Cardiac Arrest Secondary to Hypercapnia in an Obese Patient: A Case of Unresponsiveness With Preserved Awareness
Kajal S Shah, Ibtesam A Bhatti, Hinzilah S Minhas, Sunho Judy Lee, Hassan Jafary

TL;DR
A 58-year-old obese woman with sleep apnea experienced cardiac arrest due to high carbon dioxide levels, showing awareness during the event and highlighting the need for vigilance in similar cases.
Contribution
This case highlights the rare occurrence of hypercapnia-induced cardiac arrest with preserved awareness in obese patients with obstructive sleep apnea.
Findings
The patient showed awareness during a cardiac arrest episode despite being unresponsive.
Hypercapnia was identified as a trigger for the cardiac event through arterial blood gas analysis.
Bilevel positive airway pressure therapy improved the patient's clinical condition.
Abstract
In rare circumstances, hypercapnia can precipitate life-threatening cardiac events, particularly in patients with obesity hypoventilation syndrome and obstructive sleep apnea (OSA). Awareness during such episodes of unresponsiveness is uncommon, underscoring the complex interaction between respiratory and neurologic physiology. A 58-year-old Caucasian female with a body mass index of 37.4 kg/m², OSA, and a history of recurrent syncope presented to the emergency room with chest pain and shortness of breath. During hospitalization, she received sublingual nitroglycerin, after which she developed bradycardia and was administered atropine. She subsequently progressed into ventricular tachycardia and required two defibrillations to restore sinus rhythm. Remarkably, during resuscitation, she reported awareness despite unresponsiveness, hearing staff, and feeling defibrillation shocks. A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
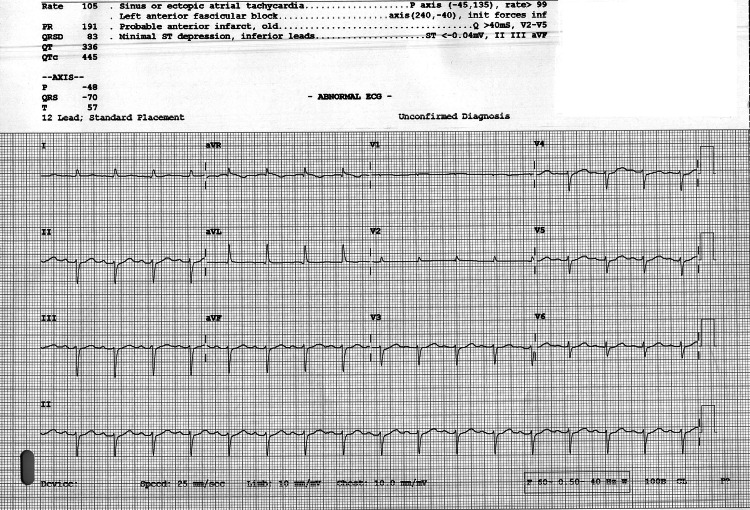 Figure 1
Figure 1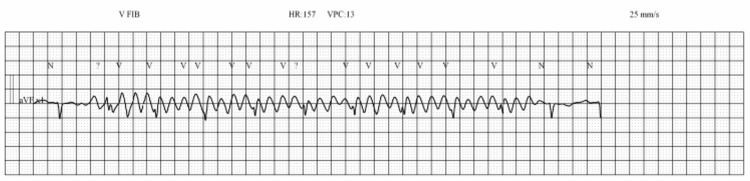 Figure 2
Figure 2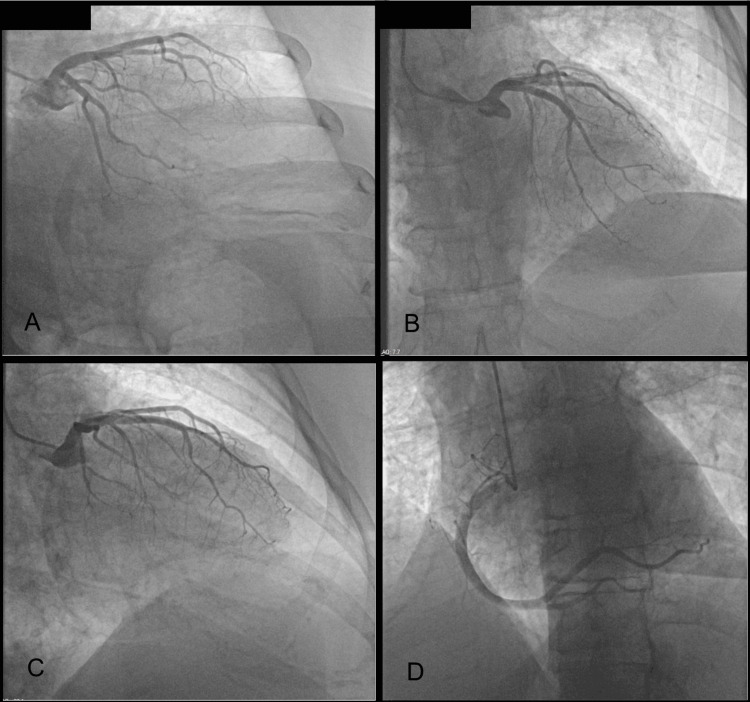 Figure 3
Figure 3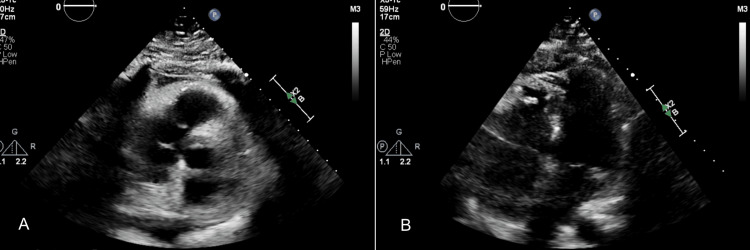 Figure 4
Figure 4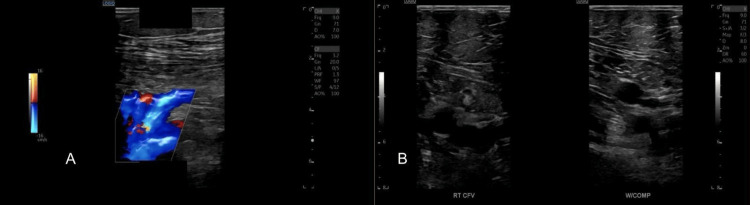 Figure 5
Figure 5| Laboratory test | Result | Reference range | Units |
| WBC | 7.51 | 4.0–9.7 | ×103/µL |
| Hemoglobin | 13.2 | 12.0–16.0 | g/dL |
| Platelet count | 240 | 182–369 | ×103/µL |
