Pancreatic Schistosomiasis, China, 2020–2024
Long He, Chuanbing Zhao, Yu Lu, Hongzhen Wei, Zanglong Deng, Yunpeng Zhang, Tao Yin

TL;DR
This paper reports four rare cases of pancreatic schistosomiasis in China and highlights the difficulty in diagnosing this condition.
Contribution
The paper presents the first reported cases of pancreatic schistosomiasis in China, emphasizing its rarity and diagnostic challenges.
Findings
Pancreatic schistosomiasis is extremely rare and poses significant diagnostic difficulties.
Four cases of pancreatic schistosomiasis were identified in endemic regions of China.
The potential association between schistosomiasis and pancreatic cancer requires further investigation.
Abstract
Schistosomiasis is a globally prevalent parasitic infection, but pancreatic involvement is extremely rare. In this article, we report 4 cases of pancreatic schistosomiasis from endemic regions in China. The possible link between schistosomiasis and pancreatic malignancy deserves further study. These cases underscore the diagnostic challenge of pancreatic schistosomiasis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
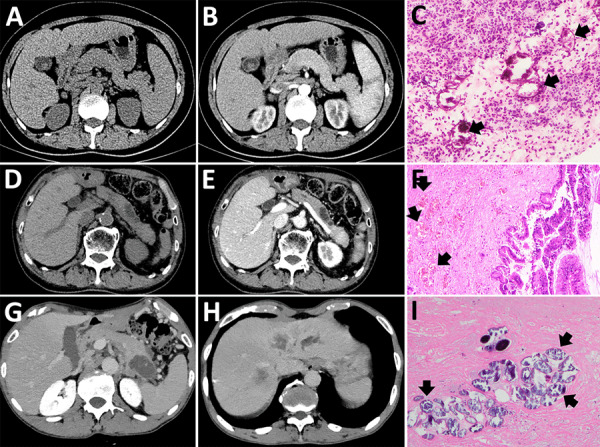 Figure 1
Figure 1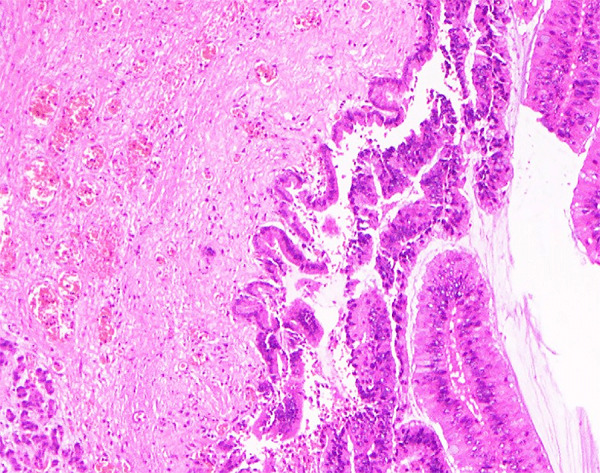 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Parasite Biology and Host Interactions · Amoebic Infections and Treatments
Schistosomiasis is a parasitic infection caused by trematodes of the genus Schistosoma (1). Globally, ≈1 billion people are at risk for schistosomiasis and there have been 250 million cases across 78 countries. By 2021, the disease accounted for >1.8 million disability-adjusted life years lost. Schistosoma infection is closely linked to impoverished living conditions (2).
The Schistosoma lifecycle requires an intermediate host, such as Biomphalaria, Bulinus, and Oncomelania snails, before infecting and causing disease in definitive hosts such as humans or other mammals (3). The main pathogenic species in humans are S. hematobium, S. japonicum, and S. mansoni. Although adult worms are relatively nonpathogenic, their eggs induce granulomatous inflammation characterized by eosinophilic and lymphocytic infiltration, leading to both acute and chronic disease (4).
The clinical manifestations of schistosomiasis are related to infection intensity and duration, and the intestines, liver, and bladder are the most involved organs (2). Early infection might manifest as cercarial dermatitis. Acute schistosomiasis is often asymptomatic, but sudden onset of fever, myalgia, fatigue, and abdominal pain lasting 2–10 weeks can occur. Chronic schistosomiasis is typically characterized by nonspecific, intermittent abdominal pain, diarrhea, and rectal bleeding (in S. mansoni and S. japonicum infections) or hematuria (in S. hematobium infection). In advanced chronic cases, complications such as portal hypertension (S. mansoni and S. japonicum) or hydronephrosis, renal failure, and bladder cancer (S. hematobium) can occur (2).
Emerging evidence suggests that schistosomiasis is a systemic disease that might also involve the spleen, heart, lungs, nervous system, and other organs (5–7). However, pancreatic involvement is exceedingly rare. In this article, we report 4 cases of schistosomiasis in China affecting the pancreas (Table). Informed consent was obtained from the patients for the publication of their information.
