studies · Spondyloarthritis Studies and Treatments
Introduction
Rheumatoid arthritis (RA) is a prevalent systemic autoimmune disease characterized by symmetrical polyarticular pain, primarily affecting synovial tissues and surrounding soft tissues [1–3]. Its estimated prevalence varies significantly, being higher in industrialized countries, with age-standardized rates of 0.38%, 0.35%, and 0.10% in North America, Western Europe, and Southeast Asia, respectively [2,4,5]. RA disproportionately affects women [6–9], with sex ratios ranging from 4:1 in younger populations to 2:1 in older adults, likely due to hormonal changes in postmenopausal women [2,5,10]. The disease leads to joint damage, functional impairment, psychological distress, and a substantial decline in quality of life, imposing a heavy economic burden on patients and healthcare systems [2,4,5]. Effective management strategies for RA include early diagnosis, goal-oriented therapy, and patient education [2,11,12]. The European Alliance of Associations for Rheumatology (EULAR) emphasizes the importance of achieving remission or low disease activity to improve patient quality of life [13]. Regular monitoring and follow-ups are crucial in this context.
Advancements in information technology have enabled the emergence of smart healthcare interventions, which offer innovative, personalized, and remote approaches to disease management [14,15]. These interventions have demonstrated effectiveness in managing chronic diseases, including RA, by improving medication adherence and self-management skills while reducing outpatient visits and healthcare costs [16–19]. Smart healthcare leverages information and communication technologies (ICTs) to deliver disease management support remotely. This encompasses a continuum of services, ranging from passive dissemination of educational information to active symptom monitoring, personalized self-management support, and remote professional guidance. Despite the diversity in their specific applications, these interventions share a common core: the use of digital tools to transcend the spatiotemporal limitations of traditional clinic-based care, thereby providing continuous support to patients. Previous meta-analyses on this topic are limited, with the most recent study dating back to 2021. These studies encountered methodological challenges, such as inconsistent measurement scales and a lack of reported adverse events [20,21]. Given the rapid advancements in technology and new research findings, this updated meta-analysis aims to provide a comprehensive evaluation of the effectiveness of smart healthcare interventions for patients with RA, thereby enhancing the robustness of existing evidence.
Methods
Protocol and registration
This study was conducted following the Cochrane Handbook for Systematic Reviews of Interventions and the PRISMA guidelines [22,23]. The protocol was pre-registered with the International Prospective Register of Systematic Reviews (PROSPERO), registration number CRD42024582224.
Data sources and search strategy
We systematically searched PubMed, Embase, and the Cochrane Library from inception to August 14, 2024, for relevant RCTs without language restrictions. Our search utilized Medical Subject Headings (MeSH) and keywords, including “Telemedicine,” “digital health,” “mHealth,” “Arthritis, Rheumatoid,” and “Randomized Controlled Trials.” Additionally, we reviewed reference lists of pertinent systematic reviews to enhance our search comprehensiveness. The details of the search strategy were shown in S1 File.
Study selection and eligibility criteria
Eligibility criteria were defined based on the population, intervention, control, outcome, and study design. Two investigators independently assessed study eligibility after removing duplicates, the consistency of the reviews was quantified using Cohen’s Kappa coefficient (κ), and any discrepancies were resolved through discussion with a third reviewer (XL Li). Duplicates were removed prior to screening using the deduplication feature of NoteExpress (Version 4.0.0.9855). We included RCTs focused on smart health interventions for adult rheumatoid arthritis. We incorporated studies that defined RA through both established classification criteria (such as the 1987 American College of Rheumatology (ACR) criteria or the 2010 ACR/EULAR criteria) and those based on a physician’s clinical diagnosis. However, due to the lack of a uniform diagnostic standard across the literature, it was not feasible to apply a single, unified RA case definition across all studies. Eligible interventions encompassed all types of smart healthcare interventions, including those enabling symptom tracking and self-management support via health applications or online platforms, as well as telemedicine and teleconsultation services. Studies that did not report outcome data specifically attributable to these smart healthcare components were excluded. Common functions of the included interventions consisted of: automated symptom tracking (e.g., monitoring disease activity indicators such as DAS28 scores); regular remote follow-up (e.g., scheduled consultations via video or messaging); and self-management support (e.g., personalized medication reminders and exercise guidance).
Detailed characteristics of the smart healthcare interventions for RA are summarized in S2 File. The complete inclusion and exclusion criteria are provided in S3 File.