| Sodium | 139 | 136–145 | mmol/L |
| Potassium | 4.6 | 3.5–5.1 | mmol/L |
| BUN | 12 | 9–23 | mg/dL |
| Creatinine | 0.76 | 0.55–1.02 | mg/dL |
| GFR | >90 | >90 | mL/minute/1.73m3 |
| Glucose | 215 | 74–106 | mg/dL |
| BNP | 83 | 0–125 | pg/mL |
| Troponin | Negative × 3 | Negative | pg/mL |
| LVEF | 60% | 55–70 | % |
| Parameter | Initial (T0) | Repeat (T1) | Next day (T2) | Nine days later (T3) | Reference range | Units |
| pH | 7.32 ↓ | 7.3 ↓ | 7.38 | 7.4 | 7.35–7.45 | - |
| PaCO2 | 60 ↑ | 58 ↑ | 56 ↑ | 53 ↑ | 35–45 | mmHg |
| PaO2 | 94 | 73 ↓ | 107 ↑ | 96 | 80–100 | mmHg |
| HCO3- | 30.9 ↑ | 28.5 ↑ | 33.1 ↑ | 32.8 ↑ | 22–26 | mEq/L |
| Total CO2 | 32.7 ↑ | 30.30 ↑ | 34.80 ↑ | 34.40 ↑ | 23–30 | mEq/L |
| O2 saturation | 97 | 93 ↓ | 98 ↑ | 98 | 95–100 | % |
| Base excess | +3 ↑ | – | +6 ↑ | +7 ↑ | -2 to +2 | mEq/L) |
| BiPAP | 5 | 10 | 10 | - | - | cmH2O |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObstructive Sleep Apnea Research · Cardiovascular and Diving-Related Complications · Neuroscience of respiration and sleep
Introduction
Obesity hypoventilation syndrome (OHS) is defined by the triad of obesity (body mass index (BMI) ≥30 kg/m²), chronic daytime hypercapnia (PaCO₂ >45 mmHg), and sleep-disordered breathing, most commonly obstructive sleep apnea (OSA) [1,2]. Excess adiposity imposes mechanical loads on the chest wall and blunts central ventilatory drive, predisposing patients to chronic carbon dioxide retention and recurrent episodes of acute-on-chronic hypercapnic respiratory failure [3].
Although hypercapnia is typically viewed as a marker of respiratory insufficiency, emerging evidence suggests that elevated PaCO₂ can have profound cardiovascular effects, including increased pulmonary vascular resistance, right ventricular strain, autonomic dysregulation, and arrhythmogenesis [4]. In patients with OHS and OSA (conditions already associated with sympathetic activation, endothelial dysfunction, and sudden cardiac death), acute hypercapnic decompensation creates a vulnerable milieu in which even modest derangements in ventilation may precipitate ventricular tachyarrhythmias or cardiac arrest [2,5].
