A peritoneal effluent sequencing assay that removes environmental DNA contamination in peritoneal dialysis patients
Liz-Audrey Kounatse Djomnang, Vesh Srivatana, Omary Mzava, Emma Belcher, Lars F Westblade, Darshana M Dadhania, Carol Li, Iwijn De Vlaminck, John R Lee

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
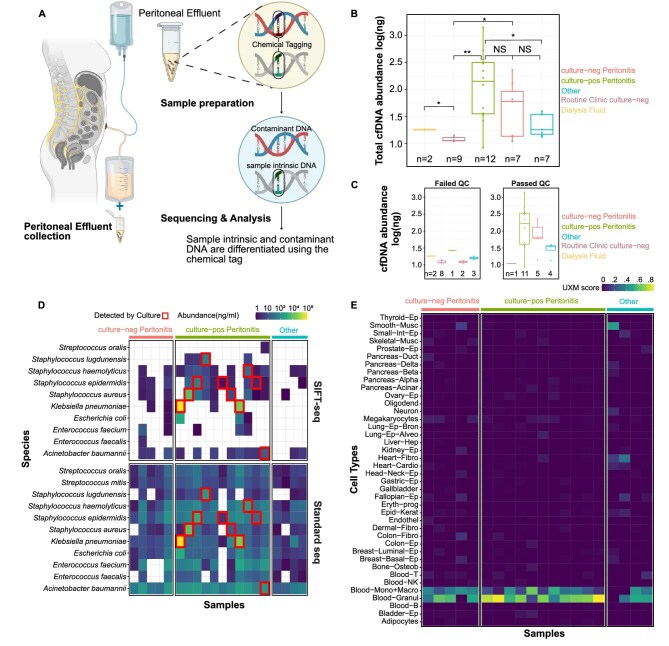 Figure 1
Figure 1- —NIH10.13039/100000002
- —NKF10.13039/100001259
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDialysis and Renal Disease Management · Health, Environment, Cognitive Aging · Cancer Genomics and Diagnostics
To the Editor,
Newer DNA sequencing techniques have the potential to identify microbial DNA in peritoneal dialysis (PD) patients with peritonitis and without peritonitis. However, given the potential low biomass of microbial DNA in peritoneal effluent, introduction of contaminant DNA during the sequencing process can lead to errors in microbial identification. We have developed Sample-Intrinsic microbial DNA Found by Tagging and Sequencing (SIFT-seq), a metagenomic sequencing assay that is robust to contamination [1]. The key concept for SIFT-seq is the chemical labeling of DNA by bisulfite salt treatment prior to sequencing, and any DNA without the chemical signature can be identified and removed [1]. SIFT-seq was shown to identify microbes in blood and urine specimens while removing environmental DNA contamination [1]. In this study, we assess its utility in PD patients with culture-confirmed peritonitis and culture-negative peritonitis.
We recruited 31 PD patients who provided a total of 35 peritoneal effluent specimens. The Weill Cornell IRB approved this protocol (1 604 017 181) and all patients provided written informed consent. Full details of SIFT-seq can be found in Mzava et al. [1], the Supplementary data and Fig. 1A. Briefly, we collected peritoneal effluent specimens from subjects in the PD clinic or the hospital. Bisulfite treatment was performed on the peritoneal effluent supernatant using either Lightning-conversion [1] or methylation-direct kit (Zymo Research, Irvine, CA, USA). Cell-free DNA (cfDNA) libraries were sequenced on an Illumina Nextseq 2000 (Illumina, San Diego, CA, USA). cfDNA sequences without bisulfite conversion (contaminant cfDNA) were removed bioinformatically and cfDNA tissue-of-origin analysis were performed as described in the Supplementary data.
Among the 35 peritoneal fluid specimens, 12 were from 12 PD patients with culture-confirmed bacterial peritonitis (culture-pos peritonitis); 7 were obtained from 7 PD patients with culture-negative peritonitis (culture-neg peritonitis); 9 were obtained from 8 PD patients without symptoms in the PD clinic and had negative peritoneal effluent culture (routine clinic culture-neg); and 7 were obtained from PD patients with a range of pathologies (2 with fungal peritonitis, 2 with abdominal pain without evidence of peritonitis, 2 with hypertensive crisis and 1 with prior peritonitis) (other). PD patients may have contributed specimens across groups. Two specimens were taken directly from Baxter-manufactured solutions (Baxter International, Deerfield, IL, USA) as controls (neg control). Demographic/clinical data are presented in Supplementary data, Table S1.
Twenty-one of the 35 peritoneal effluent specimens passed quality control (QC) with at least 10 million reads post-trimming, 10% mapping efficiency and 80% conversion efficiency. Importantly, eight of the nine peritoneal effluent specimens from the routine clinic culture-neg group and both specimens from the neg control group did not pass QC, suggesting a lower limit to the utility of SIFT-seq on low biomass specimens. In contrast, 11 of 12 specimens from the culture-pos peritonitis group passed QC and 5 of 7 specimens from the culture-neg peritonitis passed QC (Fig. 1B and C).
Among the 21 specimens that passed QC, common microbes causing peritonitis were abundantly detected in all specimens prior to computational removal of contaminant cfDNA (Fig. 1D). However, after filtering out contaminant DNA, there was significant reduction in microbial noise and notably the presumed causative agent of culture-pos peritonitis cases was detected in all cases except for one peritonitis case of Acinetobacter junii, but Acinetobacter baumannii cfDNA was detected (Fig. 1D). Importantly, in two of the culture-pos peritonitis cases, specimens were taken after antibiotic administration, suggesting the use of SIFT-seq in PD patients who may have already been treated for peritonitis. Tissue-of-origin analysis revealed that the majority of cfDNA originates from monocytes, macrophages and granulocytes in culture-pos and culture-neg peritonitis (Fig. 1E). Limitations of the study include the small sample size, the lack of comparison with 16S rRNA gene sequencing and the exploratory nature of SIFT-seq on peritoneal effluent, restricting generalizability of the conclusions. Despite these limitations, SIFT-seq may be a novel technique for detecting microbes in PD patients with and without peritonitis.
Supplementary Material
sfaf358_Supplemental_File
The reference list from the paper itself. Each links out to its DOI / PubMed record.