Neurological Manifestations and High Viral Load as Independent Predictors of Mortality in Severe Fever With Thrombocytopenia Syndrome
Rujia Chen, Yutong Xing, Wei Wei, Yun Wang, Ting Wang, Renren Ouyang, Shiji Wu, Feng Wang, Hongyan Hou

TL;DR
This study finds that neurological symptoms and high viral load are key indicators of mortality in a severe tick-borne disease called SFTS.
Contribution
The study identifies neurological symptoms and viral load as independent predictors of mortality in SFTS patients.
Findings
Neurological symptoms are linked to higher mortality and elevated inflammatory markers in SFTS patients.
High viral load correlates with severe disease markers like coagulopathy and kidney dysfunction.
Immune profiles, including T-cell and B-cell changes, differ between survivors and nonsurvivors.
Abstract
Severe fever with thrombocytopenia syndrome (SFTS), an emerging tick-borne viral hemorrhagic fever, is characterized by high mortality rates. While neurological complications (eg, seizures, encephalitis) have been identified as adverse prognostic factors in severe cases, their association with viral replication, immune responses, and neuroinflammation remain poorly defined and urgently require systematic investigation. A cohort of 277 patients with SFTS was included and stratified based on neurological symptoms. Clinical characteristics, laboratory results, and immune markers were compared between groups. Neurological symptoms developed in 78 (28.2%) patients and were associated with significantly higher 28-day mortality. These patients had higher viral loads, elevated inflammatory cytokines (IL-6, IL-10, TNF-α, and ferritin), and more severe multi-organ dysfunction. Compared with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
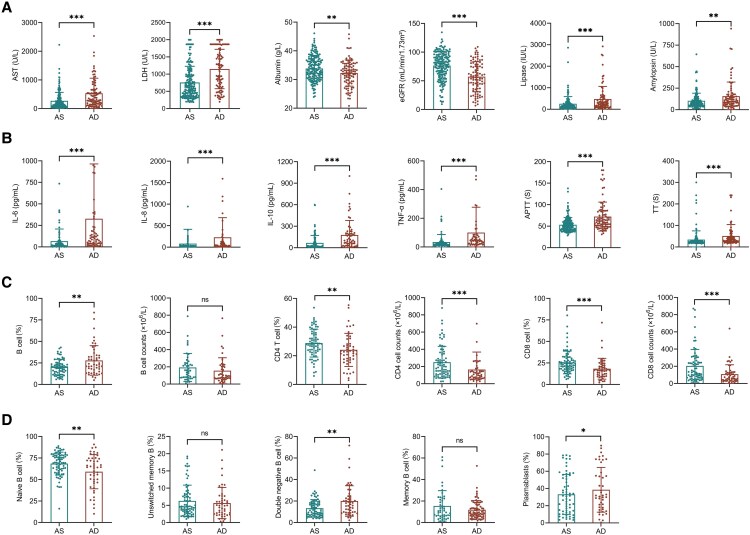 Figure 1
Figure 1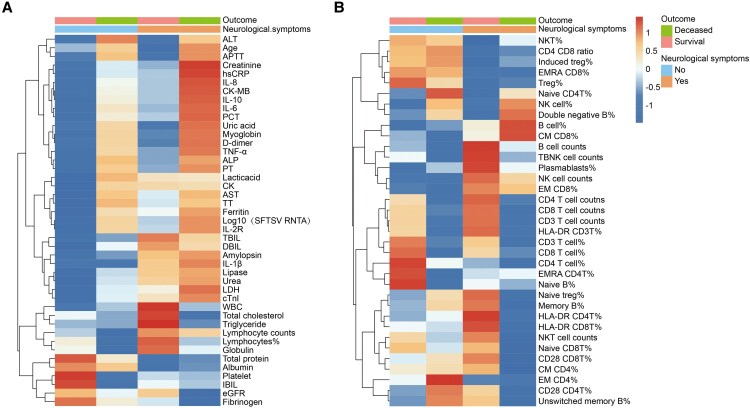 Figure 2
Figure 2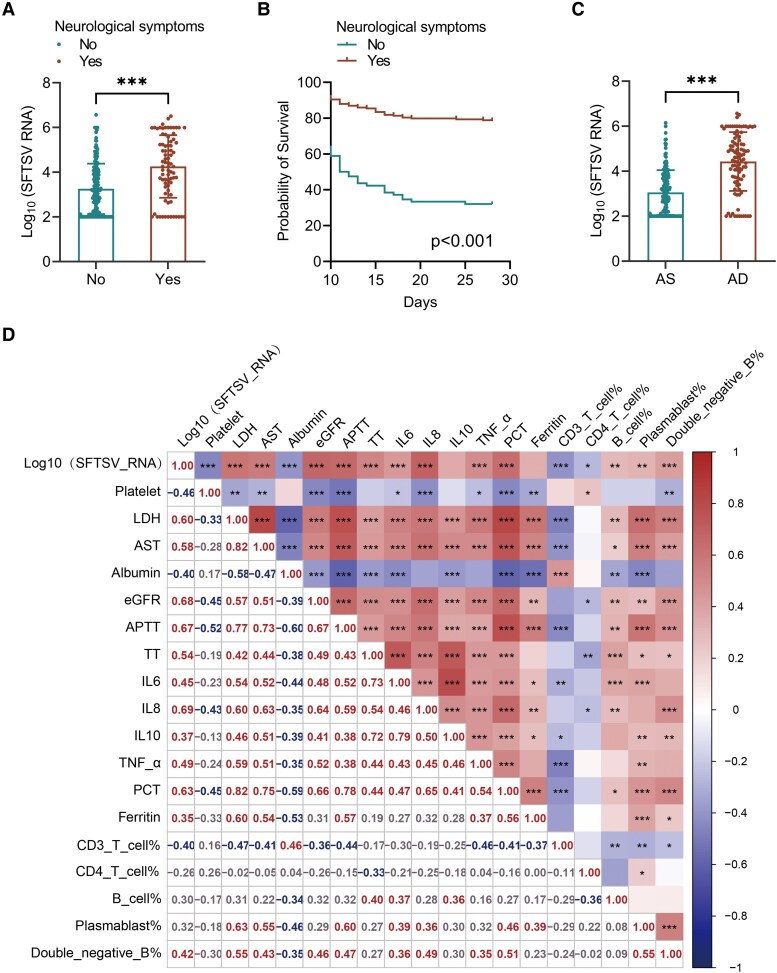 Figure 3
Figure 3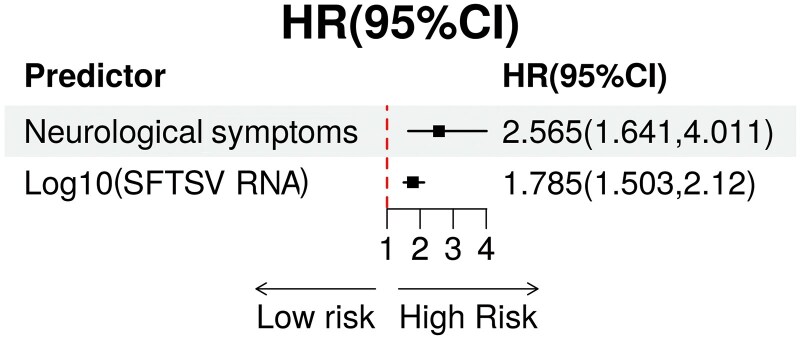 Figure 4
Figure 4| Parameters | Total (n = 277) | No Neurological Symptoms (n = 199) | Neurological Symptoms (n = 78) |
|
|---|---|---|---|---|
| Age, median [Q1–Q3] | 65.000 [57.000; 71.000] | 64.000 [56.000; 70.000] | 69.000 [61.000; 73.000] | .002 |
| Sex, n (%) | 1.000 | |||
| Female | 146 (52.708%) | 105 (52.764%) | 41 (52.564%) | |
| Male | 131 (47.292%) | 94 (47.236%) | 37 (47.436%) | |
| Outcomes, n (%) | <.001 | |||
| Survival | 181 (65.343%) | 156 (78.392%) | 25 (32.051%) | |
| Deceased | 96 (34.657%) | 43 (21.608%) | 53 (67.949%) | |
| Hemophagocytosis, n (%) | .001 | |||
| No | 173 (62.455%) | 137 (68.844%) | 36 (46.154%) | |
| Yes | 104 (37.545%) | 62 (31.156%) | 42 (53.846%) | |
