Swallowing and feeding after disease-modifying treatment for spinal muscular atrophy: a systematic review of assessment modalities and outcomes
Yasmina Martí, Ksenija Gorni, Sandhya Kumari, Anadi Mahajan, Giovanni Baranello, Liesbeth De Waele, Katlyn E. McGrattan

TL;DR
This review examines how disease-modifying treatments for spinal muscular atrophy affect swallowing and feeding, highlighting the need for standardized assessments.
Contribution
The paper systematically reviews the impact of DMTs on bulbar function in SMA, emphasizing the lack of standardized swallowing assessments.
Findings
Most studies report functional swallow outcomes, but few use clinician-administered or imaging assessments.
Treatment before symptom onset leads to better feeding outcomes compared to treatment after symptom onset.
Swallowing assessment methods vary widely, making it difficult to compare study results.
Abstract
Feeding and swallowing deficits are reported across the spectrum of spinal muscular atrophy (SMA), with more profound symptoms associated with more severe disease. Patients treated with disease-modifying therapies (DMTs) demonstrate significantly improved life expectancy and motor function relative to untreated counterparts; however, limited data exist regarding the impact of DMTs on bulbar integrity, with evidence suggesting bulbar symptoms may persist, even when motor function has improved. This systematic literature review was conducted to identify assessments used to evaluate swallowing in patients with SMA treated with DMTs, and to describe the impact of DMTs on swallowing and feeding outcomes. Embase, MEDLINE, and Cochrane central were searched from May 2021 to February 2024 for studies reporting swallowing and feeding outcomes in patients treated with nusinersen, onasemnogene…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
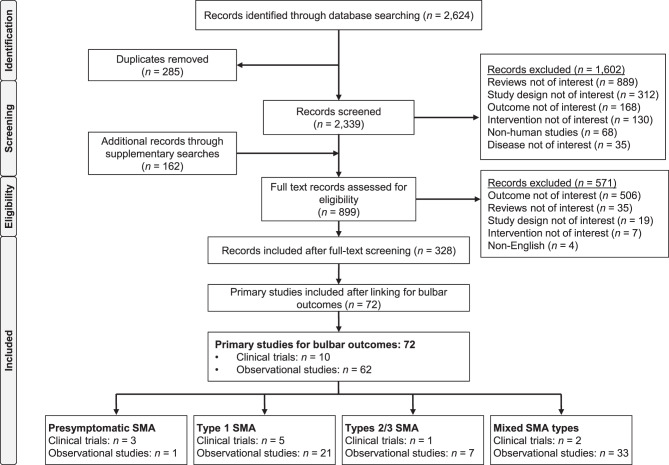 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurogenetic and Muscular Disorders Research · Amyotrophic Lateral Sclerosis Research · Nerve Injury and Rehabilitation
Background
Spinal muscular atrophy (SMA) is an autosomal recessive, progressive neuromuscular disease with an estimated global incidence of ~ 1 in 10,000 live births [1]. SMA is characterised by a deficiency in survival of motor neuron (SMN) protein [2], which leads to progressive muscle denervation, skeletal muscle atrophy, muscle weakness, and loss of motor function [1]. Although the severity of these deficits can vary greatly, feeding and swallowing deficits have been reported across all phenotypes [3–6].
In the most severe form, Type 1 SMA, bulbar deficits are prevalent, with infants exhibiting a rapid degeneration of oropharyngeal sucking and swallowing physiology that impedes the infants’ ability to express milk from the nipple, close the laryngeal opening to prevent aspiration, and clear ingested material from the pharynx [7]. The cumulative effect of these deficits in untreated patients has historically resulted in the reliance on tube nutritional support by 12 months of age [8], with children at high risk of developing aspiration pneumonia [4, 9]. In milder phenotypes (Types 2 and 3 SMA), reported deficits are isolated to chewing, instances of choking, and fatigue with meals [5, 6].
Given the prevalence and significance of these deficits, assessment of oropharyngeal swallowing integrity is critical in patients with SMA. Functional swallowing assessments can be categorised into two types: (1) clinician-administered assessments and (2) patient-reported outcomes. Clinician-administered assessments are those in which a provider makes determinations about the integrity of an individual’s swallowing biomechanics. One type of clinician-administered assessment is the clinical swallow evaluation, during which a clinician makes determinations about swallowing integrity using visual observation as they watch an individual eat and drink. Though valuable, clinical swallow evaluations are noted to have poor sensitivity for detecting pharyngeal swallow impairments, which cannot accurately be identified via observation alone [10–12]. As such, clinicians rely largely on findings from another form of clinician-administered assessment, an instrumental swallowing assessment, to fully characterise the integrity of internal biomechanics not visible to the naked eye. The gold standard in instrumental swallowing assessment is the videofluoroscopic swallow study, a procedure that uses an x-ray to quantify the integrity of oropharyngeal swallowing physiology and the impact on bolus flow, such as penetration or aspiration [13]. Other instrumental swallowing assessments such as fibreoptic endoscopic evaluation of swallowing and high-resolution manometry can also provide valuable insights into the integrity of these internal processes.
Whilst measures of swallowing integrity are critical, assessment of the functional implications of these biomechanics are of equal importance. Functional swallow outcomes can be reported in a variety of ways, including descriptive assessments, oral intake status, and the perception of swallowing integrity collected through patient-reported outcomes.
Disease-modifying therapies (DMTs) designed to halt disease progression hold promise for facilitating swallowing integrity. These treatments, including nusinersen (SPINRAZA^®^), onasemnogene abeparvovec (ZOLGENSMA^®^), and risdiplam (EVRYSDI^®^), have been shown to significantly improve the life expectancy and gross motor integrity of patients with SMA when compared with their untreated counterparts [14]. However, there are limited data regarding the impact of DMTs on bulbar integrity, with some evidence suggesting that bulbar symptoms may persist in patients even when motor function has improved [15].
Given the implications in validity of outcomes, the aim of this systematic literature review (SLR) was to identify the types of swallowing assessments used in patients with SMA treated with DMTs, and to describe the impact of DMTs on swallowing and feeding outcomes in SMA.
Methods
This SLR was reported in accordance with PRISMA guidelines. Searches were conducted in the Embase^®^, MEDLINE^®,^ and Cochrane central electronic databases and included studies published from database inception to the end of February 2024. A search strategy was developed based on the Population, Interventions, Comparison, Outcomes, and Study (PICOS) design framework [16] (Supplementary Tables 1 & 2, Additional File 1). Eligible publications included randomised control trials (RCTs), non-RCTs, single-arm studies, and real-world observational studies (prospective and retrospective) that reported data from patients with presymptomatic and symptomatic Types 1–3 SMA who were treated with at least one SMA DMT (nusinersen, onasemnogene abeparvovec, or risdiplam). Cross-sectional studies and case reports/series were excluded. Supplementary searches were performed to identify data published as relevant conference proceedings (see Supplementary Table 3, Additional File 1 for a full list of conferences included in the supplementary searches).
Assessment of bias and quality of evidence of the included studies was conducted using the National Institute for Health and Care Excellence (NICE) manufacturer’s template for RCTs [17], the Agency for Healthcare Research Quality (AHRQ) checklist for non-RCTs and single-arm trials [18], and the Newcastle-Ottawa Scale for observational studies [19].
Data were extracted from the individual studies and summarised qualitatively. Outcomes were classified as clinician-administered swallowing assessments (clinical swallow evaluation and instrumental swallow evaluation) and functional swallowing outcomes (oral intake status and patient-/caregiver-reported outcomes) for descriptive analysis.
Results
A total of 2,624 records were identified through the SLR and 162 records were identified via supplementary searches (PRISMA diagram – Fig. 1). After screening for eligibility, 72 primary studies (10 clinical trials [14%] and 62 observational studies [86%]) were identified that reported swallowing and feeding outcomes in patients with SMA treated with DMTs. Three clinical trials and one observational study reported data in presymptomatic SMA, 26 studies (five clinical trials, 21 observational studies) reported data in a Type 1 SMA population, eight studies reported data from a Type 2/3 SMA population (one clinical trial and seven observational studies), and 35 studies (two clinical trials and 33 observational studies) reported data from mixed SMA type populations. Only 48 (68%) investigations reported pre-treatment and post-treatment assessment of bulbar function. Fig. 1PRISMA diagram. Abbreviations: PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses; SMA, spinal muscular atrophy
We have classified the results into studies that reported on clinician-administered assessment (clinical swallow evaluation and instrumental assessments) and studies that reported on functional swallow outcomes. Out of 72 studies identified, almost all (71/72, 99%) reported functional swallowing outcomes, such as oral intake status (61/72, 85%) and patient-reported outcomes (14/72, 19%). Only 14 (19%) studies used clinician-administered assessments; most of these studies (11/14, 79%) reported results from clinical swallow evaluations, with only 5/14 (36%) using instrumental assessments. Results were reported using descriptive statistics for almost all (67/71, 94%) investigations.