Data extraction and outcome measures
Data extraction was performed independently by two authors, capturing details such as authorship, publication year, study size, duration, country, design, blinding, and participant demographics. We also recorded intervention types, comparison groups, and outcomes, including primary and secondary endpoints like disease activity, self-efficacy, quality of life, and adverse events. For incomplete data, authors were contacted for clarification.
The primary endpoint was the mean difference in disease activity, while secondary endpoints included self-management and functional changes.
Quality assessment
The Cochrane Collaboration’s tool for assessing risk of bias was utilized [24]. Two independent reviewers (Y Yu and MJ Wang.) evaluated each study across the seven bias domains. Each item was classified as “low,” “unclear,” or “high” risk of bias. Any disagreements in assessments were resolved through discussion until consensus was achieved. When consensus could not be reached, a third senior reviewer (XL Li) was consulted to make the final determination.
Statistical analysis
Statistical analyses were conducted using Stata software (version 14) with meta-analyses performed via a random-effects model to account for clinical heterogeneity. We calculated standardized mean differences (SMD) and 95% confidence intervals (CI) using the inverse variance method. Medians and interquartile ranges were converted to means and standard deviations [25,26]. Heterogeneity was assessed using the Cochrane Q test and quantified with the I^2^ statistic. A two-sided P-value <0.05 was considered statistically significant [27,28], and publication bias was not reported due to the limited number of included studies in each meta-analysis.
Results
Study identification
The initial search yielded 1,091 records. After removing 187 duplicates, we screened the titles and abstracts of the remaining 904 articles, excluding 842. We then evaluated the full text of 62 articles, resulting in the exclusion of 44, and ultimately included 18 RCTs in this meta-analysis [18,19,29–44]. The literature screening process is illustrated in Fig 1. The list of included and excluded articles along with the reasons can be found in S4 File.
PRISMA flow diagram.
Study characteristics
The meta-analysis incorporated 18 RCTs published between 2015 and 2024. Of these, six studies were conducted in the Netherlands [31,36,37,39,41,42], three in Denmark [29,30,33], two in China [18,34], two in France [40], two in United States [35,38],and one each in Canada [31], Spain [44], Switzerland [43]. The majority of participants were women (median percentage across studies: 75.5%), with an average age of approximately 50–60 years. Thirteen studies reported disease activity [18,19,29–39], seven reported quality of life [29–31,37,40–42], two reported RA knowledge [29,43], two reported self-management [19,42], two reported functional level [32,36], and four reported adverse events [19,32,34,44]. Two studies addressed self-efficacy [29,42]. Key characteristics of the included RCTs are presented in Table 1.
Table 1: Characteristics of studies included in the meta-analysis.
Review consistency
The consistency of study selection was assessed using Cohen’s Kappa coefficient. Based on independent evaluations of 62 full-text articles, the κ value was 0.88 (95% CI 0.749–1.012), indicating almost perfect consistency. All discrepancies were resolved through discussion with a third reviewer.
Risk of bias
The risk-of-bias assessment is summarized in Fig 2. All studies utilized randomization; however, only 14 clearly described the random assignment process. Four studies implemented concealment methods, while the others did not specify any concealment procedures. Blinding of participants and personnel was identified as the domain with the highest risk of bias. Only one study maintained blinding for both parties, nine studies did not implement blinding at all, and the remaining studies did not report their blinding status. Five studies ensured blinding during outcome assessment, while others did not disclose whether blinding was applied. In terms of attrition bias, ten studies reported using intention-to-treat analyses or other statistical methods for data management, whereas eight studies remained unclear. For reporting bias, nine studies were deemed to have a low risk, while nine exhibited an unclear risk. Regarding other biases, all eighteen studies were classified as having an unclear risk. S5 File reports the risk of bias for each study.
a. Risk of bias graph.b. Regarding disease activity, six articles reported on the Disease Activity Score (DAS28) [18,29,33]. The pooled analysis revealed a significant decrease in DAS28 scores (SMD with 95% CI: −0.22 [−0.38, −0.05], I2 = 28.8%, P = 0.011). Two articles reported on DAS28-CRP (SMD with 95% CI: −0.22 [−1.17, 0.40], I2 = 68.2%, P = 0.335) [34,38], while two articles reported DAS28-ESR (SMD with 95% CI: −0.06 [−0.70, 0.58], I2 = 49.1%, P = 0.863) [38,39]. Three studies reported on the Clinical Disease Activity Index (CDAI) (SMD with 95% CI: −0.12 [−0.30, 0.05], I2 = 51.6%, P = 0.169) [29,34,35], and three studies reported on the Rheumatoid Arthritis Disease Activity Index (RADAI) (SMD with 95% CI: −0.15 [−0.33, 0.04], I2 = 51.6%, P = 0.128) [19,36,37]. The results concerning disease activity are illustrated in Fig 3.