| Hypertension, n (%) | .017 | |||
| No | 191 (68.953%) | 146 (73.367%) | 45 (57.692%) | |
| Yes | 86 (31.047%) | 53 (26.633%) | 33 (42.308%) | |
| Hormone usage, n (%) | .007 | |||
| No | 165 (59.567%) | 129 (64.824%) | 36 (46.154%) | |
| Yes | 112 (40.433%) | 70 (35.176%) | 42 (53.846%) | |
| Continuous renal replacement therapy, n (%) | <.001 | |||
| No | 231 (83.394%) | 178 (89.447%) | 53 (67.949%) | |
| Yes | 46 (16.606%) | 21 (10.553%) | 25 (32.051%) | |
| Invasive mechanical ventilation, n (%) | <.001 | |||
| No | 246 (88.809%) | 190 (95.477%) | 56 (71.795%) | |
| Yes | 31 (11.191%) | 9 (4.523%) | 22 (28.205%) | |
| D from symptom onset to admission, median (Q1–Q3) | 7.000 [5.000; 8.000] | 7.000 [5.000; 8.000] | 7.000 [5.000; 8.750] | .468 |
| Hospitalization time, median (Q1–Q3) | 7.000 [4.000; 11.000] | 8.000 [5.000; 11.000] | 5.000 [2.000; 10.000] | .002 |
| Parameters | Total (n = 277) | No Neurological Symptoms (n = 199) | Neurological Symptoms ( |
|
|---|---|---|---|---|
|
| ||||
| WBC (×109/L) | 3.5 [2.1; 6.0] | 3.2 [1.9; 5.5] | 3.7 [2.5; 6.9] |
|
| Lymphocyte counts (×109/L) | 0.7 [0.4; 1.0] | 0.6 [0.3; 1.0] | 0.8 [0.5; 1.0] |
|
| Lymphocytes % | 19.5 [12.1; 34.5] | 18.4 [11.9; 34.5] | 20.6 [12.3; 34.7] | .498 |
| Neutrophils (×109/L) | 2.4 [1.2; 4.2] | 2.1 [1.1; 3.9] | 2.8 [1.4; 5.0] | .052 |
| Neutrophils % | 73.4 [56.0; 84.3] | 73.9 [54.5; 84.3] | 71.0 [59.4; 83.3] | .904 |
| Platelet (×1012/L) | 50.0 [32.0; 68.0] | 50.5 [34.8; 69.0] | 42.5 [28.3; 65.8] | .061 |
| RBC (×1012/L) | 4.3 (0.7) | 4.3 (0.6) | 4.2 (0.8) | .429 |
| Hemoglobin (g/L) | 129.4 (21.2) | 130.0 (18.9) | 127.8 (26.3) | .513 |
|
| ||||
| ALT (U/L) | 86.0 [46.0; 167.0] | 81.5 [42.0; 159.3] | 99.0 [57.5; 182.5] | .099 |
| AST (U/L) | 209.0 [100.0; 476.0] | 187.0 [88.8; 419.0] | 279.0 [167.0; 633.5] |
|
| LDH (U/L) | 740.0 [442.0; 1278.0] | 641.5 [374.8; 989.3] | 1264.0 [669.5; 1856.5] |
|
| Globulin (g/L) | 27.9 [25.5; 30.4] | 27.6 [25.4; 30.2] | 28.4 [25.9; 30.6] | .289 |
| Albumin (g/L) | 33.3 (4.6) | 34.3 (4.2) | 30.8 (4.8) |
|
| TBIL (μmol/L) | 9.0 [6.3; 12.8] | 8.6 [6.2; 11.8] | 10.0 [6.7; 16.1] |
|
| IBIL (μmol/L) | 3.9 [2.3; 5.9] | 4.0 [2.5; 6.0] | 3.8 [1.9; 5.2] | .14 |
| DBIL (μmol/L) | 4.4 [3.0; 6.9] | 4.2 [2.9; 5.9] | 5.1 [3.7; 10.9] |
|
| HCO3− (mmol/L) | 19.8 [17.4; 21.8] | 20.3 [17.9; 22.0] | 18.1 [15.6; 20.5] |
|
| eGFR (ml/min/1.73 m2) | 73.9 [51.4; 90.5] | 79.2 [60.0; 92.6] | 56.2 [33.2; 78.7] |
|
| Creatinine (μmol/L) | 83.0 [66.0; 116.0] | 78.0 [63.5; 100.5] | 106.0 [74.5; 156.0] |
|
| Uric acid (μmol/L) | 262.0 [200.8; 351.0] | 251.0 [193.7; 329.0] | 303.5 [221.8; 439.0] |
|
| Urea (mmol/L) | 6.1 [4.4; 9.1] | 5.5 [4.0; 7.5] | 9.0 [5.9; 14.5] |
|
