Perspectives of Physical Therapists in Saudi Arabia on radiological interpretation: attitudes, engagement, and educational needs
Samia A. Alamrani, Ali H. Alghamdi, Ahmad A. Alharbi, Hamad S. Al Amer, Abdulaziz A. Albalwi, Aisha I. Alasiri, Ibrahim E. Alfaifi

TL;DR
This study explores how physical therapists in Saudi Arabia engage with radiological interpretation, their attitudes, and their need for more education in this area.
Contribution
The study provides insights into the current practices and educational needs of physical therapists in Saudi Arabia regarding radiological interpretation.
Findings
46.1% of PTs reported frequent involvement in radiological interpretation.
83.0% of PTs believed radiological interpretation should be part of their professional role.
PTs with less involvement were four times more likely to express interest in further education.
Abstract
Radiological imaging is essential in clinical practice to support diagnosis and treatment planning. As Physical Therapists (PTs) increasingly collaborate within multidisciplinary teams, their ability to interpret radiographs has become more relevant. In Saudi Arabia, limited data exist concerning the involvement of PTs in radiological interpretation. Therefore, this study aimed to explore PTs’ engagement with radiological information, assess their attitudes, and examine the factors influencing their involvement in and interest in imaging education. This cross-sectional descriptive study employed a self-structured questionnaire to gather data on demographics, professional characteristics, practice patterns, learning sources, perceived barriers, and attitudes. Chi-square tests were used to assess associations, and binary logistic regression was used to identify predictors of interest in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
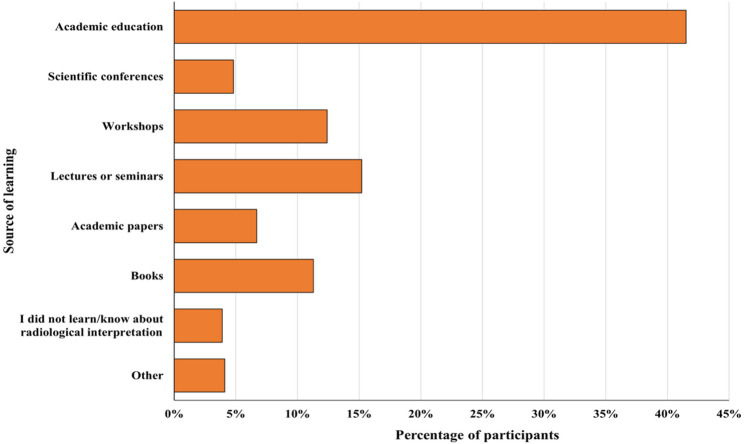 Figure 1
Figure 1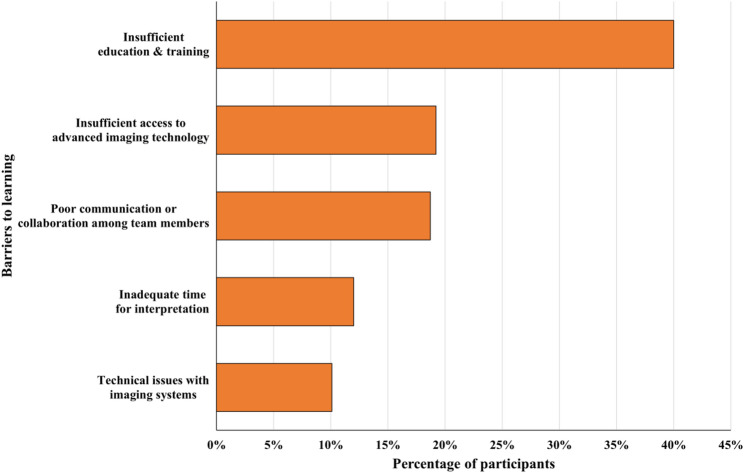 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiology practices and education · Clinical Reasoning and Diagnostic Skills · Innovations in Medical Education
Background
Radiological interpretation is an essential skill in modern clinical practice, supporting accurate diagnosis, guiding therapeutic decision-making, and promoting effective interdisciplinary collaboration [1, 2]. Interpretation of radiological images is usually the exclusive domain of physicians, radiologists, and diagnostic radiographers. However, the evolving scope of practice for Physical Therapists (PTs) in regions such as Saudi Arabia is reshaping standard boundaries in healthcare [3–5, 5]. This emerging clinical responsibility has stimulated growing interest in the competencies, accountability, and educational readiness of PTs regarding radiological interpretation. Previous studies have explored the integration of imaging into physical therapy education and practice, highlighting its potential to enhance clinical decision-making and improve patient outcomes. In some settings, this integration has helped PTs make more appropriate referrals by enabling them to better recognize when further imaging or medical consultation is needed [6–9]. The focus has largely been on referral patterns and regulatory frameworks, with the identified barriers including limited formal training in diagnostic imaging, inconsistent access to continuing education, and legal or institutional constraints [8]. Nonetheless, there remains a notable gap in the literature concerning the extent to which PTs actively engage in the interpretation of radiological images and how they perceive their role in this domain.