The Study
Patient 1 was a 49-year-old woman with a 1-year history of intermittent fever (up to 40°C) who was found to have a space-occupying lesion in the pancreatic head during routine examination in October 2020. She resided in Hubei, China, and had a history of untreated schistosomiasis. Computed tomography at Wuhan Union hospital revealed a 4.8 × 3.5 cm mass superior to the pancreatic head, involving the pancreas and associated with enlarged peripancreatic lymph nodes (Figure 1, panels A, B). Tumor markers were unremarkable, but hemoglobin was mildly reduced (93 g/L, reference range 115–150 g/L). To clarify the diagnosis, we conducted an endoscopic ultrasound-guided fine-needle aspiration of the pancreatic head. Pathology demonstrated fibrinous exudate and schistosome eggs (Figure 1, panel C). S. japonicum eggs were also found in the stool. The patient was diagnosed with pancreatic schistosomiasis and treated with a 1-day course of praziquantel (60 mg/kg in 3 doses). Two weeks later, her symptoms resolved, and she was discharged. No fever recurrence was observed at 3-month follow-up.
Imaging from 4 cases of pancreatic schistosomiasis, China, 2020–2024. A, B) Computed tomography (CT) images from patient 1 revealing a mass involving the pancreas. C) Pathologic examination from fine-needle aspiration of patient 1 showing fibrinous exudate and schistosome eggs (arrows). D, E) Abdominal CT of patient 2 showing a nonenhancing, tubular lesion adjacent to the main pancreatic duct in the body of the pancreas. F) Pathologic examination of sample from patient 2 showing intraductal papillary mucinous neoplasm with moderate dysplasia and scattered schistosome eggs (arrows). G, H) Abdominal CT of patient 3 revealing a low-density mass in the pancreatic tail and multiple ring-enhancing hepatic nodules. I) Pathologic examination of sample from patient 3 showing schistosome egg deposition (arrows) with associated tissue necrosis.
Patient 2 was a 73-year-old man who sought care in November 2024 with 1 day of abdominal pain. Six months prior, he had a history of pancreatitis. He also had a long-term residence in Hubei and a history of schistosomiasis without any treatment. Laboratory findings included hemoglobin 94 g/L (reference range 130–175 g/L) and serum amylase 522 U/L (reference range 20–125 U/L); tumor markers were unremarkable. S. japonicum eggs were detected in his stool. Abdominal computed tomography scan revealed a nonenhancing, tubular lesion adjacent to the main pancreatic duct in the body of the pancreas, suggesting possible intraductal papillary mucinous neoplasm (IPMN) and an enhancing nodule in the pancreatic tail, suspected to be a neuroendocrine tumor (Figure 1, panels D, E). After fluid replacement, analgesia, and resumption of oral intake, the abdominal pain resolved. We conducted a laparoscopic distal pancreatectomy. Pathology revealed IPMN with moderate dysplasia in parts of the glandular epithelium, and scattered schistosome eggs (Figure 1, panel F; Figure 2). We discharged the patient 2 weeks postoperatively and referred him to the infectious diseases department. He was treated with a 1-day course of praziquantel (60 mg/kg in 3 doses). At 3-month follow-up, he remained symptom-free.
Enlarged image of schistosome eggs in pancreas of patient 2 in report of 4 cases of pancreatic schistosomiasis, China, 2020–2024.
Patient 3 was a 65-year-old man who sought care in March 2022 with complaints of left upper abdominal pain lasting 1 month. He had a history of liver cirrhosis and untreated schistosomiasis. Hepatitis B surface antigen, e antigen, and core antibody were all positive. Tumor markers carcino-embryonic antigen, CA125, and CA19-9 were markedly elevated. Hemoglobin measured slightly low at 125 g/L (reference range 130–175 g/L). Contrast-enhanced abdominal computed tomography revealed a low-density mass in the pancreatic tail, highly suggestive of pancreatic cancer, and multiple ring-enhancing hepatic nodules suggestive of metastases (Figure 1, panels G, H). Endoscopic ultrasound-guided biopsy yielded 2 tissue samples: 1 sample showed schistosome egg deposition with tissue necrosis, and the other sample revealed pancreatic carcinoma cells (Figure 1, panel I). We diagnosed the patient with pancreatic schistosomiasis and pancreatic ductal adenocarcinoma with liver metastases. We transferred him to the oncology department for further management. Four months later, follow-up revealed the patient had died.
We published the case of patient 4 last year (8). In brief, a 47-year-old man who had had intermittent left upper quadrant abdominal pain for 5 years was found to have a hypodense cystic lesion in the tail of the pancreas on imaging. He subsequently underwent surgery, and the resected specimen’s pathology confirmed pancreatic and splenic schistosomiasis. Splenic schistosomiasis was documented previously (9).