| Total cholesterol (mmol/L) | 3.1 [2.5; 3.6] | 3.1 [2.5; 3.6] | 3.0 [2.5; 3.7] | .993 |
| Triglyceride (mmol/L) | 2.0 [1.5; 2.8] | 2.0 [1.4; 2.6] | 2.3 [1.6; 3.6] |
|
| Lactic acid (mmol/L) | 1.9 [1.3; 2.7] | 1.6 [1.1; 2.6] | 2.2 [1.7; 2.8] |
|
| Myoglobin (ng/mL) | 226.3 [122.1; 510.1] | 195.1 [93.1; 370.3] | 364.3 [189.4; 962.5] |
|
| cTnI (pg/mL) | 107.3 [35.4; 314.4] | 58.8 [27.1; 165.2] | 244.0 [128.4; 851.5] |
|
| CK-MB (ng/mL) | 3.0 [1.4; 6.9] | 2.3 [1.2; 5.2] | 5.6 [2.8; 9.3] |
|
| CK (U/L) | 521.0 [199.0; 1288.0] | 420.0 [178.5; 1269.3] | 858.0 [401.0; 1415.0] |
|
| Lipase (IU/L) | 187.6 [97.0; 339.8] | 162.6 [95.6; 280.4] | 290.3 [133.7; 641.5] |
|
| Amylopsin (U/L) | 83.0 [53.0139.0] | 74.5 [50.0; 111.5] | 121.5 [84.5; 244.5] |
|
|
| ||||
| hsCRP (mg/L) | 4.6 [1.8; 12.9] | 3.2 [1.5; 8.7] | 10.1 [3.0; 26.9] |
|
| Ferritin (μg/L) | 9832.0 [3250.7; 23 291.3] | 6187.9 [2378.7; 15 991.0] | 20 048.0 [10 198.0; 45 839.0] |
|
| IL-1β (pg/mL) | 5.0 [5.0; 10.5] | 5.0 [5.0; 7.8] | 6.9 [5.0; 14.6] |
|
| IL-2R (U/mL) | 1217.5 [887.0; 1740.8] | 1045.5 [779.7; 1486.3] | 1684.0 [1127.0; 2335.0] |
|
| IL-8 (pg/mL) | 25.1 [14.275; 61.250] | 20.2 [13.1; 36.7] | 59.2 [23.2; 203.8] |
|
| IL-10 (pg/mL) | 47.7 [15.6; 151.0] | 27.4 [12.9; 86.0] | 139.5 [33.5; 227.0] |
|
| TGF-β1 (pg/mL) | 4.1 [2.6; 7.3] | 4.7 [2.7; 9.3] | 4.7 [3.4; 9.2] | .820 |
| TNF-α (pg/mL) | 24.2 [16.2; 45.1] | 21.3 [14.8; 32.9] | 42.7 [21.9; 82.7] |
|
| IL-6 (pg/mL) | 37.8 [12.7; 112.5] | 29.3 [10.6; 63.8] | 74.1 [33.7; 227.7] |
|
| PCT (ng/mL) | 0.3 [0.1; 0.7] | 0.2 [0.1; 0.5] | 0.7 [0.2; 1.9] |
|
|
| ||||
| APTT (S) | 54.2 [43.7; 65.2] | 52.2 [42.2; 62.8] | 56.6 [47.8; 76.8] |
|
| PT (S) | 12.8 [12.2; 13.5] | 12.800 [12.1; 13.5] | 13.0 [12.4; 13.9] | .051 |
| TT (S) | 24.6 [21.4; 37.1] | 23.600 [20.8; 30.1] | 30.4 [23.9; 49.9] |
|
| Fibrinogen (g/L) | 2.6 [2.2; 2.9] | 2.620 [2.3; 2.9] | 2.4 [2.0; 2.9] |
|
| D-dimer (μg/mL FEU) | 2.6 [1.5; 5.7] | 2.335 [1.3; 4.5] | 3.3 [2.2; 7.4] |
|
- —National Natural Science Foundation of China10.13039/501100001809
- —National Key R&D Program of China10.13039/501100012166
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Vectors · Viral Infections and Outbreaks Research · Vector-Borne Animal Diseases
Severe fever with thrombocytopenia syndrome (SFTS), caused by the SFTS virus (SFTSV), is an emerging tick-borne infectious disease first identified in rural China in 2009 [1]. Since then, SFTS has been reported in several countries across Asian, including South Korea, Japan, and Vietnam [2–4]. The disease typically presents with fever, thrombocytopenia, leukopenia, gastrointestinal symptoms, and, in severe cases, multiple organ dysfunction syndrome (MODS) [5]. From 2009 to 2019, SFTSV outbreaks resulted in more than 13 000 cases in mainland China and over 1000 cases in South Korea, with the mortality rate ranging from 12% to 30% [6–8]. Although the epidemiology and clinical manifestations of SFTS are increasingly documented, the mechanisms underlying its variable severity, particularly the role of central nervous system (CNS) involvement, remain insufficiently understood.