A less recognized but clinically important phenomenon is preserved awareness during apparent unresponsiveness, in which patients retain auditory or tactile perception despite exhibiting outward unresponsiveness. Similar states have been described in peri-arrest physiology, syncope with transient cerebral hypoperfusion, and certain anesthetic awareness events, suggesting that cerebral cortical function may persist even when motor responsiveness is lost [6]. This phenomenon is rarely reported in the context of hypercapnia-induced cardiac instability and may lead clinicians to underestimate a patient’s perceptual awareness during resuscitative interventions.
We present the case of an obese woman with severe OSA who experienced a hypercapnia-related cardiac arrest and later described detailed awareness during a period of clinical unresponsiveness. This report underscores the importance of recognizing hypercapnia as a potential trigger for malignant arrhythmias in high-risk patients and highlights the need to consider preserved awareness during resuscitation, a feature that remains underreported in the literature.
Case presentation
A 58-year-old Caucasian woman presented to the emergency department complaining of chest pain and shortness of breath. Her medical history was significant for morbid obesity (BMI: 37.4 kg/m²), hyperlipidemia, cardiac muscle bridging, OSA, chronic respiratory failure, prior pulmonary embolism, coronary artery disease, and recurrent syncope. She described her chest pain as radiating to the left neck and left arm. At baseline, she required continuous supplemental oxygen at home as prescribed by her primary care physician.
Upon arrival, her vital signs were stable: blood pressure, 138/75 mmHg; pulse, 92 beats/minute; respiratory rate, 19 breaths/minute; and oxygen saturation, 97% on a nasal cannula. She rated the pain as 6/10 at the time of evaluation, reduced from 8/10 at presentation. Physical examination revealed no acute distress, and cardiac auscultation was unremarkable.
A 12-lead ECG (Figure 1) showed sinus or ectopic atrial tachycardia at 105 beats/minute, Q-waves in leads V2-V5 consistent with an old anterior infarct, and minimal ST-segment depression in the inferior leads (II, III, aVF). Relevant laboratory results are summarized in Table 1.