Clinician-administered swallowing assessments
Clinical swallow evaluation
Twelve publications from 11 studies reported on swallowing outcomes following a DMT using clinical swallow evaluation (Table 1). Table 1. Observational clinical swallow evaluationDMTStudy[reference]Study typeNSMA typeSMN2 copy numberAge at onsetMedian(range/IQR)Mean [range/SD]Age at treatment initiationMedian(range/IQR)Mean [range/SD]Outcome assessedAt timepoint of interest (%)^a^Baseline6 months12 months18 months24 monthsOther(timepoint)Studies in presymptomatic SMANusinersenNURTURE**De Vivo 2019 [20]SA15Presymptomatic2NR19.0d (8–41)19.5d [9.29]Good sucking and swallowing (HINE-1 score 3)----80(Day 778)-103NR23.0d (3–42)22.3d [12.45]Good sucking and swallowing (HINE-1 score 3)----100(Day 778)-Onasemnogene abeparvovecSPR1NTStrauss 2022 [21]SA14Presymptomatic2NR21.0d(8.0–34.0)20.6d[SD: 7.9]Normal swallowing of thin liquids^b^100--93--SPR1NTPost-hoc analysisShell 2023 [22]142NR20.6d(8.0–34.0)Normal swallowing of thin liquids^b^---100--153NR28.7d*(9.0–43.0)Normal swallowingof thin liquids*^b^100*---100-RisdiplamRAINBOWFISH Finkel 2022* [23]SA7Presymptomatic2,3, and ≥4-26.5d(16–40)(n = 18)Able to swallow100-100---Studies in a Type 1 SMA populationNusinersenDe Lucia 2020 [24]ROS23Type 12, 3NRNROral disorders (swallow’s disease and/or difficulties chewing)30--70--Onasemnogene abeparvovecSTART**McGrattan 2023 [25]DC/DE11Type 12NRNRSwallowing normally36---100-STR1VE-EUMercuri 2021 [26]SA33Type 121.6m*[SD: 0.9]4.1m[SD: 1.3]Intact swallowing^c^97-----STR1VE-EUMcGrattan 2023* [25]SA33Type 121.6m*[SD: 0.9]4.1m[SD: 1.3]Swallowing normally97**--91-STR1VE-USDay 2021* [27]*SA22Type 121.8m(1.0–3.0)1.9m[SD: 1.2]3.5m(2.7–5.3)3.7m[SD: 1.6]Swallowing normally^c^100--55 (at 18m of age)--Normal or functional swallow with consistencies other than thin liquid---32 (at 18m of age)--STR1VE-USMcGrattan 2023* [25]*SA22Type 121.8m(1.0–3.0)1.9m[SD: 1.2]3.5m(2.7–5.3)3.7m[SD: 1.6]Swallowing normally*100--91--McGrattan 2023 [25]*STARTSTRIVE-EUSTR1VE-USPost-hoc analysis65Type 12NRNRNormalswallow88----92 (end of study)^c^RisdiplamFIREFISHPart 2Darras 2021* [28]*SA41Type 121.5m(1.0–3.0)5.3m(2.2–6.9)CGI-C: improvement or no change--71---CGI-C: very much improved--7---CGI-C: much improved--29---CGI-C: minimally improved--10---CGI-C: unchanged--24---CGI-C: worse--10---CGI-C: much worse--7---CGI-C: minimally worse--2---Nusinersen,onasemnogene abeparvovec,risdiplam^d^Zang 2023 [29]POS10Type 122.0m(0–7)3.8m(0.7–8.9)Weak suck60.0-50.0---Strong suck10.0-20.0---Experienced fatigue related to feeding66.67N* = 9-37.5N = 8---Studies with a Type 2/3 SMA populationNusinersenAmbawatte2022 [30]ROS11Types 2/32–4NRNRSwallowing difficulties9.1-----RisdiplamAmbawatte2022 [30]ROS9Type 23,4NRNRSwallowing difficulties22.2-----Studies with a mixed SMA type populationNusinersen switch to onasemnogene abeparvovecAlNaimi2022 [31]ROS11Type 1/22/3NR(4–23m)Swallowing dysfunction45.5----45 (PGT)9Type 12NR12m(4–23)Swallowing dysfunction56-----Onasemnogene abeparvovec2Type 23*NR22m(21–23)*Swallowing dysfunction0-----Abbreviations: CGI-C, Clinical Global Impressions Scale-Clinical change; d, days; DC, dose comparison; DE, dose escalation; DMT, disease-modifying therapy; HINE-1, Hammersmith Infant Neurological Examination, Module 1; IQR, interquartile range; m, months; NR, not reported; PGT, post-gene therapy; POS, prospective observational study; ROS, retrospective observational study; SA, single arm; SD, standard deviation; SMA, spinal muscular atrophy; SMN, survival of motor neuron^a^ Values correspond to percentages of patients (N), unless stated otherwise. Timepoint refers to time on treatment, unless specified^b^ As demonstrated through a formal swallowing test with thin liquids^c^ As demonstrated through a formal swallowing test with thin or very thin liquids^d^ Nine children received onasemnogene abeparvovec; five of these nine had already received nusinersen. One child received risdiplamClinical trial publications are in italics
Presymptomatic SMA
Promising bulbar outcomes were reported amongst presymptomatic patients across all DMTs (nusinersen, onasemnogene abeparvovec and risdiplam; n = 4 studies). Clinical swallow evaluation outcomes amongst infants with two copies of the SMN2 gene revealed ‘good’ sucking and swallowing in 80% of infants treated with nusinersen [20], ‘normal’ swallowing of thin liquids in 93–100% infants treated with onasemnogene abeparvovec [21, 22], and ‘the ability to swallow’ in 100% of infants treated with risdiplam [23]. Length of follow-up ranged from 18 to 24 months across investigations.
Symptomatic SMA
Less optimistic outcomes were found when treatment was initiated after symptom onset for patients with Type 1 SMA. The ability to generalise results across the six studies identified was limited by the variety in reporting methods: three studies (50%) reported proportions of patients who had ‘normal’ or ‘intact’ swallowing, one study reported swallowing stability relative to baseline [28]; one reported sucking strength in infants [29] and one reported the presence of swallowing or chewing dysfunction [24]. The proportion of patients who achieved ‘normal’ swallowing after treatment with nusinersen or onasemnogene abeparvovec varied widely, with 30–100% of patients reported to have ‘normal’ swallowing after at least 18 months of follow-up [24–27]. Relative to baseline, studies indicate the majority of patients ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$ \ge $$\end{document} 60%) maintain or improve their pre-treatment swallow integrity regardless of the DMT they receive (nusinersen, onasemnogene abeparvovec or risdiplam) over 12–24 months of follow-up.
Longitudinal data were not available for feeding and swallowing outcomes in Types 2 and 3 SMA.