Patients with SFTS often exhibit dysregulated immune response and excessive inflammatory response [9]. This cytokine storm contributes to systemic inflammatory response syndrome, leading to vascular leakage, tissue damage, multiple organ dysfunction, and increased mortality rate [10]. Laboratory findings in patients with SFTS commonly include thrombocytopenia, leukopenia, elevated liver enzymes, and coagulation abnormalities [11, 12]. These parameters reflect both viral replication and immune-mediated damage. Hemophagocytic lymphohistiocytosis (HLH) is a life-threatening condition characterized by excessive activation of the immune system, leading to hemophagocytosis in bone marrow and other tissues [13]. This phenomenon contributes to pancytopenia and organ failure. Early recognition and management of HLH are vital to improving survival rates in patients with SFTS [14]. High viral loads, especially during the early stages of infection, are associated with severe disease manifestations [15]. Quantitative assessments of viral load can serve as prognostic indicators, aiding in early identification of patients at risk for adverse outcomes.
Neurological manifestations, such as seizures, cognitive impairment, and consciousness disorders, are increasingly recognized as critical factors influencing the prognosis of SFTS. Patients who develop encephalitis as a complications of SFTS face a mortality rate exceeding 50% [16]. Research has identified several risk factors for CNS complications, including elevated SFTSV RNA levels and lactate dehydrogenase (LDH) levels during the fever stage, both of which have been independently associated with increased risk of severe neurological outcomes [17, 18]. In addition, studies have shown elevated levels of pro-inflammatory cytokines, such as IL-6 and IL-8, in both serum and cerebrospinal fluid (CSF) of patients. This suggests that cytokine storms may contribute to increased blood-brain barrier permeability, thereby facilitating viral invasion of the CNS [19]. However, the associations between neurological manifestations and both viral load and laboratory findings still require further investigation. Elucidating the pathophysiology of CNS complications is crucial for developing targeted therapeutic interventions to improve clinical outcomes.