Twelve-lead ECG showing sinus or ectopic atrial tachycardia with Q waves in leads V2–V5 and minimal ST depression in the inferior leads.Twelve-lead ECG demonstrating sinus or ectopic atrial tachycardia at approximately 105 beats/minute, Q waves in leads V2–V5 consistent with an old anterior myocardial infarction, and minimal ST-segment depression in the inferior leads (II, III, aVF). Left anterior fascicular block is also noted. These findings suggested a prior anterior infarction but no evidence of acute ischemia contributing to the arrest.ECG = electrocardiogram; PR = PR interval; QRSD = QRS duration; QT = QT interval; QTC = corrected QT interval; P = P wave; QRST = ventricular depolarization complex; T = T wave; P-axis = atrial electrical axis; QRS-axis; ventricular electrical axis; T-axis = ventricular repolarization axis
During hospitalization, the patient developed recurrent chest pain without ST elevation but with non-specific ST-T abnormalities. She subsequently became bradycardic, received epinephrine, progressed to ventricular tachycardia, and required two external defibrillation shocks. Throughout these events, she remained alert and oriented. She was transferred to the intensive care unit (ICU) awake, with an oxygen saturation of 80-82% on a non-rebreather mask. Bilevel positive airway pressure (BiPAP) was initiated. An intravenous heparin infusion was started, and 80 mg of IV furosemide was administered for volume management. Arterial blood gas (ABG) analysis was performed (Table 2). She was scheduled for left-heart catheterization.
Later during the admission, she experienced severe recurrent chest pain, received sublingual nitroglycerin, and a code-blue event was activated. Cardiopulmonary resuscitation (CPR) was initiated, and atropine was administered for bradycardia. The rhythm evolved into ventricular tachycardia with a pulse (Figure 2), requiring two rounds of defibrillation. She subsequently regained sinus tachycardia with systolic blood pressures in the 160s and remained responsive. She was transferred back to the ICU without requiring intubation. Given the recurrence of ventricular arrhythmias, she was fitted with a LifeVest wearable cardioverter-defibrillator and referred to electrophysiology for evaluation for an implantable cardioverter-defibrillator.
Ventricular fibrillation requiring defibrillation.Cardiac rhythm strip demonstrating ventricular fibrillation characterized by rapid, irregular, and chaotic ventricular waveforms with no discernible P waves, QRS complexes, or T waves. The tracing reflects pulseless ventricular fibrillation at an approximate rate of 150–160 beats per minute. Immediate defibrillation was performed, and the patient subsequently regained sinus rhythm and hemodynamic stability. This rhythm explained the patient’s sudden collapse and the need for emergent defibrillation.ECG = electrocardiogram; HR = heart rate; V FIB = ventricular fibrillation; VPC = ventricular premature complex; BPM = beats per minute
Comprehensive cardiac evaluation, including left-heart catheterization, serial troponins, ECG, echocardiography, and laboratory testing, revealed non-obstructive coronary artery disease with probable small-vessel involvement. Coronary angiography demonstrated normal coronary flow without hemodynamically significant stenosis (Figure 3). Transthoracic echocardiography showed preserved left ventricular systolic function and no regional wall motion abnormalities (Figure 4).
Coronary angiography demonstrating non-obstructive coronary artery disease.(A–D) Sequential coronary angiographic projections showing normal coronary flow without hemodynamically significant stenosis. (A) Circumflex artery showing preserved patency and small-caliber distal segment without discrete narrowing. (B–C) Left anterior descending artery demonstrating mild non-obstructive myocardial bridging and a small-caliber distal segment. (D) Right coronary artery showing a dominant vessel with smooth contour and less than 40% stenosis of the right posterior descending artery. Collectively, these findings are consistent with non-obstructive coronary artery disease involving the small vessels, as reported on catheterization.