The importance of radiological interpretation in physical therapy practice is multifold. First, accurate interpretation of diagnostic images can lead to more precise treatment planning, especially for musculoskeletal conditions where incidental variations in imaging findings may influence therapeutic approaches [1, 10]. Second, as physical therapy practice in Saudi Arabia evolve toward greater autonomy, there is a growing need for professionals to develop competencies to determine the need for imaging and to interpret findings that inform clinical reasoning and patient management [5, 8]. Third, the integration of radiological interpretation into physical therapy practices may help reduce delays in patient management, thereby improving patient outcomes and reducing overall healthcare costs [6, 11].
For PTs managing orthopedic or movement-related conditions, timely radiological interpretation can increase care efficiency and reduce diagnostic delays, particularly in direct access or primary care models [4, 9, 12]. Globally, there is increasing momentum toward incorporating imaging competencies into physical therapy education and professional standards [13, 14]. Research from different countries has demonstrated that PTs can competently interpret certain types of radiological images when provided with appropriate training and guidelines [15, 16]. These developments have been supported by professional bodies such as the American Physical Therapy Association (APTA) and the Australian Physiotherapy Association (APA), both of which have recognized advanced imaging competencies and established pathways for advanced practice roles e.g. APTA Imaging Special Interest Group (I-SIG) [17]. However, there are substantial variations in the extent of the integration and acceptance of such practices between nations, institutional policy, and local scope-of-practice regulations [17, 18].
As healthcare systems in the region move toward greater efficiency and interdisciplinary care [19–21], understanding the current status of radiological competencies among PTs is vital for informing policy, curriculum development, and continuing education. In Saudi Arabia, physical therapy is a rapidly expanding profession, yet little is known about PTs’ engagement with radiological interpretation, their perceptions of its relevance, or the barriers that may limit their involvement. Moreover, no national-level data have been published to explore the frequency with which Saudi PTs contribute to radiograph interpretation or the factors that may influence these practices. A deeper understanding of these dimensions is essential for aligning professional competencies with modern clinical demands and advancing the quality of physical therapy care.
Study aims
This study was designed to explore PTs’ engagement with radiological interpretation and assess their attitudes toward interpreting radiographs. Additionally, it aimed to examine the demographic and professional factors associated with their contribution to and interest in radiological interpretation and related educational activities.
Methods
Study design and ethical considerations
A cross-sectional descriptive design was chosen because it allows for the collection of data at a single point in time to explore existing attitudes, engagement levels, and associated factors among PTs. This approach is ideal for identifying prevalent characteristics and associations within the targeted population without manipulating variables or observing long-term trends. Ethical approval to conduct the study was obtained from the Local Research Ethics Committee at the University of Tabuk (UT-505-313-2025). Participants were informed that participation was voluntary, and they could withdraw at any time without consequences. All procedures were conducted in accordance with the ethical standards of the Declaration of Helsinki.
Participants
Participants were recruited via a convenience sampling approach from different regions and professional sectors (public and private) in Saudi Arabia. On the basis of an estimated population of approximately 7,000 licensed PTs in the country [22], a sample size of 365 was calculated via Raosoft^®^ software , with a 95% confidence level and a 5% margin of error. Eligible participants included Saudi licensed PTs holding a recognized certificate in physical therapy, while physical therapy students, interns, and retired professionals were excluded.
Informed consent
Electronic informed consent was obtained from all participants prior to completing the survey. An online information sheet was provided, detailing the study’s purpose, procedures, potential benefits and risks, and measures taken to ensure confidentiality. Consent was indicated by selecting the “agree” option on the electronic form. Participants were also given the opportunity to contact the research team via email to ask questions or seek clarification before providing their consent.
Data collection procedure
Data collection was carried out between January 5, 2025, and May 2025, over a period of approximately 4 months. Participant invitations were distributed via institutional emails, professional networks, and social media platforms commonly used by PTs in Saudi Arabia, including X, LinkedIn, and WhatsApp professional groups. No incentives were offered for participation. The data were collected using a self-developed questionnaire specifically designed for this study, which was administered through the Google Forms platform. The full questionnaire is available in the Supplementary material (Appendix A).
