Reversible sick sinus syndrome due to sinus node artery ischaemia in an elderly woman: a case report
Yuji Kaneko, Tatsuro Hitsumoto, Masato Tada, Takuya Shimura, Akira Itoh

TL;DR
An elderly woman's reversible sick sinus syndrome was caused by sinus node artery ischaemia, which was treated with coronary intervention.
Contribution
This case report highlights ischaemia as a reversible cause of sick sinus syndrome, emphasizing the need for coronary evaluation before pacemaker implantation.
Findings
Sinus node dysfunction due to ischaemia can be reversible with percutaneous coronary intervention.
Elderly patients with multiple coronary risk factors may present with atypical ischaemic signs.
Early coronary evaluation can avoid unnecessary pacemaker implantation in select cases.
Abstract
Sick sinus syndrome often necessitates permanent pacemaker implantation; however, when sinus node artery ischaemia is the cause, sinus node dysfunction may be reversible. While age-related fibrosis is generally considered the main mechanism, ischaemia should also be recognized as a potential aetiology. An 80-year-old woman with breast cancer, hypertension, and diabetes mellitus presented with dyspnoea. Electrocardiography showed marked bradycardia at 38 beats per minute (b.p.m.) without ST-segment changes. Chest radiography revealed a cardiothoracic ratio of 61% with mild pulmonary congestion, and echocardiography showed preserved left ventricular ejection fraction (>60%) without wall motion abnormality. Although referred for pacemaker implantation, the acute onset of severe bradycardia together with multiple coronary risk factors prompted coronary angiography, which demonstrated 99%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
