Recurrent Self‐Limiting Acute Pancreatitis: Intraductal Papillary Mucinous Neoplasm Requiring Surgery
Chia‐Hsin Chang, Yu‐Chun Ma, Shih‐Chang Chuang, Chih‐Wen Wang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
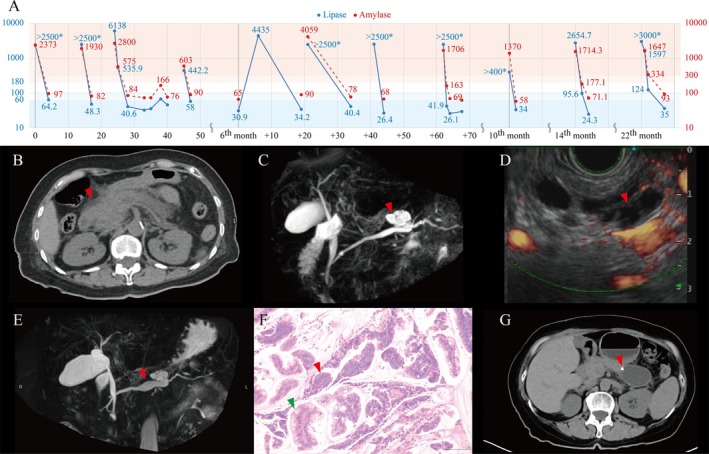 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Pancreatitis Pathology and Treatment · Gastrointestinal disorders and treatments
A 70‐year‐old woman with Type 2 diabetes mellitus who denied alcohol or tobacco use presented with mild, dull epigastric pain. The pain was relieved by the knee‐chest position and accompanied by nausea and vomiting, and she visited our emergency department after each episode. Significant increases in amylase (up to 4059 IU/L) and lipase (up to 6138 IU/L) levels recorded during over 10 visits for episodes of acute pancreatitis (Figure 1A). Interestingly, both amylase and lipase levels returned to normal within 2 days after each episode without any complications, and her epigastric pain improved spontaneously. She was subsequently discharged without issues.
Computed tomography (CT) during the first episode of pancreatitis revealed pancreatic swelling with localized infiltration (Figure 1B). One month after the initial presentation, magnetic resonance cholangiopancreatography (MRCP) showed a cystic neoplasm in the pancreatic body connected to the main pancreatic duct (Figure 1C). Endoscopic ultrasonography (Figure 1D) with a through‐the‐needle biopsy from the stomach was performed in the 10th month, which revealed cystic lesions in the pancreatic body and elevated cystic carcinoembryonic antigen level, but no signs of malignancy. The procedure was complicated by acute pancreatitis, which resolved spontaneously within 2 days. CT and MRCP in the 14th month showed an enlarging cyst and dilation of the main pancreatic duct (Figure 1E). A surgical intervention was ultimately considered necessary, and laparoscopic subtotal pancreatectomy was performed in the 23rd month. Immunohistochemical staining of the specimen revealed both intestinal and pancreato‐biliary type epithelium. A pathological examination confirmed intraductal papillary mucinous neoplasm (IPMN) with low‐grade dysplasia (Figure 1F). Postoperative recovery was complicated by a grade A pancreatic fistula (Figure 1G), which was managed with retained drainage. Her condition gradually improved, and as of 2 years post‐surgery she has not experienced any further acute pancreatitis attacks.
In patients with acute pancreatitis, an abdominal examination may reveal Grey–Turner's sign or Cullen's sign in severe cases indicating retroperitoneal hemorrhage, while guarding or rebound tenderness may be present in more advanced cases such as necrotizing pancreatitis or secondary peritonitis. The differential diagnosis of acute pancreatitis is extensive and should be approached systematically, encompassing pancreatic, biliary, gastrointestinal, hepatic, cardiovascular, metabolic, toxic, infectious, and miscellaneous causes.
Guidelines vary in their threshold for recommending surgery [1]. The International Association of Pancreatology (IAP) [2] and European [3] guidelines adopt a more aggressive stance, considering that even small enhancing nodules (< 5 mm) are potential indicators for resection. The American College of Gastroenterology (ACG) [4] and European [3] guidelines also incorporate biomarkers such as elevated CA 19‐9 levels and new‐onset diabetes into their risk stratification. In contrast, the American Gastroenterological Association (AGA) 2015 [5] guidelines take a more conservative approach, recommending a surgical intervention only when multiple high‐risk features are present.
Our patient met multiple AGA [5], IAP [2], and European [3] guideline criteria for surgical resection of IPMN, including cyst size > 3 cm, main pancreatic duct dilation > 10 mm, progressive cyst growth, and recurrent pancreatitis. The decision to operate was clinically sound and evidence‐based, especially considering the risk of malignant transformation in mixed‐type IPMN. This case also contributes to a growing body of evidence that while IPMN‐related pancreatitis is often mild, it is an important indication for surgery.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1T. B. Gardner , W. G. Park , and P. J. Allen , “Diagnosis and Management of Pancreatic Cysts,” Gastroenterology 167, no. 3 (2024): 454–468.38442782 10.1053/j.gastro.2024.02.041 · doi ↗ · pubmed ↗
- 2M. Tanaka , C. Fernandez‐Del Castillo , T. Kamisawa , et al., “Revisions of International Consensus Fukuoka Guidelines for the Management of IPMN of the Pancreas,” Pancreatology 17, no. 5 (2017): 738–753.28735806 10.1016/j.pan.2017.07.007 · doi ↗ · pubmed ↗
- 3European Study Group on Cystic Tumours of the Pancreas , “European Evidence‐Based Guidelines on Pancreatic Cystic Neoplasms,” Gut 67, no. 5 (2018): 789–804.29574408 10.1136/gutjnl-2018-316027 PMC 5890653 · doi ↗ · pubmed ↗
- 4S. Tenner , S. S. Vege , S. G. Sheth , et al., “American College of Gastroenterology Guidelines: Management of Acute Pancreatitis,” American Journal of Gastroenterology 119, no. 3 (2024): 419–437.38857482 10.14309/ajg.0000000000002645 · doi ↗ · pubmed ↗
- 5S. S. Vege , B. Ziring , R. Jain , P. Moayyedi , Clinical Guidelines Committee , and American Gastroenterology Association , “American Gastroenterological Association Institute Guideline on the Diagnosis and Management of Asymptomatic Neoplastic Pancreatic Cysts,” Gastroenterology 148, no. 4 (2015): 819–822; quize 12‐3.25805375 10.1053/j.gastro.2015.01.015 · doi ↗ · pubmed ↗