Transcatheter Mitral Valve Repair With MitraClip® in a Heart Transplant Recipient: Pushing the Limits of Percutaneous Valve Therapy
Pasquale Gagliardi, Marco Ferlini, Romina Frassica, Mauro Acquaro, Leonardo De Luca

TL;DR
A heart transplant patient successfully underwent a minimally invasive procedure to repair a leaky valve, showing this treatment can work even in complex cases.
Contribution
Demonstrates the feasibility of MitraClip® for mitral valve repair in heart transplant recipients.
Findings
Transcatheter mitral valve repair was successfully performed in a high-risk heart transplant patient.
Early follow-up showed a small left atrial thrombus that resolved with anticoagulation.
The procedure highlights the potential of percutaneous therapy in complex post-transplant valve disease.
Abstract
We report the case of a 62-year-old female who developed severe symptomatic functional mitral regurgitation (MR) 18 years after heart transplantation. Given her extremely high surgical risk, transcatheter edge-to-edge mitral valve repair with the MitraClip® device was selected as the most appropriate therapeutic option. The procedure was technically challenging due to altered post-transplant anatomy, but it was completed successfully without immediate complications and resulted in a substantial reduction in regurgitation. During early follow-up, a small left atrial thrombus was identified and subsequently resolved after a six-week course of oral anticoagulation. This report illustrates the feasibility and safety of transcatheter mitral repair in carefully selected heart transplant recipients and underscores the importance of tailored post-procedural surveillance in this complex…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
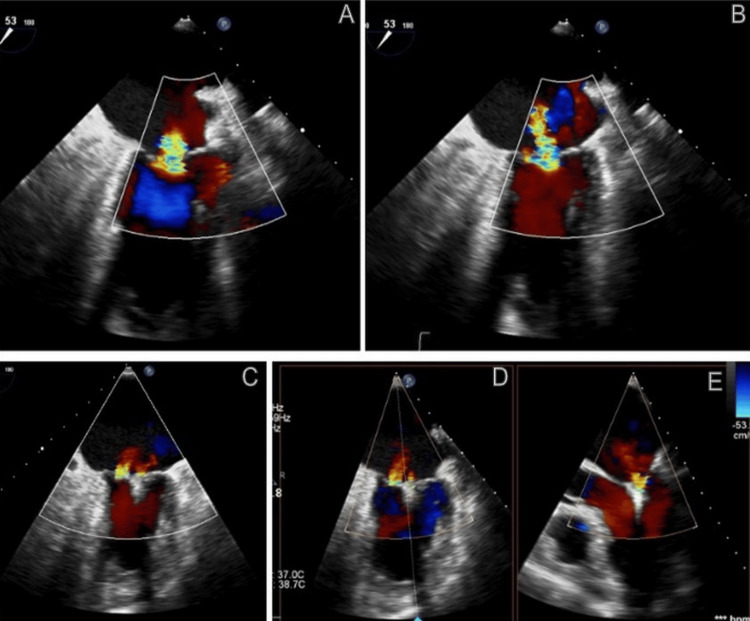 Figure 1
Figure 1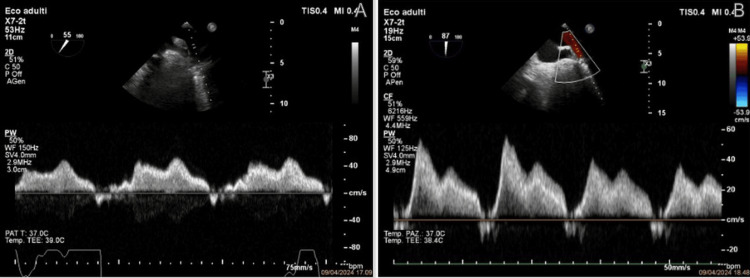 Figure 2
Figure 2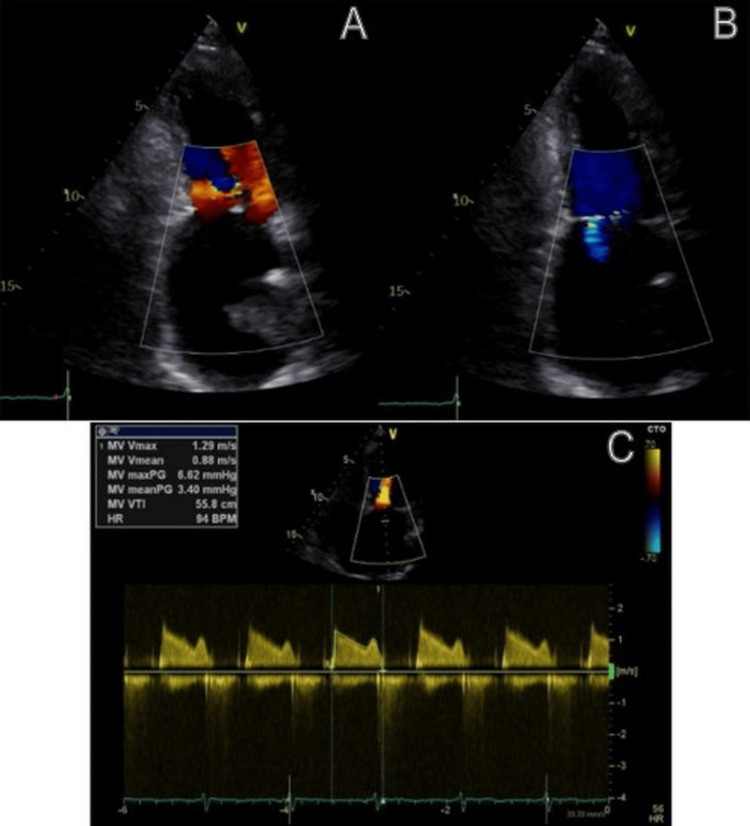 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Cardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management
Introduction
Mitral regurgitation (MR) in heart transplant recipients may result from annular dilation, graft dysfunction, or leaflet tethering [1]. Surgical correction is associated with substantial perioperative risk due to prior sternotomies, adhesions, and comorbidities related to chronic immunosuppression [2]. Transcatheter mitral valve repair with the MitraClip® system has emerged as a valuable alternative for patients with symptomatic severe MR who are considered prohibitive surgical candidates; however, published experience in the transplant population remains limited [3,4]. We describe a technically demanding but successful MitraClip® procedure in a long-term heart transplant recipient and discuss thrombotic surveillance and management considerations in this unique clinical setting.
Case presentation