METHODS
Study Population
This retrospective cohort study included patients diagnosed with SFTS at Tongji Hospital, Wuhan, between March 2022 and August 2024. A total of 277 patients were included in the study. The inclusion criteria encompassed individuals who met the diagnostic criteria for SFTS, including acute fever, thrombocytopenia, and the detection of SFTSV RNA in plasma using polymerase chain reaction (PCR) [12]. Detailed demographic, clinical, and laboratory data were collected for all patients, and the study aimed to analyze various factors influencing the prognosis of SFTS. The patients with SFTS at the acute phase of disease were divided into acute survival (AS) group and acute deceased group (AD). The clinical outcomes of the patients were monitored for a period of 28 days from the onset of symptoms. Neurological symptoms in patients with SFTS were defined as the presence of acute altered mental status, seizures, cognitive impairment, or coma, without other identifiable causes such as metabolic, hepatic, or drug-induced encephalopathy. Classification was primarily based on clinician-documented observations within 24 hours of hospital admission. When available, CSF analysis and neuroimaging findings were used to support the diagnosis of CNS involvement (eg, encephalopathy or encephalitis). These criteria were utilized to stratify patients into neurological and non-neurological groups for subsequent comparative analyses. This study was approval by the ethical committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (TJ-IRB20230632). Written informed consent was obtained from all participants. The study protocol adheres to the ethical standards of the Declaration of Helsinki.
Collection and Detection of Laboratory Indicators
Blood samples were collected upon hospitalization, complete blood count, liver and renal function tests, coagulation profiles, and cytokine levels were detected. The clinical data, including demographic information, underlying diseases, clinical symptoms and laboratory findings, comorbidity, treatment, and overall prognosis, were collected through the electronic medical record system. SFTSV RNA levels were quantified using the Da'an Gene SFTSV Fluorescent Quantitative PCR Detector Kit (Da An Gene Co., Ltd., Guangzhou, China), which targets the nucleoprotein gene of SFTSV. Quantitative PCR was performed strictly according to the manufacturer's instructions. The reported limit of detection for this assay is 100 copies/mL, as validated in the manufacturer's performance report and widely used in routine clinical diagnostics.
Flow Cytometry Analysis
Fresh whole blood was collected within 24 hours of admission. The percentages and absolute numbers of T, B, and NK cells were determined using TruCOUNT tubes and BD Multitest 6-color TBNK ReagentKit (BD Biosciences). The antibody panels used and analysis flow were based on the methods described in our previously published research [20].
Statistical Analysis
Categorical data were compared using the Chi-square test. For quantitative data, independent t-tests or Mann–Whitney U tests were used for normally or non-normally distributed data, respectively. Kaplan–Meier survival curves were generated, and differences between groups were assessed using the log-rank test. Correlation analysis was performed using the cor function in R, with Pearson correlation coefficients applied for normally distributed data and Spearman correlation coefficients for non-normally distributed data. Heatmaps were created using the “pheatmap” R package to visualize gene or biomarker expression patterns. The prognostic factors of 28-day overall survival were analyzed by Cox regression model. Variables with P < .05 in univariate analysis and/or strong clinical relevance were pre-specified for inclusion. Backward stepwise selection was performed based on the Akaike information criterion, with neurological manifestations and viral load forced into the model due to their clinical significance. Multicollinearity was assessed using variance inflation factors (VIF), and variables with VIF >5 were excluded or combined when appropriate. The proportional hazards assumption was tested using Schoenfeld residuals, and no significant violations were detected. Hazard ratios (HRs) and 95% confidence intervals (CIs) were reported. Statistical analyses were performed using GraphPad Prism version 9.5 (San Diego, CA), SPSS version 22.0 22.0 (IBM Corp., Armonk, NY). Statistical significance was determined as P < .05.
RESULTS
Baseline Characteristics of SFTS Patients With and Without Neurological Symptoms
A total of 277 patients diagnosed with SFTS were enrolled, including 146 females (52.7%) and 131 males (47.3%). Clinical outcomes were evaluated over a 28-day period from symptom onset, during which 181 patients (65.3%) survived and 96 (34.7%) died. Neurological symptoms developed in 78 patients (28.2%). Compared with those without neurological symptoms, affected patients were significantly (median age: 69 vs 64 years, P = .002), and had a markedly higher 28-day mortality rates (67.95% vs 21.61%, P < .001) (Table 1). They also required more intensive interventions, including invasive mechanical ventilation (28.21% vs 4.52%, P < .001) and continuous renal replacement therapy (32.05% vs 10.55%, P < .001). In addition, patients with neurological involvement had a higher prevalence of comorbidities, such as hypertension (42.31% vs 26.63%, P = .017) and hemophagocytosis (53.85% vs 31.16%, P = .001), indicating more severe immune dysregulation.