Transthoracic echocardiography demonstrating normal left ventricular function.(A–B) Standard transthoracic echocardiographic images showing preserved left ventricular systolic function. (A) Parasternal long-axis view demonstrating a normal-sized left ventricle with mild concentric hypertrophy, normal wall motion, and no regional wall motion abnormalities. (B) Apical four-chamber view showing normal chamber sizes, normal septal and lateral wall motion, and a left ventricular ejection fraction of ≈60%. A small pericardial effusion is present without evidence of tamponade. Valvular assessment shows mild aortic regurgitation and trace tricuspid regurgitation, with no hemodynamically significant stenosis. These findings confirm preserved global systolic function and support a diagnosis of small-vessel (microvascular) coronary disease rather than obstructive epicardial disease.
To further evaluate alternative causes of respiratory compromise, bilateral lower extremity venous Doppler ultrasonography was performed, demonstrating normal venous compressibility and flow without evidence of deep vein thrombosis (Figure 5). The patient remained hemodynamically stable and continued BiPAP therapy under pulmonology supervision for hypercapnia management. Post-catheterization vital signs included blood pressure of 155/78 mmHg, pulse of 98 beats/minute, respiratory rate of 24 breaths/minute, and oxygen saturation of 93% on 4 L nasal cannula.
Lower etremity venous Doppler ultrasound demonstrating normal flow and compressibility.(A) Color Doppler ultrasound demonstrating normal venous flow and patent lumen without evidence of thrombus. (B) B-mode compression ultrasonography of the right common femoral vein before and during compression, showing complete vein collapse with applied pressure, confirming normal venous patency.CFV = common femoral vein; COMP = compression
Neurology was consulted for intermittent slurred speech and chronic dysphagia. Prior swallow studies revealed no abnormalities requiring intervention or associated with an increased risk of aspiration. A 72-hour electroencephalograpy and CT head were negative for seizure activity or acute neurologic insult.
Several days after discharge, the patient experienced another syncopal episode at home and was found unresponsive with no awareness of her surroundings. On readmission, ABG analysis (Table 2) revealed significant hypercapnia, prompting initiation of BiPAP therapy, which led to clinical improvement. After stabilization, she was discharged on continuous positive airway pressure (CPAP) therapy for OSA, weight-management counseling, and follow-up with cardiology and pulmonology specialists.
Discussion
Hypercapnia is defined as an elevation of the arterial partial pressure of carbon dioxide (PaCO₂) above 45 mmHg. Carbon dioxide (CO₂), a metabolic byproduct of cellular respiration, is normally eliminated through diffusion across the alveolar-capillary membrane. When this process is impaired, CO₂ accumulates, resulting in respiratory acidosis.
Obesity is a major contributor to chronic hypercapnia. Excess adiposity alters respiratory mechanics by increasing chest wall load, reducing lung and chest wall compliance, and elevating airway resistance, all of which increase the work of breathing. These changes contribute to OHS, wherein impaired ventilatory drive and mechanical restriction lead to chronic CO₂ retention. Leptin resistance, common in obesity, further blunts central respiratory drive, exacerbating hypoventilation and hypercapnia [7]. As CO₂ levels rise, the respiratory system attempts to compensate through hyperventilation; however, this compensation may be insufficient, leading to persistent respiratory acidosis [8].
Chronic hypercapnia has significant cardiovascular consequences. Elevated CO₂ causes pulmonary vasoconstriction, increased pulmonary artery pressures, and right ventricular hypertrophy, eventually progressing to right-sided heart failure [9]. Acidosis impairs myocardial contractility, contributing to hypotension and reduced cerebral perfusion, which may manifest as syncope. Hypercapnia also triggers sympathetic activation, increasing myocardial oxygen demand and predisposing to malignant ventricular arrhythmias, consistent with our patient’s progression from bradycardia to ventricular tachycardia [3]. In individuals with OHS or OSA, autonomic dysregulation, endothelial dysfunction, and systemic inflammation amplify cardiovascular risk [9].