A 62-year-old female with a history of orthotopic heart transplantation in 2006 for chemotherapy-induced cardiomyopathy and maintained on routine post-transplant follow-up presented with progressive exertional dyspnea (New York Heart Association class III) and worsening MR on serial transthoracic echocardiograms. Her medical history included stage IV chronic kidney disease with a stable estimated glomerular filtration rate of 35 ml/min/1.73 m², prior endovascular aortic repair, and coronary stenting. Maintenance immunosuppression consisted of mycophenolate mofetil and everolimus. On March 15, 2024, transesophageal echocardiography (TEE) demonstrated preserved left ventricular ejection fraction (65%) and severe MR secondary to fibro-degenerative valve leaflet alterations, including posterior leaflet hypomobility and marked left atrial enlargement. Doppler indices suggested elevated left ventricular filling pressures without evidence of pulmonary hypertension.
Following Heart Team evaluation, the patient was deemed high surgical risk, and transcatheter edge-to-edge repair (TEER) with the MitraClip system was planned. She was admitted on April 8, 2024, for periprocedural optimization, and slow intravenous hydration was initiated to minimize the risk of contrast-induced kidney injury. On April 9, after endotracheal intubation and general anesthesia, coronary angiography confirmed the absence of significant epicardial coronary artery disease. Under TEE guidance, transseptal access via the right femoral vein was attempted. Anatomical distortion from prior surgery made septal crossing and leaflet grasping challenging, requiring multiple attempts before successful advancement of the guide system into the left atrium. A single MitraClip XTW was deployed in a central-medial position (A2-P2), reducing MR to mild severity with a residual mean transmitral gradient of 3 mmHg and normalization of pulmonary venous systolic flow. (Figures 1, 2).
Color Doppler TEE(A, B) Color Doppler TEE showing severe mitral regurgitation before clip deployment. (C, D, E) Color Doppler TEE images demonstrating the reduction of mitral regurgitation after clip placementTEE: transesophageal echocardiography
Pulmonary vein Doppler images(A) Pulmonary vein Doppler before MitraClip® showing systolic flow reversal. (B) Pulmonary vein Doppler after clip deployment demonstrating restoration of systolic-dominant flow
The patient was extubated in the catheterization laboratory and transferred to the intensive cardiac care unit. During her stay, arterial blood gas analysis revealed metabolic acidosis due to bicarbonate depletion, which resolved promptly after intravenous administration of 70 mEq sodium bicarbonate. She was discharged on April 12 (postoperative day three). At the three-month follow-up, TEE identified a small mural left atrial thrombus adjacent to the clip. Warfarin was initiated with a target international normalized ratio of 2-3, resulting in complete thrombus resolution after six weeks. At nine months, transthoracic echocardiography demonstrated stable mild MR (mean gradient: 3.4 mmHg), preserved left ventricular ejection fraction, and no thromboembolic events. The patient reported excellent functional status (New York Heart Association class I) (Figure 3).