Laboratory Markers Associated With Neurological Involvement
Patients with neurological complications exhibited significant abnormalities across multiple laboratory parameters (Table 2), reflecting extensive organ dysfunction, coagulation disturbances, metabolic derangements, and systemic inflammation. Elevated levels of cardiac troponin I, myoglobin, and aspartate aminotransferase (AST) levels indicated marked cardiac, muscular, and hepatic injury. Coagulation profiles revealed prolonged activated partial thromboplastin time (APTT) and elevated D-dimer levels, suggestive of a hypercoagulable state. Metabolic dysfunction was evident from hypoalbuminemia and decreased estimated glomerular filtration rate (eGFR), indicating renal impairment. Furthermore, markedly elevated levels of inflammatory cytokines, including IL-6, IL-10, tumor necrosis factor-alpha (TNF-α), and ferritin, highlighted a pronounced cytokine response. Collectively, these findings laboratory findings suggest a complex, multifactorial pathophysiological mechanism underlying neurological complications in SFTS.
Laboratory Markers Associated With Fatal Outcomes in Patients With SFTS
Laboratory analysis revealed significant differences between survival and deceased patients with SFTS, reflecting extensive systemic dysregulation in fatal cases. Deceased individuals exhibited lower platelet counts and elevated levels of liver enzymes (AST, LDH), along with indicators of renal impairment, including reduced eGFR (Figure 1A). Coagulation abnormalities, such as prolonged prothrombin time and APTT, were more pronounced in nonsurvivors, accompanied by elevated inflammatory markers including IL-6, IL-8, IL-10, and TNF-α (Figure 1B). TGF-β1 levels were significantly lower in deceased patients compared with survivors, but showed no significant difference between patients with and without neurological symptoms (Supplementary figure 1a, b). Immunologically, nonsurvivors exhibited significantly reduced absolute counts of CD3+, CD4+, and CD8+ T cells, indicating profound suppression of cellular immunity. In contrast, the total proportion of B cells was increased (Figure 1C). However, subset analysis revealed an abnormal B-cell distribution, characterized by a reduction in naïve B cells and significant increases in plasmablasts and double-negative (IgD-CD27-) B cells (Figure 1D), suggesting early and excessive B-cell activation, impaired differentiation, and potential humoral immunity.
Comparison of clinical, inflammatory, and immunological indicators between survival (AS) group and deceased (AD) group of SFTS patients. A, Liver function and renal function markers between AS and AD groups. B, The comparison of inflammatory and coagulation parameters. C, Peripheral lymphocyte subsets between the groups. D, B-cell subpopulations and plasmablasts between the groups.
Furthermore, heatmap analysis demonstrated that patients with neurological symptoms, particularly those who died, exhibited markedly higher levels of inflammatory cytokines (IL-6, IL-10, and TNF-α), increased viral loads (SFTSV RNA), and more severe coagulation disturbances (Figure 2A and B). These findings underscore the crucial roles of hyperinflammation, viral burden, immune dysfunction, and coagulation abnormalities in the pathogenesis and fatal outcomes of SFTS, especially in patients presenting with neurological involvement. Early recognition of these features may facilitate timely and targeted clinical interventions.
Heatmap analysis of clinical, biochemical, and immunological indicators in SFTS patients. A, Inflammatory cytokine levels, viral load, and coagulation parameters in SFTS patients with and without neurological symptoms and between survivors and deceased individuals. B, Immune cell subset distribution in SFTS patients based on survival status and neurological involvement.
Association of Neurological Symptoms and SFTSV Viral Load With Clinical Outcomes in Patients With SFTS
Patients with neurological symptoms exhibited significantly higher SFTSV viral loads compared with those without (median log_10_ SFTSV RNA: 6.8 [IQR: 5.2–8.1] vs 4.5 [IQR: 3.1–6.3], P < .001; Figure 3A). Kaplan–Meier survival analysis demonstrated a markedly lower 28-day survival probability in patients with neurological symptoms (32.05%) compared with those without (78.39%, log-rank P < .001; Figure 3B). Similarly, deceased patients (AD group) had significantly higher viral loads than survivors (AS group) (P < .001; Figure 3C). Correlation analysis revealed that elevated viral load was significantly associated with several key laboratory abnormalities, including lower platelet counts, increased levels of IL-6, IL-10, TNF-α, prolonged APTT, increased D-dimer levels, and reduced eGFR (Figure 3D), suggesting a close link between viral, immune activation, coagulopathy, and organ dysfunction. Multivariate Cox regression analysis further confirmed that neurological symptoms (HR = 2.565, 95% CI: 1.641–4.011, P < .001) and higher SFTSV viral load (HR = 1.785 per log10 increase, 95% CI: 1.503–2.120, P < .001) were independent predictors of 28-day mortality (Figure 4). These findings underscore the prognostic importance of both CNS involvement and vital replication in the clinical course of SFTS.
Association of neurological symptoms and SFTSV viral load with clinical outcomes in SFTS. A, Comparison of SFTSV viral load between patients with and without neurological symptoms. B, Kaplan–Meier survival curves showing significantly lower survival probability in patients with neurological symptoms. C, SFTSV viral load between survivors (AS group) and nonsurvivors (AD group). D, Correlation heatmap showing associations between viral load and key laboratory parameters, including platelet count, inflammatory cytokines, immune markers and coagulation indicators.