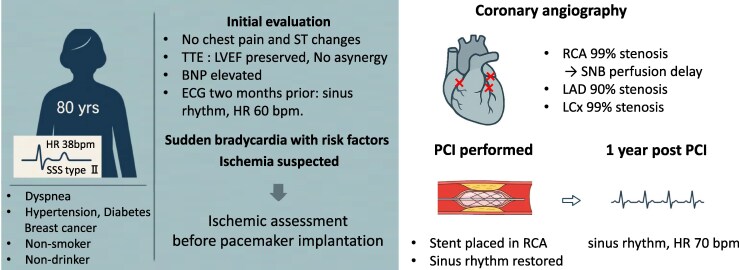 Figure 1
Figure 1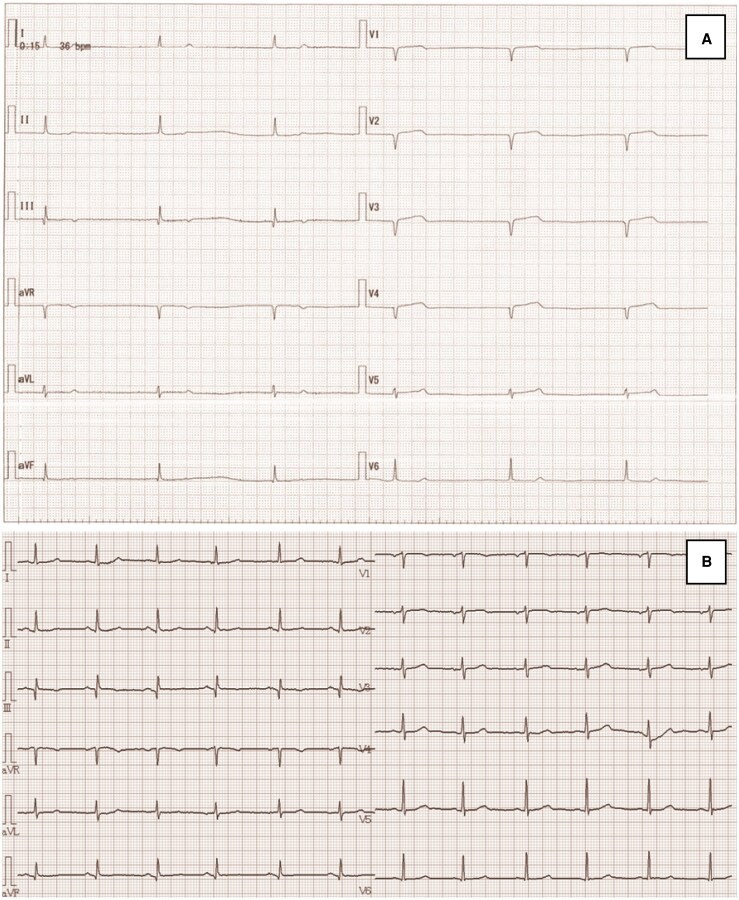 Figure 1
Figure 1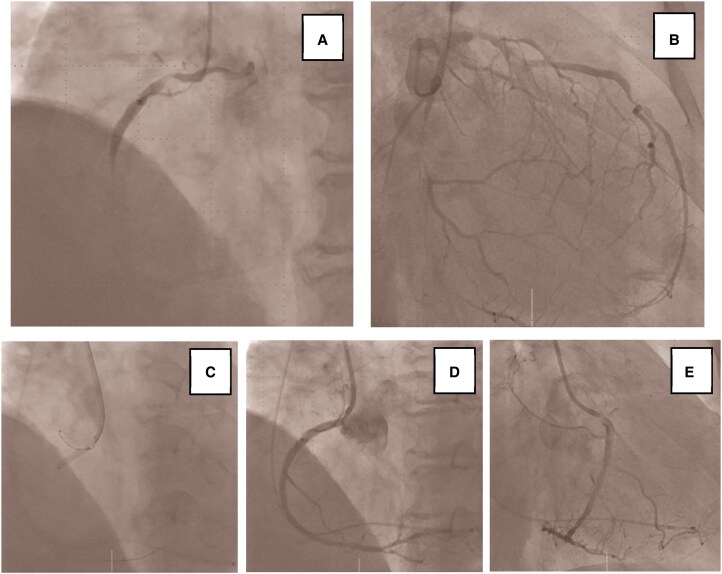 Figure 2
Figure 2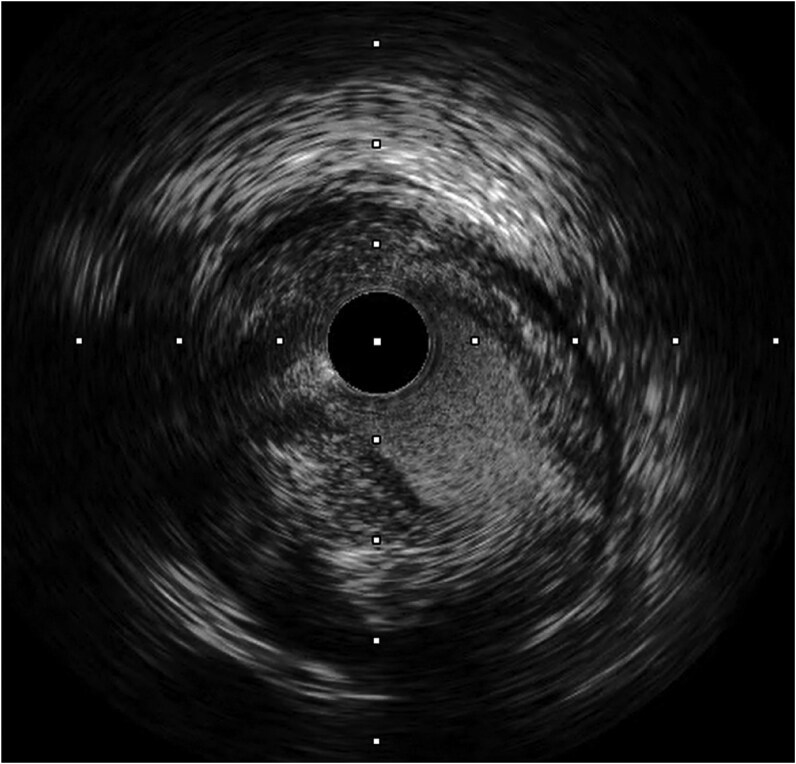 Figure 3
Figure 3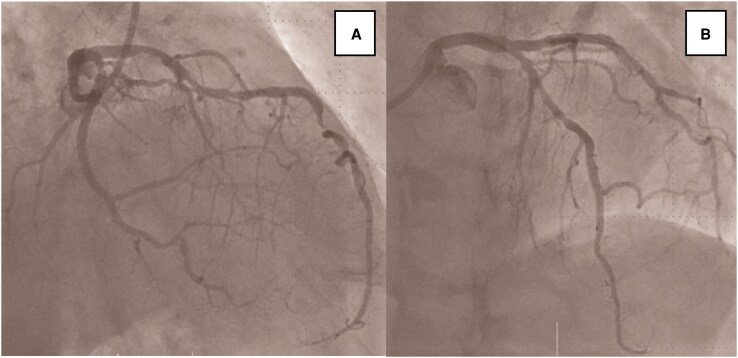 Figure 4
Figure 4| Parameter | Result | Reference range |
|---|---|---|
| RBC | 385 × 10⁴/µL | 380–480 × 10⁴/µL |
| Hb | 11.4 g/dL | 11.5–15.0 g/dL |
| Ht | 34.7% | 34–45% |
| WBC | 8400/µL | 3500–9000/µL |
| Plt | 25.1 × 10⁴/µL | 15–35 × 10⁴/µL |
| Blood glucose | 139 mg/dL | 70–109 mg/dL |
| HbA1c | 5.5% | 4.6–6.2% |
| AST | 34 U/L | 10–35 U/L |
| ALT | 41 U/L | 5–45 U/L |
| BUN | 17.8 mg/dL | 8–20 mg/dL |
| Creatinine | 0.96 mg/dL | 0.46–0.82 mg/dL |
| T-Cho | 169 mg/dL | 120–219 mg/dL |
| HDL-C | 38 mg/dL | ≥40 mg/dL |
| LDL-C | 110 mg/dL | 60–139 mg/dL |
| TG | 100 mg/dL | 30–149 mg/dL |
| TP | 6.3 g/dL | 6.5–8.2 g/dL |
| CK | 94 U/L | 40–150 U/L |
| CK-MB | 2.6 ng/mL | <5 ng/mL |
| Na | 141 mmol/L | 138–146 mmol/L |
| K | 4.2 mmol/L | 3.6–4.8 mmol/L |
| Cl | 107 mmol/L | 101–108 mmol/L |
| Ca | 9.4 mg/dL | 8.5–10.2 mg/dL |
| C-reactive protein | 0.29 mg/dL | <0.30 mg/dL |
| TSH | 0.73 mIU/L | 0.61–4.23 mIU/L |
| T3 | 2.65 pg/mL | 1.68–3.67 pg/mL |
| T4 | 0.97 ng/dL | 0.70–1.48 ng/dL |
| PT-INR | 1.02 | 0.85–1.15 |
| APTT | 34.8 s | 25–40 s |
| D-dimer | 3.70 µg/mL | <1.0 µg/mL |
| BNP | 269.8 ng/mL | <18.4 ng/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Syncope and Autonomic Disorders · Cardiac pacing and defibrillation studies · Pathogenesis and Treatment of Hiccups
Introduction