Instrumental swallowing assessments
Five observational studies reported data from instrumental swallowing assessments in patients treated with DMTs (Table 2). Four studies used videofluoroscopic swallow study or fibreoptic endoscopic evaluation of swallowing to measure swallow biomechanics and one study evaluated contracture in the temporomandibular joint by measuring mouth opening. Instrumental investigations that examined swallowing were limited in sample size, did not report biomechanics in a standardised method (only two of the four studies using imaging specified that the penetration–aspiration scale was used to score swallowing integrity [4, 29]), and results were frequently restricted to reports of penetration or aspiration alone. The length of follow-up was also unspecified in 3/5 (60%) studies. Table 2. Instrumental swallowing assessmentsDMTStudy[reference]Study typeNSMA typeSMN2 copy numberAge at disease onset Median(range/IQR)Mean [range/SD]Age at treatment initiationMedian (range/IQR)Mean [range/SD]Instrumental assessment usedOutcome assessedAt timepoint of interest^a^Baseline6 months12 months18 months24 monthsOther(timepoint)Studies in presymptomatic SMANusinersen switch to onasemnogene abeparvovecChiang2023 [32]ROS1Presymptomatic2NRNBS-diagnosedNu: 6wOA: 9wVFSSLaryngeal penetration and aspiration with thin liquids100(aged 5m)----0 (NR^b^)Studies in a Type 1 SMA populationNusinersenvan der Heul 2020 [4]POS5Type 12--VFSSSilent aspiration-----80 (NR)Nusinersen switch to onasemnogene abeparvovecOnasemnogene abeparvovecRisdiplam^c^Zang 2023 [29]POS10Type 122.0m(0.0–7.0)3.8m(0.7–8.9)FEESPAS: median score54.5----No penetration or aspiration (PAS = 1)1010----Penetration(PAS = 2–5)4050----Aspiration with cough(PAS = 6–8)4020----Silent aspiration(PAS = 8)3010**Studies with a mixed SMA type populationOnasemnogene abeparvovecBeri 2023[33]POS22NRNRNRNR-Mean maximal mouth opening (SD)18.8 (5.9)----20.7 (5.0) (3m)Onasemnogene abeparvovec and nusinersen switch to onasemnogene abeparvovec^d^AlNaimi2022 [31]ROS3Type 1/22/3Type 1: 2m(0.3–6)Type 2: 20m(21–23)Type 1: 12m(4–23)Type 2: 22m(21–23)VFSSNormal swallow100----100(NR)Abbreviations: DMT, disease-modifying therapy; FEES, fibreoptic endoscopic evaluation of swallowing; IQR, interquartile range; m, months; NBS, newborn screening; NR, not reported; Nu, nusinersen; OA, onasemnogene abeparvovec; PAS, penetration–aspiration scale; POS, prospective observational study; ROS, retrospective observational study; SD, standard deviation; SMA, spinal muscular atrophy; SMN, survival of motor neuron; VFSS, videofluoroscopic swallowing studies; W, weeks^a^ Values correspond to percentages of patients (N), unless stated otherwise. Timepoint refers to time on treatment, unless specified^b^ No timepoint specified for resolution of signs and symptoms of aspiration^c^ Nine children received onasemnogene abeparvovec; five of these nine had already received nusinersen. One child received risdiplam^d^ Patients with Type 1 SMA received nusinersen before receiving onasemnogene abeparvovec. Patients with Type 2 SMA received onasemnogene abeparvovecClinical trials are in italics
Presymptomatic SMA
The only investigation in presymptomatic SMA was Chiang et al. [32], and was limited to outcomes in a single patient.
Symptomatic SMA
Two of the three studies examining swallowing outcomes in patients treated after symptom onset were in children with Type 1 SMA. High rates of penetration or aspiration were observed after treatment: specifically, van der Heul et al. reported aspiration amongst 80% of children treated with nusinersen (timepoint unspecified) [4], and Zang et al. reported penetration or aspiration and pharyngeal residue in all but one (n = 9/10) patient following 6 months of treatment with varying DMTs [29]. These high rates of impaired swallowing biomechanics are in contrast with the results from AlNaimi et al. who reported ‘normal’ swallowing in three patients with Type 1 or Type 2 SMA after treatment with onasemnogene abeparvovec [31]. Biomechanical correlates constituting normal integrity were not reported [31].
Significant improvements in maximal mouth opening were reported in children with SMA after 3 months of treatment with onasemnogene abeparvovec in as single study [33].
Functional swallowing outcomes
Functional swallowing outcomes were assessed using a variety of metrics. Oral intake status was the most common functional swallow outcome used (85%, 61/72 studies; Table 3). Other studies (19%,14/72; Table 4) reported results from a battery of standard patient-/caregiver-reported swallowing assessments, including Parent Assessment of Swallowing Ability (PASA), the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale, Oral and Swallowing Abilities Tool (OrSAT), Syndey Swallow Questionnaire, Egen Klassifikation Scale Version 2, the Murray secretion scale, Jaw Functional Limitation Scale, and Individualised Neuromuscular Quality of Life questionnaire. Table 3. Oral feeding statusDMTStudy(reference)Study typeNSMA typeSMN2copy numberAge at onsetMedian (range)Mean [range/SD]Age at treatment initiation/enrolmentMedian (range/IQR)Mean [range/SD]Outcome assessedAt timepoint of interest (%)^a^Baseline6 months12 months18 months24 monthsOther(timepoint)Studies in presymptomatic SMANusinersenNURTURE Sansone 2021[35]SA15Presymptomatic2NR≤6wFull oral nutrition----84(Day 778)-103**NR≤6wNot tube fed----100(Day 778)-NURTURECrawford 2023 [36]SA25Presymptomatic2, 3NR22d(3–42)PEG-4(at 5.9m)--8(at 19.4m and 22.5m)8 (at 41.9m and 50.1m)Onasemnogene abeparvovecSPR1NTStrauss 2022 [21]SA14Presymptomatic28.0d (1–14)^b^7.2d*[SD: 4.8]21d(8–34)Full oral nutrition100**--100--SPR1NTStrauss 2020* [34]302–4NR2 SMN2 copies20.6d*[8.0–34.0]3 SMN2 copies28.7d**[9.0–43.0]Full oral nutrition-----100(CCOD: 31 Dec 2019)SPR1NTPost-hoc analysisShell 2023* [22]*SA14Presymptomatic28.0d (1–14)7.2d[SD: 4.8]*^b^*21d (8–34)20.6d[SD: 7.9]Fully oralnutrition100**--100--1538.0d (2–26)^b^9.9d[SD: 7.7]32.0d(9–43)28.7d [SD:11.7]100---100-RisdiplamRAINBOWFISH Finkel 2022* [23]SA7Presymptomatic2, 3, 4NR26.5d(16–40)(n = 18)Able to feed orally100-100---Studies in a Type 1 SMA populationNusinersenDe Lucia 2020 [24]ROS23Type 12, 3NRNRGastrostomy/NG tube18.0--56.0--Sansone 2020 [37]EAP118Type 11–4NR42.8m (IQR:11.0–102.8)NG tube10.2----5.7 (T300)N = 105PEG54.2----65.7 (T300)N = 105Lavie 2020 [38]POS20Type 12, 3-13.5m(1–184)IQR: 4–56Gastrostomy/ NG tube65.0---95.0-van der Heul 2020 [4]POS5Type 1238d (21–90)63d (3–218)Tube feeding-----100 (median start at 382d)Bianchi 2021[39]POS10Type 12, 32.5m (0–5)9.5m(2–28) [SD: 10.02]Required tube feeding50.060.0^c^----Chen 2021 [40]ROS9Type 12, 33m (1–5)10.6m(2.7–178.6)Gastrostomy22.0----66.7(30.1m)Mendonca2021 [41]POS21Type 12, 32.7m[SD: 1.5]NRFeeding