Follow-up imaging findings(A, B) Transthoracic echocardiogram at 1-year follow-up showing trivial mitral regurgitation. (C) Continuous-wave Doppler showing a mean transmitral gradient of 3.4 mmHg
Discussion
MR following heart transplantation is a recognized but challenging entity, often arising from a combination of annular dilatation, graft remodeling, leaflet tethering, and atrial dysfunction [1]. Its management can be particularly complex because surgical intervention carries substantial perioperative risk due to prior sternotomy, dense mediastinal adhesions, and comorbidities related to chronic immunosuppression [2]. Hence, TEER has progressively emerged as an appealing alternative for carefully selected high-risk patients, experience in the transplant population is still limited to small series and case reports [3,4].
As our case confirms, TEER in transplanted hearts may present several technical challenges. Altered atrial geometry, variable septal thickness and fibrosis, and changes in leaflet mobility can complicate both transseptal access and leaflet grasping. These anatomical aspects underline the importance of comprehensive preprocedural imaging and experienced operators. Despite these challenges, TEER has shown encouraging procedural success and symptomatic benefit in the few reports available, supporting its feasibility in this unique population. Another important aspect highlighted by our case is the predisposition of transplant recipients to left atrial thrombosis. Multiple factors - including atrial mechanical impairment, endothelial dysfunction, and immunosuppressive therapy - may contribute to a prothrombotic milieu [5].
The detection of a small mural thrombus during follow-up underscores the need for vigilant surveillance after TEER. While warfarin remains the standard treatment for device-related thrombi, the role of direct oral anticoagulants in this setting warrants further investigation. Overall, this report reinforces the concept that TEER may represent a valuable therapeutic option for heart-transplant recipients with severe MR who are not optimal candidates for surgical intervention. However, the limited body of literature highlights the need for further dedicated studies to better define patient selection, procedural strategies, and optimal antithrombotic regimens in this complex clinical environment.
Conclusions
TEER with the MitraClip® system may represent a viable and effective option for selected heart-transplant recipients with severe functional MR who are not optimal candidates for surgical intervention. This report illustrates that, despite the anatomical challenges associated with the transplanted heart, TEER can achieve meaningful clinical improvement and provide a durable reduction in regurgitation. A multidisciplinary Heart Team approach, meticulous procedural planning, and vigilant post-procedural surveillance, particularly for thrombotic complications, are essential to optimize outcomes in this complex patient population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mitral regurgitation after cardiac transplantation Am J Cardiol Stevenson LW Dadourian BJ Kobashigawa J Child JS Clark SH Laks H 119122601987330024310.1016/0002-9149(87)90997-0 · doi ↗ · pubmed ↗
- 2Cardiac surgery after heart transplantation: elective operation or last exit strategy?Transplant Direct Goekler J Zuckermann A Osorio E Brkic FF Uyanik-Uenal K Laufer G Aliabadi-Zuckermann A 03201710.1097/TXD.0000000000000725 PMC 562774029138760 · doi ↗ · pubmed ↗
- 3Use of a Mitra Clip for severe mitral regurgitation in a cardiac transplant patient Proc (Bayl Univ Med Cent) Raza FS Grayburn PA Choi JW 2262273020172840509210.1080/08998280.2017.11929597 PMC 5349838 · doi ↗ · pubmed ↗
- 4Use of Mitra Clip in the percutaneous treatment of severe mitral regurgitation in heart transplant recipients Rev Esp Cardiol (Engl Ed) Salas M Roura G Arzamendi D Berdejo J Manito N Gómez-Hospital JA 9759787220193120110610.1016/j.rec.2019.03.015 · doi ↗ · pubmed ↗
- 5Venous thromboembolism in heart transplant recipients: incidence, recurrence and predisposing factors J Heart Lung Transplant Alvarez-Alvarez RJ Barge-Caballero E Chavez-Leal SA 1671743420152543452310.1016/j.healun.2014.09.039 · doi ↗ · pubmed ↗