The questionnaire consisted of three parts. The first part collected demographic information including sex, age, and region of practice. The second part focused on work-related characteristics such as qualifications, years of experience, workplace setting, and areas of specialization. The third part included items assessing PTs’ engagement with radiological interpretation, sources of learning, perceived barriers, attitudes toward the role of PTs in radiograph interpretation, and interest in related educational activities. The clarity and relevance of the questionnaire were assessed by a panel of 14 healthcare professionals including PTs and radiologists, via the item-level content validity index (I-CVI), the average scale-level content validity index (S-CVI/Ave), and the universal agreement index (S-CVI/UA) . The questionnaire was rated as clear and relevant, as illustrated in Table 1.
Table 1. Results of the content validity evaluation of the questionnaire used in the study (n = 14)VariableClarityRelevanceNumber of Items with I-CVI ≥ 0.7066Number of Items with I-CVI < 0.7000Minimum–Maximum I-CVI0.93-1.000.93-1.00S-CVI/Ave0.980.99S-CVI/UA0.670.83I-CVI item-level content validity index, S-CVI/Ave average scale-level content validity index, S-CVI/UA universal agreement
As shown in Table 1, all the items scored above the minimum I-CVI threshold of 0.70, with results ranging from 0.93 to 1. This suggests that the items are both clear and relevant according to expert panel. The S-CVI/Ave scores also support this, showing strong agreement overall—0.98 for clarity and 0.99 for relevance. Additionally, the S-CVI/UA values indicate a high degree of consensus among the reviewers, further reinforcing the tool’s overall content validity.
Data analysis
Statistical analyses were performed to assess participants’ frequency of contribution and attitudes toward radiograph interpretation. For the purpose of this study, the term “contribution and attitudes toward radiograph interpretation” was defined as any form of PTs' involvement in utilizing or applying radiological findings within clinical practice. This included: (i) discussing imaging findings with radiologists or referring physicians; (ii) reviewing and integrating information from radiology reports to guide assessment, clinical reasoning, and treatment planning; and (iii) using imaging findings to adjust management strategies or to support patient education and shared decision-making. Due to the structure of the dataset, it was not possible to distinguish precisely between these different forms of engagement; however, all were captured under the general category of “contribution and attitudes toward radiograph interpretation.”
The analyses also examined how demographic and professional characteristics were associated with frequent contributions and agreement with PTs interpreting radiographs. Additionally, the relationships between contribution frequency, beliefs, and interest in radiological interpretation and education were explored. For analysis purposes, “Never”, “Rarely”, “Often”, and “Always” responses on the frequency of radiological interpretation were recoded into “Rarely” and “Frequently”, respectively, whereas “Strongly disagree”, “Disagree”, “Agree”, and “Strongly agree” responses on attitudes toward radiograph interpretation were grouped into “Disagree” and “Agree”, respectively.
Chi-square tests were used to assess differences in contribution frequency and attitudes toward radiograph interpretation. When significant, pairwise comparisons were performed to identify specific group differences. Chi-square tests were also applied to evaluate the associations between demographic and professional characteristics and (1) frequent contributions to radiological interpretation and (2) agreement that PTs should interpret radiographs. Finally, binary logistic regression analyses were conducted to assess the relationships between contribution frequency, beliefs, and interest in radiological interpretation and education, with the results reported as odds ratios (ORs) and 95% confidence intervals (CIs). A sensitivity analysis was also conducted to examine the robustness of the logistic regression findings using alternative categorizations of key variables. For this purpose, “Rarely” and “Sometimes” responses for contribution frequency were combined and compared with “Frequently,” and “Disagree” and “Neutral” responses for attitudes toward radiograph interpretation were combined and compared with “Agree.” Logistic regression models were re-run using these alternative groupings to evaluate the direction or significance of the associations changed. All analyses were conducted using IBM SPSS Statistics for Windows, version 25.0 (Armonk, NY). Statistical significance was determined at an alpha level of 0.05.
Results
Participant characteristics
Table 2 summarizes the participants’ characteristics. A total of 241 PTs participated in the study. Of these, 54.8% were female, and 45.2% were male. Nearly half of the participants (49.8%) were aged 22–29 years, followed by 36.1% aged 30–39 years, 12.4% aged 40–49 years, and 1.7% aged 50–59 years. The participants were distributed across five regions in Saudi Arabia, with the highest representation from the central region (29.5%), followed by the northern (27.0%), southern (19.5%), western (16.2%), and eastern regions (7.9%). With respect to educational qualifications for physical therapy, the majority held a bachelor’s degree (68.0%), whereas others reported holding a master’s degree (12.0%), a doctoral degree (12.0%), a doctor of physical therapy degree (5.0%), or a diploma certificate (2.9%).