orally4.84.8^d^----Oral + gastrostomy9.5----9.5^d^Gastrostomy85.7----85.7^d^Modrzejewska 2021 [42]POS26Type 12, 3, 42m (0–6)2m[SD: 1.72]23m (3–165)36.57m[SD: 39.25]PEG/g astrostomy57.7----50.0(18–26m)Pane 2021 [43]EAP68Type 11–4NR3.96[0.20–15.92] [SD: 3.90]Orally fed47.1---35.3-Tube fed52.9---64.7-Ergenekon2022 [44]ROS52Type 12, 32.2m[SD: 1.8]11.3m(4.0–34.8)Able to feed orally42.332.6N = 46----Gastrostomy21.234.8N = 46----NG feeding36.532.6N = 46----Menard 2022 [45]ROS17Type 12, 32m (1–6)4m (2–29)NG tube-----52.9(mean: 10m; IQR 4–15)Gastric feeding tube-----64.7(mean: 16m; IQR 14−23.5)Weststrate2022 [15]ROS24Type 12, 3NR11m[1m–7y 6m]p-FOIS median score3122--Tube feeding58.3-83.3-83.33Type 1a2, 3NR2y 2m(1m–4y 3m)p-FOIS median score1111--Tube feeding100-100-100-9Type 1b2NR4m(2m–1y 4m)p-FOIS median score3122--Tube feeding55.6-100-100-12Type 1c2, 3NR1y 7m(8m–7y 6m)p-FOIS median score5233--Tube feeding50.0-66.7-66.7-Pane 2023b [46]EAP48Type 11–3NR3.3y[7d–12y] [SD: 3.6]Oral feeding52.1----41.7 (48 m)Gastrostomy orNG tube47.9----58.3 (48 m)Pechmann2023b [47]SMARTcare registryPOS88Type 1^e^≤2 years of age at start of treatment1–≥42m (0–10)2.8m[SD: 2.5]7m (0–24)8.4m[SD: 6.0]No tube feeding70.5-----Tube feeding supplementary19.3-----Tube feeding exclusively10.2-----55Type 1^e^ >2 years of age at start of treatment1–≥45m (0–56)6.2m[SD: 7.8]68m(24–207)89.8m[SD: 58.4]No tube feeding61.8-----Tube feeding supplementary25.5-----Tube feeding exclusively12.7-----Probability of the need for tube feeding43.6----51.4(38m)Shin 2023 [48]ROS7Type 12, 3NR(3.0–4.4m)3.7m[SD: 1.4]NR(6.4–9.4y)7.3y[SD: 4.0]Orogastric14.3----14.3 (46.2m)Gastrostomy85.7----85.7 (46.2m)Xiao 2023 [49]ROS11Type 121.5m(0.5–4.0)5.4m(2.0–108.7)Enteral feeding54.5----NROnasemnogene abeparvovecSTART**Mendell 2017 [50]DC/DE12Type 12Cohort 21.4m[0–3.0]Cohort 23.4m*[0.9–7.9]Required enteral feeding41.7**-----Oral nutrition64**-----Alecu 2021START LTFU* [51]POS13Type 12NR0.3y(0.1–0.6)0.3y(SD: 0.2)Did not require feeding support-----60(CCOD: Dec 2019)Fed orally-----100(CCOD: Dec 2019)STARTMcGrattan 2023 [25]SAPost-hoc analysis11Type 12NRNRFull oral nutrition63.6*---54.5 (at 24m of age)-STR1VE-EU Mercuri 2021 [26]SA33Type 121.5m(0.0–4.0)1.6m[SD: 0.9]4.1m(1.8–6.0)4.1m[SD: 1.3]Required feeding support27.3**--15.2 (at 18m of age)--STR1VE-EUMcGrattan 2023* [25]SAPost-hoc analysis32Type 12NRNRFull oral nutrition81.2*--75.0--STR1VE-USDay 2021* [27]SA22Type 121.8m*(1.0–3.0)1.9m[SD: 1.2]3.5m(2.7–5.3)3.7m[SD: 1.6]Able to swallow thin liquid100**--54.5 (at 18m of age)--Did not require any non-oral feeding support100**-----Fed exclusively by mouth---86.4 (at 18m of age)--Did not require feeding support at any point during study---68.2 (at 18m of age)--STR1VE-USMcGrattan 2023* [25]SAPost-hoc analysis22Type 12NRNRFull oral nutrition100*--86.4 (at 18m of age)--START STR1VE-EUSTR1VE-USMcGrattan 2023* [25]*SAPost-hoc analysis65Type 12NRNRFull oral nutrition84.6----75.4(aged 18m and 24m)Bitetti 2022 [52]POS9Type 122.7m[0–5][SD: 1.9]NRPEG tube22.2----22.2 (3m)Gowda 2023 [53]ROS15Type 1NRNRNR(2–38m)Fully orally fed40.0----40.0(8–15m)Fully tube fed40.0----40.0(8–15m)Mixed oral and tube feeding13.3----6.7(8–15m)RisdiplamFIREFISHPart 1* [54]DC/DE21Type 122.0m(0.9–3.0)6.7m(3.3–6.9)Able to feed orally--85.7---Combination of oral and tube feeding--14.3---FIREFISHPart 2 [28, 55]SA41Type 121.5m*(1.0–2.0)5.3m(4.2–6.8)Able to feed orally85.4**-82.9-85.4-Fed exclusively via feeding tube9.8**---7.3-Fed via combination of oral and feeding tube4.9**-14.6-14.6-Fed exclusively orally80.5**-68.3-70.7-FIREFISH Part 1 + Part 2 pivotal dose cohort [55]SA58Type 12--Able to feed orally--84-83-Risdiplamswitch to onasemnogene abeparvovecQuelch2023 [56]ROS5Type 1NR5.8m (1–12)26m(7–87)Exclusively oral feeding40.0-----Exclusively NG feeding40.0-----Mixed NG/oral feeding20.0-----Onasemnogene abeparvovec (n = 4);nusinersen switching to onasemnogene abeparvovec (n = 5);risdiplam(n = 1)Zang 2023 [29]POS10Type 122.0m(0.0–7.0)3.8m(0.7–8.9)NdSSS median score4.53.0----Studies with a Type 2/3 SMA populationNusinersenAmbawatte 2022 [30]ROS9Type 23,4NRNRGastrostomy11.1-----Vetlesen 2024[57]POS20Type 23, 4NR7.0y(IQR: 2.0–12.9)Gastrostomy5.0----5.0 (3y)20Type 32, 3, 4NR8.4y(IQR: 4.3–12.2)Gastrostomy0----0 (3y)Studies with a mixed SMA type populationNusinersenAragon-Gawinska 2018 [94]POS15NR23m (1.5–5)19.8m(8.3–42.0)No nutritional support7360---60 (M2)Tube feeding2740---40 (M2)17NR34m (2–6)27.7(8.8–113.1)No nutritional support7171---71 (M2)Tube feeding2929---29 (M2)33NR2, 34m (1.5–6)21.3m(8.3–113.1)No nutritional support7364---67 (M2)Tube feeding2736---33 (M2)Audic 2020 [63]ROS30Type 1/2(age <2y)2–4NR(3m–17y)NG tube/gastrostomy10.0-16.7---47Type 1/2(age 2–5y)NG tube/gastrostomy12.8-12.8---46Type 1/2(age 6–17y)NG tube/gastrostomy10.9-10.9---Kim 2020 [61]ROS4Type 12(7d–5m)NRGastrostomy50.0----50.0 (median F/U 6.1m)Oral feeding without difficulty50.0----50.0 (median F/U 6.1m)3Type 2310.67m(8–15)NRGastrostomy0----0 (median F/U 6.1m)Oral feeding without difficulty100----100 (median F/U 6.1m)Osredkar 2021 [64]POS61Types 1–32–4NR8.6y(0.2–18.8)Gastrostomy13.1----14.8 (14m)Barisic 2022 [95]ROS18Type 1NRNR3m–3.5yRequired feeding support16.7----16.7 (36m)Calvo-Medina 2022 [96]ROS20Type 1/22–47m(IQR: 4–12)4 y (IQR: 19m–11)NG tube/gastrostomy-----20.0 (34m)Hepkaya 2022 [65]ROS43Types 1–3<3 copies≥3 copies27.8 [SD: 39.1]^b^60.8[SD: 69.5]NG tube9.3----18.6 (T1)^f^14.3 (T2)^f^Gastrostomy2.3----4.7 (T1)^f^9.3 (T2)^f^Oral feeding88.4----76.7 (T1)^f^76.7 (T2)^f^Pechmann 2022a [59]POS256Types 2/31–≥4NRNRTube feeding5.5----7.4 (F/U ≤38m; CCOD Nov 2021)Pechmann 2023a [62]SMARTcare registryPOS114Type 32–≥440.8 [99% CI 30.4–51.5]103.3 [99% CI 89–117.6]Tube feeding0----0 (38m)^g^Tscherter2022 [97]POS6Type 1(aged 0–18m)2, 3NR0.2y(0.1–0.4)Tube feeding0----66.7(median F/U 25.5m)Belancic 2023 [58]ROS52Type 1–31–4NR13.4y(0.1–51.1)16.4y[SD: 13.2]PEG7.7----9.6 (completed the first 6 doses)NG tube19.2----17.3 (completed the first 6 doses)18Type 11–3NR5.2y(0.1–20.8)6.3y[SD: 6.3]PEG22.2----27.8 (completed the first 6 doses)NG tube44.4----38.9 (completed the first 6 doses)6Type 21–3NR10.2y(1.5–16.7)8.8y[SD: 6.0]PEG0----0 (completed the first 6 doses)NG tube33.3----33.3 (completed the first 6 doses)28Type 32–4NR24.8y(4.2–51.1)24.5y[SD: 12.3]PEG0----0 (completed the first 6 doses)NG tube0----0 (completed the first 6 doses)Dabbous 2023 [70]ROS19Types 1–3NRNRNRImproved/maintained in eating function-----58.8(n = 17)Johnson 2023 [67]ROS27UnclearNRNRNRGastrostomy-70.0(0–6m)52.0(6–12m)-26.0(12–24m)-Öz Yıldız 2023 [98]ROS18Type 1NRNR6.5m(1–123)PEG-----11.1 (37.7m)NG tube-----5.6 (37.7m)Toro 2023 [99]ROS62Types 1/2NRNR13.1[SD: 7.1][IQR: 7.0–21.0]Nutritional support-----74.2 (10m)NG tube-----72.6 (10m)Audic 2024 [66]ROS57Types 1/22, 3NR16m (2–34)NG tube3.5----0 (36m)Gastrostomy7.0----24.6 (36m)Onasemnogene abeparvovecLT-002Darras 2023* [100]SA25PresymptomaticIVNRNRNRNutritional support*-----0 (CCOD May 2022)38SymptomaticIVNRNRNRNutritional support-----20.0 (CCOD May 2022)63Presymptomatic/symptomaticIV totalNRNRNRAble to feed orally-----95 (CCOD May 2022)18ITNRNRNRNutritional support-----0 (CCOD May 2022)Able to feed orally-----100 (CCOD May 2022)Pane 2023a [101]POS46Presymptomatic + Type 12/3NRNRDid not need nutritional support78.3-78.3---Required tube feeding21.7-21.7---RESTOREFinkel 2023 [102]19NR≥4NR^h^3 (1–11)Nutritional support---**--0(CCOD Dec 2022)RESTORE Servais 2024 [103]POS168Types 1–3Unknown,1, 2, 3, ≥4NR3 (1–10)6.38 [SD: 8.29]Fed exclusively by mouth--96.6**---Wang 2023 [68]ROS4Type 1/2NRNRNRWeaned off NG tube to oral feeding**--**--**-25.0 (NR)Waldrop2020 [69]ROS21Presymptomatic + symptomatic SMA2–4NR(1–23m)Feeding orally (exclusively and partially)76.2--**--80.9 (NR)Dabbous 2023 [70]ROS8Types 1–3NRNRNRSubjective improvement/maintenance in eating function-**--**--**83.3 (NR)N = 6Stettner 2022 [104]POS6Type 1NRNR5m[2w–17m]Required nutritional support-----67 (270d)Chiang2023 [32]ROS11Unclear2, 3NR3.6w (IQR: 3.3–21.3)Enteral feeding0----0 (NR)Martins 2023 [71]POS25Type 1/2NRNRNRStabilisation or improvement in oral function--100---Gastrostomy--4---Toro 2023 [99]ROS12Types 1/2NRNR14.2[SD: 6.7] (IQR: 8.8–20.5)Nutritional support-----50.0(9.8m)Gastrostomy-----41.7(9.8m)Waldrop2024 [72]ROS19Unclear2–4NR(7–729d)Unable to eat orally52.6-----Improved in oral feeding status-----36.8 (33.3m)46Decline in oral feeding status-----0(33.3m)Nusinersen, onasemnogene abeparvovecAlNaimi2022 [31]ROS9Type 122m (0.3–6)^b^12m (4–23)Enteral feeding55.6----55.6(F/U 6–24m)Nusinersen, onasemnogene abeparvovec, risdiplamSegovia 2021 [105]ROS21Type 1NRNR4y [0–9]^i^Tube feeding41.1 (NR)-----62Type 2NRNR11y (2–37)^i^Tube feeding2.5 (NR)-----Nusinersen switched to onasemnogene abeparvovecDabbous 2023 [70]ROS15Types 1–3NRNRNRSubjective improvement/maintenance in eating function-----50.0 (NR)N = 14Nusinersen monotherapy, onasemnogene abeparvovec monotherapy, nusinersen followed by risdiplamAngeli 2023 [106]ROS11Presymptomatic/Type 1/2/3NRNR61.7m(SD: 66.5)NG tube or gastrostomy-----0(43m)Onasemnogene abeparvovecNusinersen switch to onasemnogene abeparvovecLatzer 2023 [60]ROS6Type 1a21.62m[0.1–2.5]3.69m[0.75–6]Oral feeding66.7--33.3--Enteral feeding33.3--66.7--14Type lb2, 31.96m[0.2–4.0]10.51m[0.3–24]Oral feeding92.9--71.4--Partially oral and enteral feeding0--14.3--Enteral feeding7.1--14.3--3Type 1c3, 44.4m[4.1–5.0]9.9m[4.7–18]Oral feeding100--100--2Type 2310.55m [7.1–14]20m [19–21]Oral feeding100--100--25Types 1/22–4-6.1m (3.3–17.0)Enteral feeding12--24--Oral feeding88--68--Partially oral and enteral feeding0--8--Risdiplam (n = 45); nusinersen (n = 20); onasemnogene abeparvovec (n = 4)Vuillerot 2023 [107]ROS11Type 1NRNRNRFed exclusively by mouth-----81.8(1–8y^j^)Abbreviations: CCOD, clinical cut-off date; CI, confidence interval; d, days; DMT, disease-modifying therapy; CCOD, clinical cut-off date; DC, dose comparison; DE, dose escalation; EAP, expanded access programme; F/U, follow-up; IQR, interquartile range; IT, intrathecal; IV, intravenous; LTFU, long-term follow-up; m, months; NdSSS, Neuromuscular Disease Swallowing Status Scale; NG, nasogastric; NR, not reported; PEG, percutaneous endoscopic gastrostomy; p-FOIS; Paediatric Functional Oral Intake Scale Score; POS, prospective observational study; ROS, retrospective observational study; SA, single arm; SD, standard deviation; SMA, spinal muscular atrophy; SMN, survival of motor neuron; T1, timepoint 1, T2, timepoint 2; T300, 300 days post-infusion; w, weeks; y, years^a^ Values are percentages of patients (N), unless otherwise stated. Timepoint refers to time on treatment, unless specified^b^ Age at diagnosis^c^ One patient who did not require nutritional support at baseline required an NG tube at Day 180 and one patient who required an orogastric tube at baseline had received a PEG by Day 180^d^ Six infants were followed up for 6 months, five for 12 months, seven for 16 months, and three for 24 months. No infant changed their feeding status over the duration of F/U. One infant with gastrostomy died within 6 months of F/U^e^ All patients under treatment with nusinersen who never had the ability to sit independently before the start of treatment were identified for data analysis^f^ T1 was performed after the nusinersen loading doses were administered – Day 64 for Type 1 SMA and Day 274 for Types 2/3 SMA. T2 was performed 4 months after the first maintenance dose of nusinersen was given: ~Day 187 for Type 1 SMA and ~Day 643 for Types 2/3 SMA^g^ One paediatric patient (0.9%) required tube feeding for a period of 6 months during the study^h^ All but one patient received presymptomatic treatment^i^ Age at baseline^j^ A retrospective study of patients followed in a neuromuscular disease reference centre between 2012 and 2022Clinical trials are in italicsTable 4Patient-reported swallowing and feeding outcomesDMTStudy(reference)Study typeNSMA typeSMN2 copy numberAge at onsetMedian (range)Mean [range/SD]Age at treatment initiation/enrolmentMedian (range/IQR)Mean [range/SD]Outcome assessedAt timepoint of interest (%)^a^Baseline6 months12 months18 months24 monthsOther(timepoint)Studies in presymptomatic SMANusinersenNURTUREDay 778: Sansone 2021[34]5y: Crawford 2023[35]SA25Presymptomatic2/3NR22.0d(3–42)PASA: able to swallow----92(Day 778)92(5y)PASA: not being tube fed----84(Day 778)80(5y)PASA: never gagged/choked on liquid food----91(Day 778)-PASA: never gagged/choked on solid food----87(Day 778)-PASA: no swallowing concerns over choking^b^----88(Day 778)76(5y)PASA: no aspiration concerns whilst eating^b^----96(Day 778)80(5y)152NR*≤6wPASA: not being tube fed----73(Day 778)67 (5y)103NR≤6wPASA: not being tube fed100(Day 778)100 (5y)Studies in a Type 1 SMA populationNusinersenBerti 2022 [73]POS18Type 1 – allNRNR6.5m[3w–15m]Mean%-change (SD) in OrSAT score---−5.45% (28.69)--8Type 1 – patients who never had PEG/tracheostomyMean%-change (SD) in OrSAT score---+1.79% (20.02)--2Type 1 – patients who required tube feeding after treatment startedMean%-change (SD) in OrSAT score---−67.86% (33.67)--4Type 1 – patients who required PEG, but no tracheostomyMean%-change (SD) in OrSAT score---+5.83% (20.2)--4Type 1 – patients who required PEG and tracheostomyMean%-change (SD) in OrSAT score---0.00%--Cho et al.2023 [108]ROS21Type 11–4≤3y2.3y[SD: 4.6]Improvement in swallowing and speech--20---Nusinersen,onasemnogene abeparvovec,risdiplamZang 2023 [29]POS10Type 122.0m(0.0–7.0)3.8m(0.7–8.9)Murray secretion scale: median score21.5----OrSAT median score3.53----Studies with a Type 