Metatranscriptomic Identification of Trubanaman Virus Sequences in Patient with Encephalitis, Australia
Krispin Hajkowicz, John Woodford, Elango Subramonia Pillai, Andrea Henden, Kym Lowry, Mary E. Petrone, Patrick N.A. Harris, Edward C. Holmes

TL;DR
Trubanaman virus was found in a patient with fatal encephalitis in Australia, suggesting it may be a new cause of this disease.
Contribution
First report of Trubanaman virus associated with human encephalitis.
Findings
Trubanaman virus sequences were identified in cerebrospinal fluid from a fatal encephalitis case.
The virus is related to orthobunyaviruses previously found in Australian mosquitoes.
No other causes were detected, implicating Trubanaman virus as the likely pathogen.
Abstract
Using metatranscriptomics, we identified Trubanaman virus in cerebrospinal fluid from a severely immunocompromised man who died of encephalitis in Queensland, Australia. Virus sequences were related to orthobunyaviruses previously detected in mosquitoes in Australia. Testing for other causes yielded negative results, suggesting that Trubanaman virus was the cause of this fatal encephalitis case.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
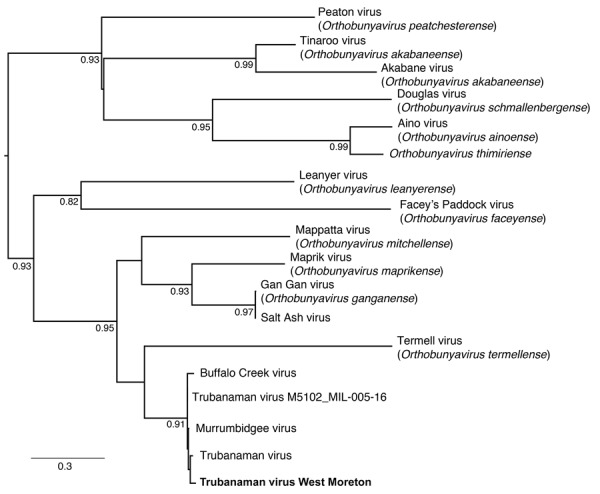 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Vectors · Mosquito-borne diseases and control · Vector-Borne Animal Diseases
Approximately 50% of global encephalitis cases remain undiagnosed by conventional testing (1). Metagenomic next-generation sequencing (mNGS), particularly metatranscriptomics (i.e., total RNA sequencing), is an emerging approach to infection diagnosis that reveals all nucleic acid in a sample, making it ideal for detecting novel and emerging pathogens (2).
Orthobunyavirus (order Bunyavirales) is a diverse genus of negative-sense single-stranded RNA viruses recognized to cause febrile illness and encephalitis in humans globally (3). The best described orthobunyaviruses are La Crosse virus and Jamestown Canyon virus, both of which rarely cause encephalitis, permanent neurologic sequalae, or death (4,5). Jamestown Canyon virus is associated with meningoencephalitis in immunocompromised persons (5), whereas the emerging Oropuche virus is associated with fever, headache, myalgias, and rare cases of meningoencephalitis and has recently expanded its range in Central and South America (6). We used metatranscriptomics to investigate a case of encephalitis in an immunocompromised person in Australia.
The study was approved by the Metro-North Health Human Research Ethics Committee and written informed consent was obtained from the patient and his next of kin. Metatranscriptomic sequencing and analysis methods are detailed (Appendix).
A man in his 50s who lived in West Moreton, Queensland, Australia, was admitted for a volunteer unrelated donor allogeneic hemopoietic stem cell transplantation with posttransplant cyclophosphamide and tacrolimus for B-cell acute lymphoblastic leukemia in complete remission one. There was no central nervous system involvement. He received 8 cycles of rituximab-hyper cyclophosphamide, vincristine, doxorubicin, and dexamethasone before transplantation. The transplant was complicated by a polymicrobial bloodstream infection that was successfully treated with intravenous daptomycin, as well as mucositis and diarrhea.
On day 18 after the hemopoietic stem cell transplantation, the patient experienced fever to 38.8°C, tachycardia to 10^9^ beats/min, muscular pain, intermittent headache, and confusion manifesting as slow and tangential answers to questions, difficulty word-finding, reduced oral intake, disorientation to time and place, and delusions such as thinking that he had been in a car accident. The onset coincided with recovery of his neutrophil and lymphocyte count. His confusion fluctuated but generally deteriorated. Twenty-two days later, a cerebrospinal fluid (CSF) examination was performed (Table). Magnetic resonance imaging (MRI) of the brain was also performed, and results were unremarkable. However, results of an electroencephalograph were abnormal, showing mild, diffuse cortical dysfunction but no epileptiform activity. Results of a nasopharyngeal nucleic acid amplification test (NAAT) were positive for rhinovirus. Stool, blood, and urine culture and NAAT results were negative for viruses, bacteria, and fungi (Table). He was unresponsive to corticosteroids, and during the next few months, his level of consciousness, function, and speech declined; serial MRIs showed progressive cerebral atrophy. He died 6 months after the onset of confusion.