Sick sinus syndrome (SSS) is a condition characterized by impaired sinus node function leading to bradycardia or sinus arrest and is one of the major indications for permanent pacemaker implantation in elderly patients. Although irreversible changes due to aging and fibrosis are generally considered the main causes, ischaemia of the sinus node branch (SNB) has also been reported as an aetiology.^1,2^ In such cases, relief of ischaemia may restore sinus node function, potentially allowing avoidance of pacemaker implantation.^3,4^
Most reports of sinus node dysfunction related to the SNB describe iatrogenic occlusion during percutaneous coronary intervention (PCI). By contrast, de novo ischaemia of the SNB causing severe bradycardia before any intervention is extremely rare. Recognizing this difference is important because it highlights the need for ischaemic evaluation in patients with unexplained bradycardia.
We report a case of severe bradycardia referred for pacemaker implantation. Coronary angiography (CAG) revealed multivessel disease, including severe proximal right coronary artery (pRCA) stenosis with delayed flow in the SNB. After PCI, sinus rhythm was restored, and permanent pacing was successfully avoided.
Summary figure
**
Case presentation
An 80-year-old woman developed dyspnoea in late December 2024, which gradually limited her daily activities. In January 2025, she visited a local physician, where marked bradycardia at 38 beats per minute (b.p.m.) was observed, and she was referred to our department of cardiology for pacemaker implantation.
Her past medical history included breast cancer, hypertension, and diabetes mellitus. Medications included letrozole for breast cancer, angiotensin receptor blocker, DPP-4 inhibitor, and proton pump inhibitor. She had no history of taking drugs associated with bradycardia. She had no history of smoking or alcohol consumption, and no family history of cardiac disease.