2/3 SMA populationNusinersenSHINE–CHERISH [74]SA119Type 2/3*NRNR**NR*PASA – tube feeding2.5----1.7(3.7y)Brakemeier2021 [109]POS22Types 2/33 to ≥6NR38.5y [SD: 14.2] (20–72)SSQ bulbar sub score – mean (SD)23.6 (18.9)n = 1824.1 (19.3)n = 15---20.0 (17.9)(n = 13, 14m)ALSFRS-R bulbar sub score – mean (SD)10.5 (1.2)n = 1610.5 (1.3)n = 20---10.9 (1.0)(n = 18, 14m)Cho et al.2023 [108]ROS103Type 21–4≤3 years15.4y[SD: 10.0]Improvement in swallowing/speech--5---Vetlesen2024 [57]POS40Types 2/32–4NR7.2y(2.4–12.7)EK2 – feeding difficulty^c^-----65(3y)EK2 – difficulties with food textures^c^-----37.5(3y)EK2 – prolonged mealtimes^c^-----42.5(3y)EK2 – swallowing difficulties^c^-----22.5(3y)20Type 23/4NR7.0y(2.0–12.9)Feeding difficulty^c^-----85(3y)EK2 – difficulties with food textures^c^-----50 (3y)EK2 – prolonged mealtimes^c^-----65 (3y)EK2 – swallowing difficulties^c^-----35%(3y)20Type 32–4NR8.4y(4.3–12.2)EK2 – feeding difficulty^c^-----45(3y)EK2 – difficulties with food textures^c^-----25(3y)EK2 – prolonged mealtimes^c^-----20(3y)EK2 – swallowing difficulties^c^-----10(3y)DEVOTE(Part A)Finkel 2023 [110]SA6Type 33/419.5m(8–36)9.4y(6.1–12.6)PASA score: not able to eat as much as would like3.5--3.7 (302d)-3.7 (64d)3.7 (269d)PASA score: had to suction excess saliva or drool4--4 (302d)-4 (64d)4 (269d)PASA score: not able to eat food variety they like3.8--3.7 (302d)-3.7 (64d)3.7 (269d)PASA score: had difficulty feeding themselves3.3--3.5 (302d)-3.5 (64d)3.5 (269d)PASA score: cough/clear throat - swallow liquid food4--4 (302d)-4 (64d)4 (269d)PASA: gagged or choked on liquid food4--4 (302d)-4 (64d)4 (269d)PASA: refused liquid food4--4 (302d)-4 (64d)4 (269d)PASA: retching/vomiting when drinking liquids4--4 (302d)-4 (64d)4 (269d)PASA: taken >30 minutes to drink liquids4--4 (302d)-4 (64d)4 (269d)PASA: difficulty swallowing soft foods4--4 (302d)-4 (64d)4 (269d)PASA: difficulty swallowing solid foods3.8--3.8 (302d)-3.8 (64d)3.8 (269d)PASA: experienced or shown pain when eating4--4 (302d)-4 (64d)4 (269d)PASA: gagged or choked on solid food3.8--4 (302d)-3.8 (64d)3.8 (269d)PASA: has taken >30 minutes to eat solids3.0--3.3 (302d)-3.0 (64d)3.2 (269d)PASA: refused solid foods3.8--4 (302d)-3.8 (64d)3.7 (269d)PASA: retching/vomiting when eating solids3.7--3.8 (302d)-3.7 (64d)3.8 (269d)PASA: had difficulty swallowing pills3.7--3.8 (302d)-4 (64d)4 (269d)PASA: required food to be cut up2.8--3.5 (302d)-3.5 (64d)3.5 (269d)PASA score: beentube fed4--4 (302d)-4 (64d)4 (269d)PASA score: concern unable to eat as much as like1.3--2.5 (302d)-2.6 (64d)1.6 (269d)PASA score: concern unable to eat variety as like1.5--2.8 (302d)-2.5 (64d)1.8 (269d)PASA score: concerned about my child’s weight0.8--2.0 (302d)-2.0 (64d)1.5 (269d)PASA score: concerned about swallowing ability2.0--2.8 (302d)-2.8 (64d)1.6 (269d)PASA score: concerned about variety of foods eaten1.3--2.0 (302d)-2.5 (64d)1.8 (269d)PASA score: concerned about aspirating food2.0--3.0 (302d)-2.8 (64d)2.0 (269d)PASA: concerned about choking when eating1.8--3.0 (302d)-2.8 (64d)2.0 (269d)PASA score: concerned about not getting goodness from diet1.0--2.8 (302d)-2.1 (64d)1.8 (269d)RisdiplamZoppi 2022 [75]POS6Types 2/3NRNR40y (22–25)Reported a subjective benefit with bulbar function-----100(FU: 6–21 m)Ñungo Garzόn 2023 [76]EAP6Type 21, 3, 4NRNREK2 – bulbar function score4.33 (mean)4 (median)-3.5 (mean)3 (median)---ALSFRS-R –bulbar function score7.83 (mean)8.5 (median)-10.5 (mean)10.5 (median)---Brakemeier2024 [77]POS25Types 2/32/3NR34.3 [11.3] (19–58)SSQ bulbar sub score – mean (SD)19.5 (16.4)n = 24-15.6 (18.6)n = 19--17.4 (16.9)n = 23 (4m)SSQ bulbarsub score –improved--83--64 (4m)SSQ bulbarsub score –unchanged--0--9 (4m)SSQ bulbarsub score –declined--17--27 (4m)ALSFRS-R bulbarsub scoremean (SD)10.1 (1.3)n = 24-10.4 (1.5)*n *= 17--10.3 (1.7)n = 22 (4m)ALSFRS-R –improved--4741 (4m)ALSFRS-R –unchanged--3541 (4m)ALSFRS-R –declined--1818 (4m)Sitas 2024 [78]ROS15Type 22–42.0y(0.5–18)30y(18–65)JFLS – mouth opening limitations indicative of TMJ contracture100----60 (2.5y)JFLS – swallowing difficulties86.7-----JFLS –improvement in swallowing-----20 (2.5y)16Type 3JFLS – swallowing difficulty12.5-----31Type 2/3INQoL – swallowing improvement-----26.7(2.5y)Studies in a mixed SMA populationNusinersenOsredkar2021 [64]POS61Types 1–32–4NRType 15.2y(0.2–14.7)Type 28.9y(0.8–18.8)Type 312.6y(1.9–18.6)Improvement in aspirations-----3.3 (14m)Improvement in feeding-----26.2 (14m)Improvement in salivation-----0 (14m)RisdiplamGomez Garcia de la Banda 2022 [111]ROS15Types 1–3NRNRNRImprovement in swallowing-----6.67 (≥12m)Nusinersen, onasemnogene abeparvovecOnasemnogene abeparvovec + nusinersen (combo therapy)D’Silva2022 [112]POS21Unclear2, 327d(9–329)^b^11m(0.65–24)OrSAT: normal oral and swallowing abilities^d^66.7----71.4 (15m)OrSAT: moderate impairment: supplemental nutrition required (NG, nasojejunal, or gastrostomy tube)^d^4.7----9.5 (15m)OrSAT: all nutrition and hydration via non-oral means^d^28.5----19.0 (15 m)Abbreviations: ALSFRS-R, Revised Amyotrophic Lateral Sclerosis Functional Rating Scale; d, days; DMT, disease-modifying therapy; EAP, expanded access programme; EK2, Egen Klassifikation Scale Version 2; INQoL, Individualised Neuromuscular Quality of Life questionnaire; IQR, interquartile range; JFLS, Jaw Functional Limitation Scale; m, months; NG, nasogastric; NR, not reported; OrSAT, Oral and Swallowing Abilities Tool; PASA, Parent Assessment of Swallowing Ability; PEG, percutaneous endoscopic gastrostomy; POS, prospective observational study; ROS, retrospective observational study; SA, single arm; SD, standard deviation; SMA, spinal muscular atrophy; SMN, survival of motor neuron; SSQ, Syndey Swallow Questionnaire; TMJ, temporomandibular joint; w, weeks; y, years^a^ Values are percentages of patients (N), unless otherwise stated. Timepoint refers to time on treatment, unless specified^b^ Parents disagreed/strongly disagreed with the PASA statements^c^ Feeding difficulties are defined as scoring >0 in EK2 total score or within the individual EK2 function domains^d^ The OrSAT was applied through retrospective analysis of patient records. No mention of patient reportClinical trials are in italics
Oral intake status
Presymptomatic SMA
Results from six publications indicate that most patients, regardless of SMN2 copy number and treatment type, were taking full oral nutrition at the last follow-up (range: 5.9–50.1 months). All studies investigating outcomes after onasemnogene abeparvovec and risdiplam reported that 100% of infants had full oral intake at the last timepoint (12–24 months of age) [21–23, 34]. Studies of nusinersen reported mixed results, with the proportion of infants taking full oral nutrition ranging from 84–100% after 19.4–50.1 months of treatment [35, 36].