Neurological symptoms and viral load predict mortality of SFTS patients.
DISCUSSION
This study demonstrated that neurological involvement plays a pivotal role in determining disease severity and clinical outcomes in patients with SFTS. Patients who developed neurological symptoms exhibited significantly higher mortality rates and more severe disease presentations, underscoring the importance of early recognition and targeted management of CNS complications. These findings are consistent with previous studies identifying neurological manifestations, particularly encephalitis, as key indicators of poor prognosis in SFTS [17, 22]. Importantly, this study builds upon existing knowledge by comprehensively integrating clinical and laboratory parameters, including immune-related biomarkers, thereby offering a more refined and detailed evaluation of prognostic factors.
One of the most important findings of this study is the observed association between elevated SFTSV RNA viral loads and neurological involvement, both of which were independently associated with increased mortality risk [11, 16]. While prior studies have reported a correlation between high viral load and disease severity [15], the present study further emphasizes the synergistic interplay between CNS complications and viral burden. This relationship suggests the potential for direct viral neuroinvasion and/or indirect CNS injury mediated by systemic immune dysregulation. The significantly elevated levels of pro-inflammatory cytokines, including IL-6, IL-10, TNF-α, and ferritin, among patients with neurological manifestations support the hypothesis of cytokine-mediated neurotoxicity, thereby extending current knowledge of cytokine storm mechanisms in severe viral infections.
The comprehensive analysis integrating laboratory and immunological parameters provides important insights into the systemic pathophysiology underlying CNS involvement and adverse outcomes in SFTS. Patients with fatal outcomes consistently exhibited significant coagulation disturbances, renal impairment, and elevated markers of organ injury. These findings are consistent with previous studies reporting multi-organ dysfunction and coagulopathy as hallmarks of severe SFTS [20, 23]. These abnormalities coincided with heightened levels of inflammatory cytokines, particularly IL-6, IL-10, TNF-α, and ferritin, which are known mediators of cytokine storm syndromes [12, 24]. Excessive cytokine release has been implicated in blood-brain barrier disruption and subsequent neuroinflammation in viral infections, suggesting that the neurological complications observed in SFTS may result not only from direct viral neurotropism, but also from immune-mediated CNS injury. Previous experimental and clinical studies have demonstrated that elevated IL-6 and TNF-α levels can increase blood-brain barrier permeability, promote leukocyte infiltration into the CNS, and exacerbate neuronal damage [25, 26]. Consistent with prior findings in fatal SFTS and severe COVID-19, we observed significantly reduced TGF-β1 levels in nonsurvivors, supporting the notion of impaired immunoregulatory control during disease progression [27, 28]. This imbalance between elevated IL-6/IL-10 and suppressed TGF-β1 may exacerbate systemic inflammation and contribute to poor clinical outcomes.
Although our study identified significant elevations of IL-6, IL-8, IL-10, and TNF-α in patients with severe outcomes, the specific cellular sources of these cytokines could not be determined within our current design. Previous studies have identified monocytes and macrophages as primary sources of IL-6, IL-10, and TNF-α during viral infections, while IL-8 is typically secreted by macrophages and endothelial cells [29–31]. Effector T cells are known to secrete pro- and anti-inflammatory cytokines, including TNF-α and IL-10, in response to viral or other pathogenic stimulation [32]. Moreover, our recent single-cell RNA sequencing study demonstrated that plasmablasts from SFTS patients can produce TNF-α and IL-6, suggesting a potential role for B cells in driving cytokine-mediated inflammation and immune dysregulation [21]. Future research utilizing single-cell transcriptomics or intracellular cytokine staining is warranted to accurately identify the cellular sources of inflammatory cytokines in SFTS and clarify their contribution to CNS injury. Furthermore, hyperferritinemia, often seen in HLH syndrome, is associated with severe systemic inflammation and adverse neurological outcomes [33].
Immunological dysregulation may play a pivotal role in the pathogenesis of severe SFTS and its associated CNS complications. Previous studies have shown that fatal viral infections are frequently accompanied by lymphopenia and T-cell exhaustion, both of which compromise antiviral immunity and contribute to systemic inflammation [9, 24, 34]. Consistent with this, our findings indicate profound suppression of cellular immunity in severe SFTS, reflected by reduced in CD4+ and CD8+ T-cell populations. Although an overall increase in B-cell proportion, the skewed distribution, characterized by reduced naïve B cells and increased plasmablasts and double-negative B cells, suggests dysregulated humoral immunity. B cells have been identified as primary targets of SFTSV infection, and transient plasmablast expansion has been associated with ineffective antibody responses, contributing to poor outcomes in severe SFTSV infection [35–37]. These immune features may facilitate viral persistence, enhance cytokine production and disrupt the blood-brain barrier, thereby increasing the risk of CNS injury. The combined impairment of T-cell surveillance and maladaptive B-cell responses may represent a central immunopathogenic mechanism in fatal SFTS.