On admission, she was alert with a body temperature of 36.4°C, blood pressure of 99/49 mmHg, heart rate of 38 b.p.m., respiratory rate of 12 breaths/min, and SpO₂ 95% on 2 L oxygen supplementation. Jugular venous distension was absent. Heart sounds were regular without murmurs, and breath sounds were clear. There was no peripheral coldness, with only mild pretibial oedema.
Electrocardiography (ECG) revealed sinus arrest with a narrow QRS escape rhythm at 38 b.p.m., without ST-segment changes. There was no atrioventricular block or QT prolongation, and the escape rhythm had a narrow QRS configuration (Figure 1A). Chest radiography showed a cardiothoracic ratio of 61% with mild pulmonary congestion. Transthoracic echocardiography revealed preserved left ventricular ejection fraction (>60%) without regional wall motion abnormalities. Laboratory data showed elevated B-type natriuretic peptide (BNP) at 269.8 ng/mL, while cardiac enzymes were within normal ranges. Thyroid function and electrolytes were also within normal limits (Table 1).
(A) Pre-percutaneous coronary intervention electrocardiography showing sinus arrest with a ventricular rate of 38 b.p.m. and a narrow QRS escape rhythm, without ST-segment changes. (B) Electrocardiography at 1-year follow-up showing stable sinus rhythm with a heart rate of 70 b.p.m.
From these initial findings, there was no evidence of ischaemia, as chest pain, ST-segment changes, and ischaemic biomarkers were absent. An ECG obtained 2 months prior had documented sinus rhythm with a heart rate in the 60 b.p.m., suggesting relatively recent onset of bradycardia. Given her multiple coronary risk factors, including hypertension and diabetes mellitus, ischaemia was considered as a possible underlying cause. Therefore, instead of proceeding directly to pacemaker implantation, we decided to perform CAG.
Coronary angiography revealed 99% stenosis in pRCA, 99% in the proximal left circumflex artery (pLCx), and 90% in the mid left anterior descending artery (mLAD). Flow delay was observed in the SNB arising from the RCA (Figure 2A,B). Based on these findings, we concluded that sinus node dysfunction was due to ischaemia of the SNB. The initially scheduled pacemaker implantation was cancelled, and temporary pacing was established while PCI was prioritized.
(A) Coronary angiography revealed 99% stenosis of proximal right coronary artery, with delayed flow in sinus node branch (Supplementary material online, Video 2(A)). (B) Coronary angiography revealed 99% stenosis of proximal left circumflex artery and 90% stenosis of mid left anterior descending artery. (C) Deployment of a Xience Skypoint stent (3.5 × 15 mm) in proximal right coronary artery. (D, E) Following stent implantation, coronary angiography showed restoration of TIMI III flow in right coronary artery territory, including sinus node branch (Supplementary material online, Video (2E)).
Intravascular ultrasound of the pRCA demonstrated mixed plaque and thrombus, suggesting a relatively acute lesion (Figure 3). A Xience Skypoint stent (3.5 × 15 mm) was implanted in the pRCA (Figure 2C), achieving thrombolysis in myocardial infarction (TIMI) III flow in the RCA territory including the SNB (Figure 2D, E). Sinus rhythm with rates in the 50 s was restored during PCI. The temporary pacemaker was removed the following day, after which sinus rhythm was maintained and symptoms of heart failure improved.
Intravascular ultrasound findings of proximal right coronary artery. Intravascular ultrasound demonstrated a mixed plaque with both fibrous and lipid components and the presence of thrombus, suggesting a relatively acute lesion responsible for sinus node artery ischaemia (Supplementary material online, Video 3).
Subsequent staged PCI achieved complete revascularization with additional Orsiro stents (2.25 × 30 mm in the pLCx and 2.5 × 18 mm in the mLAD (Figure 4A, B). At 1-year follow-up, she remained in stable sinus rhythm at 70 b.p.m. (Figure 1B). During this period, she experienced no recurrence of bradycardia or symptoms. Permanent pacemaker implantation was successfully avoided, confirming the reversibility of sinus node dysfunction in this case.
(A) Orsiro stent (2.25 × 30 mm) was deployed in proximal left circumflex artery. (B) Orsiro stent (2.5 × 18 mm) was deployed in mid left anterior descending artery.
Discussion
This case showed a reversible type of SSS caused by coronary artery disease. After revascularization, sinus node function completely recovered. In most elderly patients, SSS is due to irreversible fibrosis or aging. However, when ischaemia of SNB is present, restoring blood flow can improve sinus node activity.^1–4^ Although ischaemia is estimated to account for <15% of SSS cases,^5–7^ reports directly demonstrating SNB ischaemia as the cause are rare. This makes our case unique because the ischaemia was observed before any coronary intervention and was not iatrogenic.