CO₂ narcosis represents another severe manifestation of hypercapnia, driven by cerebral vasodilation in response to elevated PaCO₂. Clinically, this can range from confusion and lethargy to coma. In our patient, significant hypercapnia, together with OHS and OSA, likely impaired cerebral perfusion and contributed to her syncopal episode [10].
Awareness during cardiac arrest is rare but clinically recognized. Transient cerebral perfusion during chest compressions or brief periods of spontaneous circulation may preserve partial consciousness even when systemic circulation is severely compromised [11]. Patients may appear unresponsive yet retain perceptual awareness or recall of resuscitative efforts. In this case, the patient’s awareness during defibrillation is most plausibly explained by intermittent restoration of cerebral blood flow sufficient to maintain consciousness despite ongoing cardiac instability [12].
This case underscores the importance of early recognition and prompt correction of hypercapnia in obese patients who present with unexplained respiratory or neurologic symptoms. Non-invasive ventilatory support, such as BiPAP, plays a central role in improving alveolar ventilation and reducing PaCO₂ [1]. In our patient, rapid initiation of BiPAP stabilized gas exchange and prevented further cardiovascular deterioration. Preventive strategies should prioritize optimization of OSA therapy, structured weight reduction interventions, and careful oxygen titration to avoid suppressing hypoxic ventilatory drive.
Conclusions
This case illustrates the complex interplay between obesity, hypoventilation, and cardiovascular instability. In individuals with OHS and OSA, acute CO₂ retention may precipitate hemodynamically significant ventricular tachyarrhythmias or cardiac arrest. The patient’s preserved awareness during apparent unresponsiveness highlights a rarely described phenomenon and expands the clinical understanding of perceptual experiences during peri-arrest states. Recognizing hypercapnia as a potential contributor to unexplained arrhythmias or syncope is essential, particularly in patients with severe obesity and sleep-disordered breathing. Early application of non-invasive ventilation, careful cardiac monitoring, and long-term weight management remain critical to preventing recurrence and improving patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Obesity Hypoventilation Syndrome Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls Publishing. Ghimire P Sankari A Antoine MH Bollu PC Kaul P Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 542216/
- 2Characteristics of obese patients with acute hypercapnia respiratory failure admitted in the Department of Pneumology: an observational study of a North African population Sleep Disord Msaad S Gargouri R Kotti A 5398460202220223522310310.1155/2022/5398460 PMC 8872695 · doi ↗ · pubmed ↗
- 3Hypercapnia in patients with acute heart failure ESC Heart Fail Konishi M Akiyama E Suzuki H 1219220152883464310.1002/ehf 2.12023 PMC 5746960 · doi ↗ · pubmed ↗
- 4Effects of mild hypercapnia on myocardial injury after out-of-hospital cardiac arrest. A sub-study of the TAME trial Resuscitation Melberg MB Flaa A Andersen GØ 11029520120243893665210.1016/j.resuscitation.2024.110295 · doi ↗ · pubmed ↗
- 5Cardiac arrest and mortality in OSA patient with morbid obesity Sleep Alawad S Alsaeed N Jarrar A Alyami B Sharma S 080482025
- 6Cardiovascular changes induced by targeted mild hypercapnia after out of hospital cardiac arrest. A sub-study of the TAME cardiac arrest trial Resuscitation Melberg MB Flaa A Andersen GØ 10997019320233771640110.1016/j.resuscitation.2023.109970 · doi ↗ · pubmed ↗
- 7Obesity hypoventilation syndrome Curr Pulmonol Rep Shetty S Parthasarathy S 4255420152602949710.1007/s 13665-015-0108-6PMC 4444067 · doi ↗ · pubmed ↗
- 8Respiratory Acidosis Curr Pulmonol Rep Patel S Sharma S 4255 Treasure Island, FL Stat Pearls Publishing 42023 https://www.ncbi.nlm.nih.gov/books/NBK 482430/29494037 · pubmed ↗