Forest plots of disease activity.
Quality of life
Quality of life was assessed using the EQ-5D and RAND-36 [45,46]. Five studies reported EQ-5D scores [29–31,40,41], confirming a significant difference between the intervention and control groups (SMD with 95% CI: 0.16 [0.01, 0.32], I^2^ = 0.0%, P = 0.033). Two studies analyzed RAND-36 [37,42], focusing on physical and mental health. The physical component showed no significant difference (SMD with 95% CI: 0.19 [−0.10, 0.47], I^2^ = 0.0%, P = 0.765), while the mental component demonstrated an unclear significance (SMD with 95% CI: 0.30 [−0.35, 0.95], I^2^ = 78.4%, P = 0.369) (Fig 4).
Forest plots of quality of life.
The meta-analysis on RA knowledge, functional level, self-management, and self-efficacy included only two studies. Although we report the combined effect sizes, caution should be exercised when interpreting these results due to the limited number of studies and potential methodological and clinical heterogeneity. The specific results are as follows: the combined effect size for RA knowledge was 0.46 (95% CI: −0.14, 1.07, I^2^ = 75.98%, P = 0.133) (Fig 5); the combined effect size for functional level was −0.30 (95% CI: [−0.54, −0.06], I^2^ = 0.0%, P = 0.014) (Fig 6); the combined effect size for self-management was 0.11 (95% CI: [−0.17, 0.39], P = 0.451) (Fig 7); and the combined effect size for self-efficacy was 0.12 (95% CI: [−0.12, 0.35], I^2^ = 0.0%, P = 0.340) (Fig 8).
Forest plots of RA knowledge.
Forest plots of functional level.
Forest plots of self-management.
Forest plots of self-efficacy.
Adverse events
Adverse events were reported in four studies. Three studies noted adverse events unrelated to the intervention [19,34,44]. For example, one study reported muscle pain due to increased physical activity after initiating the intervention. Falls were also reported but were deemed unrelated to the intervention [19]. Another report mentioned that participants experienced disease-related pain episodes during the follow-up period [44]. Notably, one study recorded serious adverse events, including one death in the intervention group. The most prevalent serious adverse event in the control group was infection (n = 5), whereas only one case of infection was reported in the intervention group [32].
Discussion
This systematic review and meta-analysis of 18 RCTs assessed the effectiveness of smart healthcare interventions for adults with RA, focusing on disease activity, self-efficacy, functional capacity, RA knowledge, self-management, and qualitative adverse events. Our findings reveal that smart healthcare interventions significantly reduce DAS28, enhance EQ-5D index values, and improve functional capacity, thereby elevating the quality of life for patients with RA. However, no statistically significant differences were observed in other outcome measures.
The methodological assessment revealed several issues requiring careful consideration. A primary concern was the inadequate reporting of allocation concealment procedures in multiple studies, resulting in uncertain risk of selection bias. Furthermore, nine studies demonstrated high risk of bias in blinding of participants and personnel – an inherent methodological challenge associated with the remote nature of digital interventions. Maintaining adequate blinding of participants, healthcare providers, and outcome assessors in digital health trials poses significant challenges, potentially compromising methodological rigor and leading to overestimation of treatment effects. Additionally, the limited number of available studies for certain outcome measures prevented us from conducting sensitivity analyses, thereby constraining the assessment of result robustness.
The analysis demonstrated substantial heterogeneity across multiple dimensions of the included interventions. The studies employed varied technological platforms (including mobile applications, teleconsultation systems, and web-based platforms), with differences in intervention types, implementation approaches, and follow-up durations (ranging from 3 to 12 months). While this diversity reflects the dynamic evolution of digital health technologies, it limited our ability to identify specific active components through subgroup analyses. Variations in outcome measurement instruments across studies (for instance, in RA knowledge assessment) further complicated cross-study comparisons [29,43]. The insufficient number of studies focusing on similar intervention components hindered meaningful subgroup analyses, highlighting the urgent need for standardized intervention frameworks and reporting guidelines in future trials.
An important finding relates to the demographic characteristics of the study populations. The average age of participants in most included studies exceeded 50 years, substantially limiting the generalizability of the findings. This age distribution may not adequately represent younger RA populations, who typically demonstrate different levels of digital literacy, technology usage patterns, communication preferences, and disease management needs. The effectiveness, engagement patterns, and implementation requirements of digital health interventions may differ significantly across age groups, indicating that current findings should be applied with particular caution to younger patient populations.