Symptomatic SMA
In patients with Type 1 SMA treated symptomatically, the proportions of patients requiring full or partial nutritional support ranged from 14 to 100% at study endpoint (range of follow-up: 2–48 months) [4, 25]. With nusinersen, over 50% (range: 56–100%) of patients required alternative nutrition at the last study timepoint in all reported studies (range of follow-up: 6–48 months), and the need for tube feeding increased over time in most studies that had longitudinal data (77%, 10/13) [15, 24, 37–40, 43, 44, 46, 47]. With onasemnogene abeparvovec, less than 50% (range:15–46%) of patients required alternative nutrition at the last study timepoint (range of follow-up: 3–24 months) [25, 26] and in six studies with longitudinal results, 50% reported stability in feeding status after treatment initiation. With risdiplam, the proportion of infants able to feed orally was stable over 24 months of treatment; however, there was an increase from baseline in the proportion of patients who received supplemental nutritional support (29% vs. 20%) [28, 55].
Eight observational studies reported oral feeding status in patients with Types 2 and/or Type 3 SMA; six studies reported longitudinal data over a duration of 6.1–38 months. Overall, the proportion of patients reported to require a feeding tube was low in this population. No patients with Type 3 SMA were reported to require feeding support. However, three studies reported rates of tube feeding after treatment to be 5 and 33% in Type 2 SMA [57, 58] and 7.4% in a mixed Types 2/3 SMA population [59] after 3 years, 7.8 months, and 38 months, respectively. In one study of onasemnogene abeparvovec, all patients with Type 2 SMA could feed orally after a median 6.1 months of treatment [60]. Out of five studies reporting longitudinal data for nusinersen, all but one reported that swallowing and feeding ability was stable over the duration of follow-up (range: 6.1–38 months) [57, 58, 61, 62].
Twenty-one publications reported data from populations with a mixed or unclear SMA type, with a follow-up ranging from 6 months to 8 years. In populations treated with nusinersen, the proportions of patients requiring feeding support generally increased over time (range: 6–38 months) [58, 63–67]. With onasemnogene abeparvovec, all publications reported with longitudinal data showed stabilisation or improvement in oral feeding status over 12–33.3 months of treatment [32, 68–72]. No publications reported data from mixed populations treated with risdiplam.
Patient-/caregiver-reported outcomes
Fifteen publications from 14 studies were identified that used patient-/caregiver-reported measures to assess swallowing (Table 4).
Presymptomatic SMA
The only study in presymptomatic SMA reporting caregiver-reported assessments investigated nusinersen, with swallowing evaluated using the PASA general feeding section. Five years after treatment, 67% of children with two SMN2 copies, and all children with three SMN2 copies, were consuming all nutrition by mouth, with 76% of caregivers indicating that they did not have concerns about their child choking during eating [36].
Symptomatic SMA
Outcomes amongst children with Type 1 SMA suggest that the magnitude of underlying bulbar deficits at the time of treatment may influence treatment outcomes. In an investigation of the effect of nusinersen on OrSAT scores, Berti et al. found none of the children who relied on a tube for nutrition and tracheostomy for ventilation at baseline (n = 4) exhibited improvement in OrSAT score after 18 months of treatment [73]. This was in contrast with children who at baseline solely required a tube for nutrition (no tracheostomy; n = 4), who all exhibited numerical improvement in OrSAT score ranging from 1 to 6 points post-nusinersen; however, it is important to note that these improvements were not robust enough to facilitate full oral nutrition in any of the cases. Similarly optimistic results were observed amongst children without the need for tube nutrition at baseline (n = 12): these children generally maintained or improved their OrSAT score, and 83% maintained the ability to swallow, with no need for tube feeding after 18 months [73].
Five studies reported patient-/caregiver-reported bulbar outcomes with nusinersen in Types 2 and 3 SMA after 2 months to 3.7 years of treatment. Of four investigations reporting pre- and post-treatment assessments, studies demonstrated that patients generally maintained baseline swallowing integrity. One study reported improvements in swallowing and speech in 5% of patients after 1 year of treatment and in one study a reduction was reported in the proportion of patients being identified by the PASA general feeding score as being tube fed from baseline to 3.7 years of follow-up (2.5% vs. 1.7%) [74].
Similar findings, suggesting maintenance or improvement in bulbar integrity for patients with Type 2 or 3 SMA, were found after 1–2.5 years of treatment with risdiplam [75–78]. Interestingly, the proportion of individuals exhibiting improvement was highly variable within and across studies, ranging from 20 to 100% [75, 78]. This was in part dependent on the outcome used, with nearly twice as many patients from the same study reporting bulbar improvement on the Sydney Swallow Questionnaire than on the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale (47% vs. 83%) [77].
Discussion
Progressive impairment of swallowing physiology and function has historically been reported amongst patients spanning the SMA severity spectrum [3–6]. These deficits pose substantial risks to respiratory and nutritional health and are of great detriment to quality of life [3, 4]. Despite the significance of swallowing impairments, little is known regarding the effect of DMTs on feeding and swallowing in SMA.
Although we identified 72 studies that evaluated bulbar outcomes after DMTs in this review, nearly all were observational studies, and 32% (23 of 72) of studies did not collect bulbar status both pre- and post-treatment. These limitations significantly restrict our ability to draw conclusions regarding the effects of DMTs on bulbar outcomes. Additionally, the heterogeneity, and often questionable validity of the bulbar outcomes that were used, further convoluted the interpretation of results within and across investigations.
Nearly all investigations evaluated bulbar outcomes using functional swallow outcomes, such as oral intake status, and patient-reported outcomes. Whilst functional swallowing outcomes are of substantial clinical relevance and it is crucial that they are evaluated, they are subject to limitations in their sensitivity as they are dependent on a myriad of personal and clinical variables that may not pertain to a patient’s underlying bulbar integrity. For example, when considering oral feeding status, it is commonly appreciated in the field of dysphagia that recommendations to utilise alternative nutrition such as a gastrostomy tube, implement compensatory strategies such as thickened liquids, or cease oral intake altogether are subjective, and the decision of when to initiate an intervention is highly dependent on the evaluating provider. Additionally, oral feeding status may naturally evolve over time as patients age. Infants with bulbar deficits are more likely to receive alternative nutrition as they age due to the demonstrated persistence of problems throughout a wait-and-see period that eventually warrants intervention from their care team. As these infants continue to age and become less fragile, many caregivers decide to reinitiate some oral feeds for the infant’s enjoyment.
Additionally, patient-reported outcomes are also based on the perception of impairments that rely on an individual comparing their current function to their prior ability. It becomes even more challenging to assess swallowing function in others, particularly in young children who may not be able to articulate what they experience when swallowing.