In terms of practice experience, approximately one-third (34.9%) had 1–5 years of experience, 20.3% had 6–10 years, 19.5% had 11–20 years, and 6.2% had over 20 years of experience. Approximately 19.1% had less than one year of experience. With respect to workplaces, 46.1% were employed in public hospitals or clinics, 35.7% were employed in private settings, 16.2% were employed in university-affiliated facilities, and 2.1% were unemployed. The most common area of specialization was general physical therapy (55.2%), followed by orthopedic (21.6%), pediatric (7.5%), neurological (5.0%), sports (4.1%), chest (2.1%), and geriatric (2.1%). Approximately 2.5% reported other specialties including women’s health, oncology, lymphoedema, and biomechanics or movement sciences.
Table 2. Characteristics of the participating PTs (n = 241)Characteristic n %Sex Male10945.2 Female13254.8Age 22–29 years12049.8 30–39 years8736.1 40–49 years3012.4 50–59 years41.7Practicing region in Saudi Arabia Central region7129.5 Western region3916.2 Eastern region197.9 North region6527.0 Southern region4719.5Qualification (physical therapy) Diploma certificate72.9 Bachelor’s degree16468.0 Doctor of physical therapy125.0 Master’s degree2912.0 Doctoral degree (PhD or equivalent)2912.0Experience < 1 year4619.1 1–5 years8434.9 6–10 years4920.3 11–20 years4719.5 > 20 years156.2Working place Public hospital/clinic/center11146.1 Private hospital/clinic/center8635.7 University hospital/clinic/center3916.2 Unemployed52.1Specialization (physical therapy) General13355.2 Orthopedic5221.6 Neurological125.0 Pediatric187.5 Geriatric52.1 Sports104.1 Chest52.1 Other62.5
Learning sources, barriers, and beliefs toward radiological interpretation
As shown in Fig. 1; Table 3, academic education was the most reported source of knowledge (41.5%), followed by lectures or seminars (15.2%), workshops (12.4%), books (11.3%), academic papers (6.7%), and scientific conferences (4.8%). A minority of participants reported not having learned about radiological interpretation (3.9%) or indicated other sources, such as clinical experience, guidance from a radiologist or physician, medical websites, coaching, self-learning, educational videos, or shadowing radiologists (4.1%).
Fig. 1. Sources of learning about radiological interpretation reported by participants
Table 3. Survey responses on learning sources, barriers, and beliefs toward radiological interpretation among the participating PTs (n = 241)Question n %How did you learn/know about radiological interpretation? * Academic education18041.5 Scientific conferences214.8 Workshops5412.4 Lectures or seminars6615.2 Academic papers296.7 Books4911.3 I did not learn/know about radiological interpretation173.9 Other184.1From your perspective, what are the factors that may limit the ability to conduct radiological interpretations effectively? * Insufficient education and training19040.0 Insufficient access to advanced imaging technology9119.2 Poor communication or collaboration among team members8918.7 Inadequate time for interpretation (limited staffing/heavy workload)5712.0 Technical issues with imaging systems (e.g., poor image quality)4810.1Are you interested in radiological interpretations? Yes21689.6 No2510.4Would you be interested in attending a lecture or hands-on seminar about radiological interpretation?Yes21990.9No229.1PTs Physical Therapists*Multiple responses were allowed for this item
The participants identified several barriers that may limit their ability to interpret radiological images effectively, as shown in Fig. 2. The most frequently reported barrier was insufficient education and training (40.0%), followed by a lack of access to advanced imaging technology (19.2%), poor communication or collaboration (18.7%), limited time due to staffing or workload (12.0%), and technical issues related to imaging systems (10.1%). Finally, 89.6% of the participants expressed interest in radiological interpretation, and 90.9% indicated that they would be interested in attending a related lecture or hands-on seminar.
Fig. 2. Factors reported by participants as barriers to effective radiological interpretation
Contribution frequency and attitudes toward radiograph interpretation
As presented in Table 4, statistically significant differences were observed in participants’ frequency of contribution to radiological interpretation. A total of 46.1% of the participants reported contributing frequently, 30.3% reported contributing sometimes, and 23.7% reported contributing rarely (p < 0.005). Pairwise comparisons revealed that those who contributed frequently were significantly more common than those who contributed rarely (p < 0.005) or sometimes (p = 0.005). No significant difference was found between those who contributed rarely or sometimes (p = 0.161).
With respect to attitudes toward the role of PTs in radiograph interpretation, 83.0% agreed that PTs should interpret radiographs, whereas 11.6% were neutral and 5.4% disagreed (p < 0.005). Pairwise comparisons indicated that agreement was significantly more common than both disagreement (p < 0.005) and neutrality (p < 0.005) while neutrality was also significantly more common than disagreement (p = 0.019).