In this case, there were no typical ischaemic findings such as chest pain, ST-segment changes, or elevation of cardiac enzymes. Several mechanisms may explain this. First, flow impairment of the RCA was intermittent, preventing progression to severe ischaemia. Second, collateral circulation from the LCx to the SNB may have limited ischaemic severity. Interestingly, bradycardia itself has been reported to promote the development of collateral circulation.^8,9^ Gloekler et al.^10^ reported that ivabradine-induced heart rate reduction enhanced collateral function in patients with stable coronary artery disease. This adaptive mechanism may have masked ischaemic signs and contributed to the clinically silent presentation. Previous studies also reported that even when the SNB is occluded during PCI, nearly half of patients remain asymptomatic.^6^ Additionally, under a ventricular escape rhythm, abnormal repolarization can hide ischaemia-related ST changes, making diagnosis even more difficult.
The important implication of this case is that bradycardia is not always caused by irreversible disease; ischaemia may represent a reversible aetiology. In particular, when elderly patients present with acute-onset bradycardia and multiple coronary risk factors, ischaemia should be strongly suspected.
Revascularization should be performed before permanent pacemaker implantation, and sinus node recovery should be observed. This strategy avoids unnecessary device implantation and related complications, improving long-term quality of life. This approach is consistent with the ESC pacing guidelines, which recommend excluding reversible causes such as ischaemia before device implantation.^11^
This case highlights that even in patients referred for pacemaker implantation, underlying coronary artery disease may be present. For similar cases in the future, rather than proceeding directly to device implantation, thorough ischaemic evaluation is of great clinical importance. This case serves as an educational reminder that careful diagnostic reasoning, guided by clinical and angiographic evidence, is crucial even in apparently straightforward cases of bradycardia.
Conclusion
We reported an elderly woman with severe bradycardia caused by ischaemia of the SNB. After PCI, sinus rhythm recovered, and permanent pacemaker implantation was successfully avoided. This case demonstrates that even when typical ischaemic signs are absent, ischaemia should be considered as a reversible cause of bradycardia. Careful ischaemic evaluation before pacemaker implantation can prevent unnecessary procedures and improve patient outcomes.
Supplementary Material
ytaf660_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Semelka M, Gera J, Usman S. Sick sinus syndrome: a review. Am Fam Physician 2021;104:179–185.23939447 · pubmed ↗
- 2Patel S, Shah S, Velagapudi P, Shah M. Ischemia-related sinus node dysfunction reversed by PCI. Interv Cardiol 2018;10:37–38.
- 3Maeda S, Nishikawa K, Miyazaki H, Yoshino S, Sato M, Ikeda S. Recovery of sinus node function after revascularization. Cardiol Res 2022;13:172–176.35836732
- 4Seiler C . The human coronary collateral circulation. Coron Artery Dis 2000;11:467–472.10966132 10.1097/00019501-200009000-00004 · doi ↗ · pubmed ↗
- 5Ciulla MM, Astuti M, Carugo S. The atherosclerosis of the sinus node artery is associated with an increased history of supra-ventricular arrhythmias: a retrospective study on 541 standard coronary angiograms. Peer J 2015;3:e 1156.26336639 10.7717/peerj.1156 PMC 4556151 · doi ↗ · pubmed ↗
- 6Jariwala P, Gude D, Kulkarni GP, Jariwala A. Sino-atrial nodal artery occlusion causing acute sinus node dysfunction after percutaneous coronary intervention: case report and systematic review. Pacing Clin Electrophysiol 2024;47:1038–1048.38923028 10.1111/pace.15029 · doi ↗ · pubmed ↗
- 7Kyriakidis M, Trikas A, Triposkiadis F, Barbarousi M, Kremastinos DT. Sinus node dysfunction in acute inferior myocardial infarction: role of sinus node artery and clinical course in patients with one-vessel coronary artery disease. Cardiology 1997;88:166–169.9096918 10.1159/000177325 · doi ↗ · pubmed ↗
- 8Maseri A, Crea F, Kaski JC, Crake T. Mechanisms of ischemia without ST elevation. Arterioscler Thromb Vasc Biol 2005;25:2122–2127.16051883