Consequently, pairing these functional outcomes with more sensitive measures of physiology is critical in fully understanding bulbar integrity. We found that physiological instrumental assessments were rarely utilised within the identified studies, and when they were used, results were not reported using validated metrics. These findings highlight a lack of consensus within the medical community when it comes to the evaluation of bulbar integrity in SMA. Whilst the recent development of functional swallowing outcomes specific to patients with SMA hold promise in filling this gap moving forward [73, 79], true understanding of underlying integrity requires pairing these outcomes with measures of underlying physiology as is routinely done in the evaluation of motor control. Indeed, other recent studies outside of our search parameters have demonstrated that the inclusion of additional physiological measures such as lip and tongue strength and endurance and mouth opening can enable a comprehensive assessment of bulbar function impairments and track more subtle changes in function in SMA [80, 81].
Despite these limitations, our findings suggest that the majority of presymptomatic patients treated with DMTs achieve good swallowing outcomes, with most patients able to achieve full oral nutrition without profound functional deficits. This outcome is further supported by clinical and real-world data published after the data cut of our SLR [82, 83].
These data are encouraging, as previously, without treatment, almost all patients with Type 1 SMA would require exclusive tube feeding due to severe bulbar deficits [8, 84, 85]. Although these outcomes are promising, the aforementioned limitations in methods used to assess bulbar integrity warrant more cautious optimism. Patients consuming full oral nutrition can concurrently have profound swallowing deficits that pose functional limitations for eating efficiency, obtainment of appropriate nutrition, and respiratory health. To have functional swallowing integrity, an individual must not only have full oral nutrition but do so whilst maintaining good respiratory health [25]. Future investigations evaluating the ability of patients to achieve all swallowing endpoints necessary for full function are warranted.
In addition, though the majority of children treated before the onset of symptoms acquired full oral nutrition, not all children achieve these favourable outcomes, with some studies reporting that only 84% of patients achieved full oral nutrition. One theory for the mechanism contributing to this discrepancy is that in infants at risk of developing SMA, there is a clinically silent prodromal phase of disease progression in the late neonatal or early postnatal stage prior to the provision of DMT [86]. The potential for clinically silent, pre-treatment disease progression that may affect outcomes of DMTs warrants further investigation, as it has profound implications for managing caregiver expectations and exploring the safety and effectiveness of extending treatment initiation to the prenatal period [87].
The promising outcomes in patients treated prior to symptom onset are in strong contrast to bulbar outcomes amongst patients treated after symptoms have manifested. Identified studies suggest there is wide variability in bulbar outcomes within this patient population, with the proportion of patients obtaining full oral nutrition ranging from 0 to 86%. It is likely that much of the variability is attributable to differences in pre-treatment status.
Previous research in untreated patients with SMA revealed pathological changes in critical regulators of oropharyngeal swallowing physiology [88, 89]. Outcomes with DMTs are dependent on the composition of the motor neuron pool when treatment is initiated and the extent of the neuronal damage, which are heavily affected by the severity of SMA and disease duration. As such, patients who have deficits in key neural regulators of swallowing at treatment onset are not necessarily anticipated to experience improvements after treatment, but instead, may experience maintenance of baseline function. Results from this review indicate mixed results relating to the ability to maintain bulbar function in patients treated after symptom onset, with variables that influence outcomes including severity of deficits at baseline as well as the type of outcome being reported. Furthermore, patients with profound impairments at baseline, such as those requiring full alternative nutrition, have reached the floor of most assessment scales, and therefore will likely demonstrate maintenance of function at follow-up due to low prognosis for improvement. In contrast, scales are able to capture changes in patients who have more mild–moderate impairments at treatment initiation, such as those who consume some oral nutrition but receive supplemental nutrition by tube.
Although the heterogeneity in bulbar outcomes limited the ability to draw robust conclusions about DMT effects, it is plausible that other treatment-related factors, such as pharmacodynamics and pharmacokinetics, as well as the biodistribution/transduction of a drug within the body, may also influence how bulbar function responds to treatment. Tissue-dependent concentration of nusinersen in autoptic samples from five patients suggested that nusinersen distribution is rostro-caudal, with less distribution to motor neurons in the brainstem than to lumbar and thoracic segments of the spinal cord [90]. In a study by van der Heul et al. in patients treated with nusinersen, this was hypothesised as being implicated in a suboptimal bulbar treatment response [4]. Conversely, both onasemnogene abeparvovec and risdiplam have shown extensive distribution throughout and beyond the central nervous system (CNS), supporting a potentially favourable outcome of these DMTs on bulbar function in SMA. A study examining post-mortem tissue samples after treatment with onasemnogene abeparvovec demonstrated widespread homogeneous distribution of vector genomes and transgenes throughout the CNS, and increased SMN protein levels in the brainstem [91]. Further studies are required more specifically to determine the number and types of cells transduced in these regions, as, although neurons are at least one major target, liver vector genomes demonstrated a 300–1,000-fold increase in transduction over the CNS [91]. In a study by Poirier et al., a homogeneous distribution of risdiplam was observed throughout the CNS, plasma and peripheral tissues in three different animal species, with similar penetration observed in the brain stem and cortex regions via the blood–brain barrier [92]. The distribution is expected to be the same in humans given the same mechanistic rationale [93]. It is important to interpret this biodistribution data with caution as they originate from heterogeneous and limited sources. More research is needed to confirm these observations, but future research should consider this as a possible prognostic factor influencing bulbar function treatment response.
Conclusions
Our findings suggest:
- The ability to draw conclusions on the effects of DMTs on swallowing is limited by the use of heterogeneous functional swallowing outcomes across the literature, and that studies frequently did not collect information about pre-treatment bulbar integrity.
- Patients treated with DMTs prior to symptom onset typically have good feeding and swallowing outcomes.
- Swallowing and feeding outcomes amongst patients treated with DMTs after symptom onset appear largely dependent on the level of impairment at baseline.
- It is plausible that other treatment-related factors, such as pharmacodynamics and pharmacokinetics, as well as the biodistribution/transduction of a drug within the body, may also influence how bulbar function responds to treatment; however, more evidence and further observations would be needed to confirm these aspects.
Our findings highlight the need for future investigations to systematically evaluate both physiological and functional aspects of bulbar integrity to allow stronger conclusions to be drawn regarding the effects of DMTs.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU technical support document, 2: a generalised linear modelling framework for pairwise and network metanalysis of randomised controlled trials. 2014. Available from:https://www.ncbi.nlm.nih.gov/books/NBK 310366/. [Cited March 2025].27466657 · pubmed ↗
- 2Agency for Healthcare Research and Quality (AHRQ). Assessing the risk of bias of individual studies when comparing medical interventions. Available from: https://effectivehealthcare.ahrq.gov/sites/default/files/assessing-the-risk-of-bias_draft-report.pdf. [Cited March 2025].
- 3Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The newcastle-ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available from: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. [Cited March 2025].
- 4Chiang J, Xiao L, Nigro E, St-Laurent A, Weinstock L, Law E, et al. Sleep disordered breathing in infants identified through newborn screening with spinal muscular atrophy. Sleep Med. 2023;111161–69.10.1016/j.sleep.2023.09.01937778092 · doi ↗ · pubmed ↗
- 5Crawford TO, Swoboda KJ, De Vivo DC, Bertini E, Hwu WL, Finkel RS, et al. Continued benefit of nusinersen initiated in the presymptomatic stage of spinal muscular atrophy: 5-year update of the NURTURE study. Muscle Nerve. 2023;68(2):157–70.10.1002/mus.2785337409780 · doi ↗ · pubmed ↗
- 6Sansone VA, Pirola A, Albamonte E, Pane M, Lizio A, D’Amico A, et al. Respiratory needs in patients with type 1 spinal muscular atrophy treated with Nusinersen. J Pediatr. 2020;219:223–8.e 4. 10.1016/j.jpeds.2019.12.04732035635 · doi ↗ · pubmed ↗
- 7Chen K-A, Widger J, Teng A, Fitzgerald DA, D’Silva A, Farrar M. Real-world respiratory and bulbar comorbidities of SMA type 1 children treated with nusinersen: 2-year single centre Australian experience. Paediatr Respir Rev. 2021;39:54–60. 10.1016/j.prrv.2020.09.00233129670 · doi ↗ · pubmed ↗
- 8Tokatly Latzer I, Sagi L, Lavi R, Aharoni S, Bistritzer J, Noyman I, et al. Real-life outcome after gene replacement therapy for spinal muscular atrophy: a multicenter experience. Pediatr Neurol. 2023;144:60–68.10.1016/j.pediatrneurol.2023.04.00737149951 · doi ↗ · pubmed ↗