Table 4. Main differences and pairwise comparisons of contribution frequency and attitudes toward radiograph interpretation (n = 241)Category n %p-valuePairwise comparisonp-valueFrequency of contribution to radiological interpretation Rarely5723.7< 0.005Rarely vs. Sometimes0.161 Sometimes7330.3Rarely vs. Frequently< 0.005 Frequently11146.1Sometimes vs. Frequently0.005PTs should interpret radiographs as part of their job Disagree135.4< 0.005Disagree vs. Neutral0.019* Neutral2811.6Disagree vs. Agree< 0.005* Agree20083.0Neutral vs. Agree< 0.005Note: Significant differences were examined via chi-square testsSignificant difference at α = 0.05
Factors associated with frequent contributions to radiological interpretation
As shown in Table 5, a significant proportion of both male (48.6%, p < 0.005) and female (43.9%, p = 0.032) participants reported frequently contributing to radiological interpretation. Regionally, participants from the Western (53.8%, p = 0.018) and Northern (47.7%, p = 0.041) regions demonstrated significantly high proportions of frequent contributions, whereas those from the Central, Eastern, and Southern regions did not show statistically significant percentages. Regarding qualifications, a significant proportion of bachelor’s degree holders (50.0%, p < 0.005) reported frequent contributions. In contrast, participants with diplomas, doctor of physical therapy, master’s degrees, or doctoral degrees did not report statistically significant proportions of frequent contributions.
Years of experience were also associated with contribution frequency. Participants with 1–5 years (46.4%, p = 0.039) and 6–10 years (51.0%, p = 0.004) of experience showed significant levels of frequent contribution, whereas those with less than 1 year, 11–20 years, or more than 20 years of experience did not. In terms of workplace, significant proportions of participants working in public (52.3%, p < 0.005) and private (46.5%, p = 0.034) settings reported frequent contributions. However, those employed at university-affiliated facilities or unemployed did not report significant proportions. Among areas of specialization, only participants practicing in general physical therapy reported a significant level of frequent contribution (47.4%, p = 0.002). The proportions of other specialties were not significantly different.
Table 5. Associations of demographic and professional factors with frequent contributions to radiological interpretation (n = 111)CharacteristicsProportion of participants who frequently contributed to radiological interpretation n %p-valueSexMale5348.6< 0.005Female5843.90.032Practicing region in Saudi ArabiaCentral2839.40.546Western2153.80.018Eastern947.40.368Northern3147.70.041Southern2246.80.067QualificationDiploma certificate114.30.102Bachelor’s degree8250.0< 0.005Doctor of physical therapy541.70.779Master’s degree1241.40.639Doctoral degree (PhD or equivalent)1137.90.786Experience< 1 year1941.30.3451–5 years3946.40.0396–10 years2551.00.00411–20 years2144.70.240> 20 years746.70.247Working placePublic hospital/clinic/center5852.3< 0.005Private hospital/clinic/center4046.50.034University hospital/clinic/center1230.80.794Unemployed120.00.449Primary area of specialization in physical therapyGeneral6347.40.002Orthopedic2446.20.138Neurological541.70.779Pediatric738.90.846Geriatric120.00.819Sports660.00.527Chest360.00.449Other233.30.607Note: Significant differences were examined via chi-square tests*Significant difference at α = 0.05
Factors associated with agreement with PTs interpreting radiographs
As shown in Table 6, a significant proportion of both male (84.4%, p < 0.005) and female (81.8%, p < 0.005) participants agreed that PTs should interpret radiographs as part of their professional role. Regionally, significant proportions of agreement were observed among participants from all five regions: western (89.7%, p < 0.005), southern (87.2%, p < 0.005), northern (83.1%, p < 0.005), central (78.9%, p < 0.005), and eastern (73.7%, p = 0.001) regions. With respect to qualifications, a significant proportion of bachelor’s degree holders (82.9%, p < 0.005) and participants with master’s (89.7%, p < 0.005) or doctoral degrees (82.8%, p < 0.005) agreed that PTs should interpret radiographs. In contrast, agreement was not statistically significant among participants with a diploma or doctor of physical therapy degree.
Work experience was also associated with agreement levels. A significant proportion of participants with less than 1 year (78.3%, p < 0.005), 1–5 years (79.8%, p < 0.005), 6–10 years (87.8%, p < 0.005), 11–20 years (85.1%, p < 0.005), or more than 20 years of experience (93.3%, p = 0.001) agreed that PTs should interpret radiographs. With respect to workplace setting, significant agreement was observed among participants working in public (87.4%, p < 0.005), private (80.2%, p < 0.005), and university hospitals (76.9%, p < 0.005). In terms of specialization, significant proportions of agreement were found among those in general (82.0%, p < 0.005), orthopedic (86.5%, p < 0.005), pediatric (83.3%, p < 0.005), neurological (75.0%, p = 0.009), and sports (90.0%, p = 0.011) specialties. All participants in the chest and “other” categories (100%) agreed with PTs interpreting radiographs.