In contrast to previous meta-analyses that often combined different measurement instruments, our analytical approach involved separate evaluation of distinct measurement tools. We individually analyzed DAS28, DAS28-CRP, DAS28-ESR, CDAI, and RADAI for disease activity assessment, and independently evaluated EQ-5D and RAND-36 for quality of life measurement. This methodological refinement contributed to reduced clinical heterogeneity and enhanced the validity and reliability of our findings. However, the consistent underreporting of adverse events across the majority of studies represents a significant evidence gap that requires urgent attention in future digital health research.
Conclusion
This systematic review indicates that digitally delivered healthcare interventions can improve key clinical outcomes in patients with RA, including disease activity, functional capacity, and quality of life. However, important limitations – including methodological weaknesses in the original studies, substantial clinical heterogeneity, and demographic considerations – necessitate cautious interpretation of the results and restrict their generalizability to younger populations. Future research should focus on establishing RA-specific standardized digital health frameworks; developing core outcome sets that incorporate both RA characteristics and digital health dimensions; conducting methodologically rigorous trials with appropriate blinding procedures; and performing stratified analyses to identify the most effective intervention components suitable for different age groups and patient characteristics. Particularly crucial is the implementation of large-scale randomized controlled trials that evaluate long-term efficacy, cost-effectiveness, and implementation strategies, while fully considering patient-specific factors such as digital literacy, technology access, and age-related characteristics.
Supporting information
S1 FileSearch strategy.(DOCX)
S2 FileCharacteristics of Smart Healthcare Interventions.(DOCX)
S3 FileInclusion and Exclusion Criteria.(DOCX)
S4 FileReferences of studies excluded based on full text.(XLS)
S5 FileRisk of bias by RCT.(DOCX)
S6 FilePRISMA Checklist.(DOCX)
S7 FilePRISMA_2020_checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Di Matteo A, Bathon JM, Emery P. Rheumatoid arthritis. Lancet. 2023;402(10416):2019–33. doi: 10.1016/S 0140-6736(23)01525-8 38240831 · doi ↗ · pubmed ↗
- 2Finckh A, Gilbert B, Hodkinson B, Bae S-C, Thomas R, Deane KD, et al. Global epidemiology of rheumatoid arthritis. Nat Rev Rheumatol. 2022;18(10):591–602. doi: 10.1038/s 41584-022-00827-y 36068354 · doi ↗ · pubmed ↗
- 3Gravallese EM, Firestein GS. Rheumatoid Arthritis - Common Origins, Divergent Mechanisms. N Engl J Med. 2023;388(6):529–42.36780677 10.1056/NEJ Mra 2103726 · doi ↗ · pubmed ↗
- 4Song Y, Li J, Wu Y. Evolving understanding of autoimmune mechanisms and new therapeutic strategies of autoimmune disorders. Signal Transduct Target Ther. 2024;9(1):263. doi: 10.1038/s 41392-024-01952-8 39362875 PMC 11452214 · doi ↗ · pubmed ↗
- 5Safiri S, Kolahi AA, Hoy D, Smith E, Bettampadi D, Mansournia MA, et al. Global, regional and national burden of rheumatoid arthritis 1990-2017: a systematic analysis of the Global Burden of Disease study 2017. Ann Rheum Dis. 2019;78(11):1463–71. doi: 10.1136/annrheumdis-2019-215920 31511227 · doi ↗ · pubmed ↗
- 6Castillo-Cañón JC, Trujillo-Cáceres SJ, Bautista-Molano W, Valbuena-García AM, Fernández-Ávila DG, Acuña-Merchán L. Rheumatoid arthritis in Colombia: a clinical profile and prevalence from a national registry. Clin Rheumatol. 2021;40(9):3565–73. doi: 10.1007/s 10067-021-05710-x 33772350 · doi ↗ · pubmed ↗
- 7Galarza-Delgado DA, Azpiri-Lopez JR, Colunga-Pedraza IJ, Cárdenas-de la Garza JA, Vera-Pineda R, Wah-Suárez M, et al. Prevalence of comorbidities in Mexican mestizo patients with rheumatoid arthritis. Rheumatol Int. 2017;37(9):1507–11. doi: 10.1007/s 00296-017-3769-3 28681250 · doi ↗ · pubmed ↗
- 8Barragán-Martínez C, Amaya-Amaya J, Pineda-Tamayo R, Mantilla RD, Castellanos-de la Hoz J, Bernal-Macías S, et al. Gender differences in Latin-American patients with rheumatoid arthritis. Gend Med. 2012;9(6):490-510.e 5. doi: 10.1016/j.genm.2012.10.005 23217568 · doi ↗ · pubmed ↗