Conclusions
During the past 70 years, China has made remarkable progress in controlling schistosomiasis (caused by S. japonicum), resulting in a 99% reduction in prevalence. China is steadily progressing toward the goal of complete schistosomiasis elimination (10). However, sporadic cases of schistosomal infection continue to occur in endemic areas such as Hunan, Jiangxi, and Hubei.
Pancreatic schistosomiasis is extremely rare, and we found only 1 known previous report of chronic pancreatitis caused by S. mansoni (11). Animal studies have shown that schistosome eggs can be deposited in pancreatic tissue (12). All 4 patients described in this article lived in endemic areas and had a history of schistosomiasis. Their main symptoms were intermittent abdominal pain and fever, and imaging consistently indicated pancreatic space-occupying lesions that posed diagnostic challenges. Two cases were ultimately diagnosed as inflammatory lesions, 1 as IPMN, and 1 as pancreatic ductal adenocarcinoma with hepatic metastases. Pathology confirmed S. japonicum egg deposition in all 4 cases.
Egg deposition in the pancreas induces granuloma formation and chronic inflammation. Of note, in case 3, pancreatic cancer cells and liver metastasis were found at the lesion site. Associations between schistosomiasis and colorectal, liver, and bladder cancers have been previously published (13–15). Furthermore, schistosome egg deposition in colorectal cancer is linked to a higher rate of the KRAS G12D mutation, which is also a key driver mutation in pancreatic cancer. Therefore, the pancreatic cancer in case 3 might be related to schistosomal infection, rather than being coincidental.
Once pancreatic schistosomiasis is confirmed, praziquantel remains the primary treatment. In this article, patient 1 improved with praziquantel therapy; patients 2 and 4 underwent surgery because of the high suspicion of malignancy and were treated with praziquantel after the diagnosis of pancreatic schistosomiasis; and patient 3 primarily received chemotherapy but died because of advanced disease.
Schistosomiasis involving the pancreas is exceedingly rare and manifests with nonspecific symptoms, making diagnosis challenging. In endemic areas, particularly in patients with a history of schistosomiasis who are found to have pancreatic lesions, pancreatic schistosomiasis should be considered as part of a differential diagnosis. In addition, there is evidence of a potential association between Schistosoma infection and pancreatic cancer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Colley DG, Bustinduy AL, Secor WE, King CH. Human schistosomiasis. Lancet. 2014;383:2253–64. 10.1016/S 0140-6736(13)61949-224698483 PMC 4672382 · doi ↗ · pubmed ↗
- 2Buonfrate D, Ferrari TCA, Adegnika AA, Russell Stothard J, Gobbi FG. Human schistosomiasis. Lancet. 2025;405:658–70. 10.1016/S 0140-6736(24)02814-939986748 · doi ↗ · pubmed ↗
- 3Wilson RA. Schistosomiasis then and now: what has changed in the last 100 years? Parasitology. 2020;147:507–15. 10.1017/S 003118202000004931965953 PMC 10317683 · doi ↗ · pubmed ↗
- 4Gobbi F, Tamarozzi F, Buonfrate D, van Lieshout L, Bisoffi Z, Bottieau E; Trop Net Schisto Task Force. Trop Net Schisto Task Force. New insights on acute and chronic schistosomiasis: do we need a redefinition? Trends Parasitol. 2020;36:660–7. 10.1016/j.pt.2020.05.00932505540 · doi ↗ · pubmed ↗
- 5Lambertucci JR. Acute schistosomiasis mansoni: revisited and reconsidered. Mem Inst Oswaldo Cruz. 2010;105:422–35. 10.1590/s 0074-0276201000040001220721485 · doi ↗ · pubmed ↗
- 6Ferrari TC, Moreira PR. Neuroschistosomiasis: clinical symptoms and pathogenesis. Lancet Neurol. 2011;10:853–64. 10.1016/S 1474-4422(11)70170-321849166 · doi ↗ · pubmed ↗
- 7Gobbi F, Buonfrate D, Angheben A, Beltrame A, Bassetti M, Bertolaccini L, et al. Pulmonary nodules in African migrants caused by chronic schistosomiasis. Lancet Infect Dis. 2017;17:e 159–65. 10.1016/S 1473-3099(16)30530-828214126 · doi ↗ · pubmed ↗
- 8He L, Lu Y, Hu X, Yin T. Schistosomal pancreatitis mimicking pancreatic neoplasm. Dig Liver Dis. 2025;57:342–3. 10.1016/j.dld.2024.10.02039523196 · doi ↗ · pubmed ↗