Table 6. Associations of demographic and professional factors with agreement with PTs interpreting radiographs (n = 200)CharacteristicsProportion of participants who agree that PTs should interpret radiographsn%p-valueSexMale9284.4< 0.005Female10881.8< 0.005Practicing region in Saudi ArabiaCentral5678.9< 0.005Western3589.7< 0.005Eastern1473.70.001North5483.1< 0.005Southern4187.2< 0.005QualificationDiploma certificate571.40.257Bachelor’s degree13682.9< 0.005Doctor of physical therapy975.00.083Master’s degree2689.7< 0.005Doctoral degree (PhD or equivalent)2482.8< 0.005Experience< 1 year3678.3< 0.0051–5 years6779.8< 0.0056–10 years4387.8< 0.00511–20 years4085.1< 0.005> 20 years1493.30.001Working placePublic hospital/clinic/center9787.4< 0.005Private hospital/clinic/center6980.2< 0.005University hospital/clinic/center3076.9< 0.005Unemployed480.00.180Primary area of specialization in physical therapyGeneral10982.0< 0.005Orthopedic4586.5< 0.005Neurological975.00.009Pediatric1583.3< 0.005Geriatric240.00.655Sports990.00.011Chest5100.0ConstantOther6100.0ConstantNote: Significant differences were examined via chi-square testsSignificant difference at α = 0.05
Relationships among practice, beliefs, and engagement with radiological interpretation
Table 7 presents the results of the binary logistic regression examining the relationships among contribution frequency, attitudes, and participants’ interest in radiological interpretation as well as their willingness to attend educational activities. When participants who frequently contributed to radiological interpretation were used as the reference group, those who rarely contributed were significantly more likely to express interest in radiological interpretation (OR = 4.0, p = 0.007). However, no significant difference in interest was observed among participants who contributed occasionally (p = 0.621). Similarly, participants who contributed rarely or occasionally did not show a significant association with interest in attending a lecture or seminar about radiological interpretation (p = 0.192 and 0.265, respectively).
With respect to attitudes and the use of participants who disagreed with the role of PTs in interpreting radiographs as a reference, those who agreed were approximately seven times more likely to express interest in radiological interpretation (OR = 7.6, p = 0.003). Furthermore, the likelihood of expressing interest in attending a lecture or hands-on seminar was also significant among those who agreed (OR = 5.7, p = 0.018). No significant associations were observed for the neutral group regarding interest in radiological interpretation or attendance at educational activities (p = 0.756 and 0.554, respectively).
The results of the sensitivity analysis using the alternative coding schemes confirmed the magnitude and direction of key relationships (Appendix B.). For frequency of contribution, the effect of rare contribution on interest in radiological interpretation remained elevated and in the same direction (OR = 2.4), although with a slightly higher p-value (p = 0.062). For attitudes toward radiograph interpretation, participants who agreed that PTs should interpret radiographs also expressed a high interest in radiological interpretation (OR = 8.9, p < 0.005). A similar pattern was observed for interest in attending a lecture, where the association remained high and robust (OR = 7.9, p < 0.005).
Table 7. Logistic regression analysis for the relationships among contribution frequency, beliefs, and interest in radiological interpretation and education (n = 241)AttributeInterested in radiological interpretationsInterested in attending a lecture or seminar on radiological interpretationYes (%)No (%)OR (95% CI)p-valueYes (%)No (%)OR (95% CI)p-valueFrequency of contribution to radiological interpretationRarely45 (78.9%)12 (21.1%)4.0 (1.5–10.7) 0.00750 (87.7%)7 (12.3%)0.5 (0.2–1.4)0.192Sometimes67 (91.8%)6 (8.2%)1.3 (0.4–4.1)0.62165 (89.0%)8 (11.0%)0.5 (0.2–1.6)0.265Frequently104 (93.7%)7 (6.3%)1-104 (93.7%)7 (6.3%)1-PTs should interpret radiographs as part of their jobDisagree9 (69.2%)4 (30.8%)1-10 (76.9%)3 (23.1%)1-Neutral18 (64.3%)10 (35.7%)0.8 (0.2–3.3)0.75619 (67.9%)9 (32.1%)0.6 (0.1–2.9)0.554Agree189 (94.5%)11 (5.5%)7.6 (2.0-28.7) 0.003190 (95.0%)10 (5.0%)5.7 (1.4–24.0) 0.018OR odds ratio, CI confidence intervalSignificant at α = 0.05
Discussion
This study provides a comprehensive national perspective from Saudi Arabia on PTs’ engagement, attitudes, and educational interests in radiological interpretation. It addresses a notable gap in the literature regarding the extent to which PTs actively engage in interpreting radiological images and their perceptions of their role in this area. This shows that the majority of PTs (83%) feel that interpreting radiographs should be part of their professional responsibilities. Nearly half of the respondents (46%) reported some level of involvement in radiological interpretation, though the specific activities and their clinical impact warrant further clarification. Additionally, more than 90% indicated that they would be interested in receiving additional training on the subject. The findings demonstrate a significant level of engagement and notable interest in radiological interpretation.