In light of these findings, it is also important to evaluate how our results may inform and enhance current prognostic frameworks for SFTS. The prognostic value of the identified clinical and laboratory parameters is further validated by our multivariate Cox regression analysis, which identified both neurological manifestations and viral load as independent predictors of mortality. These results not only corroborate previous evidence regarding the association between high viral burden and disease severity [28], but also highlight the often-overlooked impact of CNS involvement on patient outcomes in SFTS. Most existing prognostic models for SFTS primarily incorporate general clinical indicators such as age, platelet count, or hepatic function markers [18, 38, 39]. Although these variables contribute to risk assessment, they frequently omit neurological symptoms and immune-inflammatory markers, which, as our findings suggest, are critically associated with disease progression and fatal outcomes. By integrating parameters reflective of immune dysregulation (eg, cytokine elevations, ferritin levels), organ dysfunction, and CNS complications, our study provides a more comprehensive framework for risk stratification. This integrative approach may significantly enhance the predictive accuracy of existing models, enabling earlier recognition of high-risk patients and facilitating more targeted clinical interventions. Due to the retrospective design, dynamic temporal profiles of viral load and cytokine levels were not available. As such, we could not conclusively determine whether neurological symptoms were preceded or triggered by peak viremia or immune activation. This limits causal inference and highlights the need for prospective studies with serial monitoring of viral kinetics and host immune responses.
This study has several notable limitations. First, its single-center retrospective design inherently limits generalizability and increases susceptibility to selection bias, necessitating validation through multicenter prospective cohorts. Second, the absence of CSF analyses and neuroimaging data precludes direct assessment of neurotropic viral invasion and CNS-specific pathological changes. Third, while we adjusted for key covariates, residual confounding factors (eg, pre-existing neurological conditions or genetic predispositions) may influence the observed associations. Finally, the lack of longitudinal follow-up beyond the acute phase restricts our understanding of long-term neurological sequelae and functional recovery patterns. Future studies incorporating standardized CSF virology, advanced neuroimaging modalities, and extended neurocognitive assessments would enable more robust characterization of SFTS-related neuropathogenesis.
CONCLUSION
In conclusion, this study highlights the pivotal role of neurological manifestations and high viral load in driving disease progression and mortality in patients with SFTS. These findings underscore the urgent need for heightened clinical awareness of CNS involvement and viral burden as key indicators of poor prognosis. Considering neurological and immune profiles in risk assessment may contribute to earlier recognition of disease severity and personalized management. Further prospective studies are warranted to elucidate the underlying mechanisms and to develop effective strategies for reducing SFTS-related mortality.
Supplementary Material
ofaf803_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yu XJ, Liang MF, Zhang SY, et al Fever with thrombocytopenia associated with a novel Bunyavirus in China. N Engl J Med 2011; 364:1523–32.21410387 10.1056/NEJ Moa 1010095 PMC 3113718 · doi ↗ · pubmed ↗
- 2Kwon JS, Jin S, Kim JY, et al Viral and immunologic factors associated with fatal outcome of patients with severe fever with thrombocytopenia syndrome in Korea. Viruses 2021; 13:2351.34960620 10.3390/v 13122351 PMC 8703577 · doi ↗ · pubmed ↗
- 3Kobayashi Y, Kato H, Yamagishi T, et al Severe fever with thrombocytopenia syndrome, Japan, 2013–2017. Emerg Infect Dis 2020; 26:692–9.32186502 10.3201/eid 2604.191011 PMC 7101122 · doi ↗ · pubmed ↗
- 4Tran XC, Yun Y, Kim SH, et al Endemic severe fever with thrombocytopenia syndrome, Vietnam. Emerg Infect Dis 2019; 25:1029–31.31002059 10.3201/eid 2505.181463 PMC 6478219 · doi ↗ · pubmed ↗
- 5Casel MA, Park SJ, Choi YK. Severe fever with thrombocytopenia syndrome virus: emerging novel phlebovirus and their control strategy. Exp Mol Med 2021; 53:713–22.33953322 10.1038/s 12276-021-00610-1PMC 8178303 · doi ↗ · pubmed ↗
- 6Li J, Li S, Yang L, et al Severe fever with thrombocytopenia syndrome virus: a highly lethal Bunyavirus. Crit Rev Microbiol 2021; 47:112–25.33245676 10.1080/1040841 X.2020.1847037 · doi ↗ · pubmed ↗
- 7Huang X, Li J, Li A, et al Epidemiological characteristics of severe fever with thrombocytopenia syndrome from 2010 to 2019 in mainland China. Int J Environ Res Public Health 2021; 18:3092.33802869 10.3390/ijerph 18063092 PMC 8002760 · doi ↗ · pubmed ↗
- 8Yuan C, Xu Q, Ning Y, et al Potential mechanisms implied in tick infection by arboviruses and their transmission to vertebrate hosts. Integr Zool 2025; 20:315–30.39016029 10.1111/1749-4877.12875 PMC 11897945 · doi ↗ · pubmed ↗