Metatranscriptomic sequencing of the patient’s CSF using NovaSeq (Illumina, https://www.illumina.com) generated a total of 57,452,775 paired reads, of which 74 matched the M glycoprotein precursor of Trubanaman, Murrumbidgee, and Buffalo Creek viruses (i.e., the Mapputta group, which likely represents a single species within the genus Orthobunyavirus). E-values were <10^−116^. From some of those reads, we assembled a single contig of 270 bp (GenBank accession no. PV702715), denoted Trubanaman virus West Moreton (Figure). We did not recover reads from the RNA-dependent RNA polymerase (RdRp) or other virus genes. The water control was negative for bunyaviruses. Similarly, metatranscriptomic analysis was negative for other known or putative human pathogenic viruses, bacteria, fungi, and parasites, and no other candidate pathogens were identified.
Using metatranscriptomics, we identified Trubanaman virus sequences in a CSF sample from a person with encephalitis. Extensive testing for other infectious, autoimmune, and malignant causes yielded negative results. In the context of a high-risk immunocompromised person with typical clinical manifestations of encephalitis, our findings support, but do not confirm, that Trubanaman virus was the cause of the patient’s encephalitis. PCR could not be performed on the original sample because it was fully depleted for conventional testing and sequencing, although no viable routes to sample contamination existed. Follow-up testing of CSF collected 6 weeks later was negative by both metatranscriptomics and orthobunyavirus-specific PCRs targeting the N protein and RdRp.
Trubanaman and related viruses have been detected in mosquito populations throughout Australia (7). Patients with a suspected arthropodborne virus infection in New South Wales exhibited neutralizing antibody prevalences of 4.7% to Gan Gan virus (GGV) and 1.4% to Trubanaman virus (8). GGV was associated with an acute febrile illness and polyarthritis in 3 persons in Australia who had significant titer rises in paired serum samples, as well as GGV-specific IgM (9). In addition, serologic evidence suggests that kangaroos, feral animals, and domestic horses are reservoirs for orthobunyaviruses in Australia (9). Of note, 2 bunyavirus-associated cases of fatal meningoencephalitis in immunocompromised persons were recently described in the United States using CSF mNGS (10). Further research is required to establish the pathogenic role of Trubanaman virus as a cause of encephalitis in Australia and to determine the arthropod vectors, zoonotic reservoirs, and seroprevalence. However, our findings suggest that Trubanaman virus was the cause of this fatal encephalitis case, and clinicians should be aware of the possibility of infection with this virus in similar cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schubert RD, Wilson MR. A tale of two approaches: how metagenomics and proteomics are shaping the future of encephalitis diagnostics. Curr Opin Neurol. 2015;28:283–7.25923127 10.1097/WCO.0000000000000198 PMC 4418212 · doi ↗ · pubmed ↗
- 2Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20:341–55.30918369 10.1038/s 41576-019-0113-7PMC 6858796 · doi ↗ · pubmed ↗
- 3Elliott RM. Orthobunyaviruses: recent genetic and structural insights. Nat Rev Microbiol. 2014;12:673–85.25198140 10.1038/nrmicro 3332 · doi ↗ · pubmed ↗
- 4Haddow AD, Odoi A. The incidence risk, clustering, and clinical presentation of La Crosse virus infections in the eastern United States, 2003-2007. P Lo S One. 2009;4:e 6145.19582158 10.1371/journal.pone.0006145 PMC 2702082 · doi ↗ · pubmed ↗
- 5Meier-Stephenson V, Drebot MA, Dimitrova K, Di Quinzio M, Fonseca K, Forrest D, et al. Case series of Jamestown Canyon virus infections with neurologic outcomes, Canada, 2011–2016. Emerg Infect Dis. 2024;30:874–81.38666581 10.3201/eid 3005.221258 PMC 11060468 · doi ↗ · pubmed ↗
- 6Riccò M, Corrado S, Bottazzoli M, Marchesi F, Gili R, Bianchi FP, et al. (Re-)emergence of Oropouche virus (OROV) infections: systematic review and meta-analysis of observational studies. Viruses. 2024;16:1498.39339974 10.3390/v 16091498 PMC 11437499 · doi ↗ · pubmed ↗
- 7Gauci PJ, Mc Allister J, Mitchell IR, Weir RP, Melville LF, Gubala AJ. Genomic characterisation of Trubanaman and Gan Gan viruses, two bunyaviruses with potential significance to public health in Australia. Virol Rep. 2016;6:1–10.
- 8Boughton CR, Hawkes RA, Naim HM. Arbovirus infection in humans in NSW: seroprevalence and pathogenicity of certain Australian bunyaviruses. Aust N Z J Med. 1990;20:51–5.2108660 10.1111/j.1445-5994.1990.tb 00371.x · doi ↗ · pubmed ↗