Despite academic education being the most frequently reported source of knowledge (41.5%), the most cited barrier to effective radiological interpretation was insufficient education and training (40.0%). This reveals a gap between academic education and the practical training required for radiological reasoning in clinical practice. While academic programs may cover theoretical aspect of radiological assessment, they often provide limited opportunities for students to apply these concepts to real patients’ cases [23, 24]. Previous studies have similarly reported that many PTs feel uncertain about when diagnostic imaging is appropriately indicated and how to interpret imaging findings within their clinical scope. These difficulties were primarily attributed to inadequate formal training (32%). Additionally, 69% of PTs reported that they require mentorship and support from other professionals [7].
In Saudi Arabia, PTs’ ability to make independent radiological decisions may be restricted by institutional or regulatory constraints [4, 8]. This discrepancy between formal education and the competencies required in practice, highlights the need to revise curricula to align with current clinical standards [14]. For instance, a recent Delphi study indicated that PTs in critical care are expected to understand pathophysiology, interpret radiographs, and carry out functional assessments [25], Currently, physical therapy curricula provide only limited and variable training in diagnostic and procedural imaging. While some programs include imaging education, the scope, depth, and integration of such training differ considerably between institutions, and there is no consistent standard across curricula [14, 23]. This variability highlights the need for more consistent and comprehensive imaging education to better prepare PTs for evolving clinical roles. This could include the introduction of modules on radiological evaluation, interdisciplinary teaching approaches, along with practical workshops on imaging interpretation during clinical rotations.
The high level of interest (89.6%) and willingness (90.9%) to attend educational activities related to radiological interpretation suggest strong motivation to enhance competencies in this area. However, an interesting and inconsistent finding revealed that PTs who rarely contributed to radiological interpretation were significantly more likely to express interest in further training than those who frequently contributed (OR = 4.0, p = 0.007). This may indicate a lack of confidence, limited institutional support or access to imaging systems, or legal and professional barriers rather than a lack of motivation [8]. These findings point to the utility of personalized and flexible educational approaches such as modular training, case-based learning or mentorship-driven models, especially for under-engaged practitioners [26]. Furthermore, the use of digital platforms and simulation technologies such as 3D virtual reality [27], or real-time interactive X-ray simulation [28] in clinical education may facilitate learning, promote self-paced engagement and improve diagnostic reasoning skills [29]. These strategies can also help address geographic differences by offering remote learning opportunities, especially for practitioners in rural regions.
The frequency of contribution to radiograph interpretation was significantly associated with several factors, including sex, region, educational level, years of experience, workplace setting, and area of specialization. Mid-career professionals (with 1–10 years of experience) and those working in public or private settings were more likely to contribute frequently, possibly reflecting greater clinical responsibility and routine exposure to imaging. Notably, general physical therapy was the only specialty significantly associated with frequent contributions, suggesting a potential need for greater imaging exposure and training in other subspecialties, such as neurology and pediatrics, where imaging interpretation may still be limited or delegated. This is consistent with previous studies showing that PTs with an orthopedic caseload of 50% or more (p < 0.001) and those working in the private sector (p < 0.001) demonstrated greater interest in ordering radiographs [7].
The attitudes toward radiograph interpretation were positive, with 83.0% of the participants agreeing that PTs are interested in radiograph interpretation. This agreement was consistently distributed across different regions, qualifications, and levels of experience, reflecting a growing interest in the evolving diagnostic contribution of PTs within interprofessional care teams. Notably, PTs who supported this role were significantly more likely to express interest in training and active engagement, highlighting an empirically supported link between professional attitudes and motivation for skill development.
To translate this interest into safe and effective clinical practice, national stakeholders, including professional bodies and educational institutions, should prioritize the integration of imaging competencies into undergraduate and postgraduate curricula such as blended learning and simulation. This integration could follow competency-based education that define measurable learning outcomes [30], such as understanding imaging modalities, applying clinical decision rules, and interpreting common radiological findings. Blended learning approaches, combining online theoretical modules with face-to-face practical workshops, can enhance accessibility and accommodate diverse learning needs. Furthermore, simulation-based education can provide realistic, risk-free environments for experimental learning and skill improvement [31].
Additionally, there is a clear need for continuing professional development programs that are accessible and standardized, ensuring upskilling across the profession. Developing clear guidelines on scope of practice and legal responsibilities can further support PTs in safely applying imaging interpretation within clinical settings. Future research should focus on the design, implementation and evaluation of educational interventions that address the training gap, particularly for underrepresented subgroups. It is also important to investigate how PTs’ interpretative skills influence referral patterns, cost effectiveness, and patient safety to support broader and systemic changes in training and practice policies.
Despite its valuable findings, this study has several limitations that should be considered. First, the use of convenience sampling may limit the generalizability of our findings to the broader physical therapy workforce in Saudi Arabia. Second, as a cross-sectional study, it can identify associations but cannot establish causal relationships between the examined factors and PTs’ attitudes or involvement in radiological interpretation. Although associations were found, it is impossible to determine whether these relationships are directional or temporal. However, the study offers important baseline data that identify practice patterns and potential research areas. To address these limitations, future research should aim to include larger samples and implement the longitudinal or experimental research designs to explore causal pathways. Additionally, validation methods such as comparing self-reported practices with direct observation, chart audits, or case-based performance assessments could strengthen future evaluations of PTs’ imaging related competencies. Finally , the measure of “engagement with radiological information” did not distinguish between different forms of involvement—such as collaborative discussion of imaging findings, integration of radiology reports into clinical reasoning, or informal reference to imaging during patient management. Consequently, the reported frequencies may reflect a range of engagement rather than distinct levels of interpretive responsibility. Future studies should examine these dimensions more precisely, using objective methods such as structured case vignettes, scenario-based assessments, or observational designs to clarify the nature and extent of PTs’ engagement with radiological information.
Conclusion
This study highlights the growing interest and positive attitudes of PTs in Saudi Arabia toward radiological interpretation, despite the notable gap between academic preparation and clinical demands. While many PTs report academic education as their primary source of radiological knowledge, inadequate training remains a key barrier to effective clinical application. The findings emphasize the need to update physical therapy curricula, expand access to continuing professional development, and establish clear professional guidelines to support the safe and effective integration of imaging into practice. Addressing these areas may improve clinical decision-making and diagnostic accuracy and empower PTs to meet the evolving demands of modern healthcare systems.
Supplementary Information
Supplementary Material 1: Appendix A. PDF (Study questionnaire).
Supplementary Material 2: Appendix B. PDF (Results of sensitivity analysis).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mabry LM, Severin R, Gisselman AS, Ross MD, Davenport TE, Young BA. Physical therapists are routinely performing the requisite skills to directly refer for musculoskeletal imaging: an observational study. J Man Manip Ther. 2022;30(5):261–72. 10.1080/10669817.2022.2106729.10.1080/10669817.2022.2106729 PMC 948795635968741 · doi ↗ · pubmed ↗
- 2Oakley PA, Cuttler JM, Harrison DE. X-ray imaging is essential for contemporary chiropractic and manual therapy spinal rehabilitation: radiography increases benefits and reduces risks. Dose-Response. 2018;16(2). 10.1177/1559325818781437.10.1177/1559325818781437 PMC 602428329977177 · doi ↗ · pubmed ↗
- 3Burton SO, Donovan JK, Jones SL, Meadley BN. Can non-physician providers use ultrasound to aid in establishing peripheral IV access in patients who are difficult to cannulate? A scoping review. Prehosp Disaster Med. 2022;37(4), Article 4.10.1017/S 1049023 X 22000796 PMC 928006435593145 · doi ↗ · pubmed ↗
- 4Mabry LM, Aaron K, ,Brian Y, Reilly A, Nicholas, Ross, Michael D., Gisselman, Angela Spontelli,and, Goss D. Physical therapist awareness of diagnostic imaging referral jurisdictional scope of practice: an observational study. J Man Manip Ther. 2024;32(4):435–445. 10.1080/10669817.2023.2296260.10.1080/10669817.2023.2296260 PMC 1125700238130076 · doi ↗ · pubmed ↗
- 5Asmri MA, Almalki MJ, Fitzgerald G, Clark M. The public health care system and primary care services in Saudi arabia: a system in transition. East Mediterr Health J. 2020;26(4). 10.26719/emhj.19.049.10.26719/emhj.19.04932338366 · doi ↗ · pubmed ↗
- 6World Physiotherapy Annual Membership Census. World Physiotherapy. 2023. https://world.physio/sites/default/files/2024-01/AMC 2023-Saudi-Arabia.pdf.
- 7Baxi G, Palekar T.Competency-based physiotherapy education. Indian J Phys Therapy Res. 2020;2(2). https://journals.lww.com/ijpt/fulltext/2020/02020/competency_based_physiotherapy_education.13.aspx.