Efficacy and safety of single-trajectory posterior subthalamic area and subthalamic nucleus deep brain stimulation for dystonic tremor: a retrospective pilot study
Jianyi Shen, Zhengyu Lin, Suzhen Lin, Peng Huang, Yixin Pan, Bomin Sun, Jianqing Ding, Yiwen Wu, Dianyou Li

TL;DR
A new deep brain stimulation method targeting two brain areas at once shows promise for treating dystonic tremor with high safety and effectiveness.
Contribution
A novel single-lead, dual-target DBS approach for dystonic tremor is introduced and evaluated.
Findings
Combined PSA and STN stimulation was preferred by 83.3% of patients and showed greater efficacy than single-target stimulation.
Mean tremor scores improved by 78.1% and 87.1% on two clinical scales after 6–12 months of treatment.
No serious adverse events were reported, indicating the approach is safe.
Abstract
To evaluate the feasibility, safety, and preliminary efficacy of a novel single-lead, dual-target deep brain stimulation (DBS) approach targeting the posterior subthalamic area (PSA) and subthalamic nucleus (STN) for dystonic tremor. This retrospective pilot study reviewed outcomes of six consecutive patients with medically refractory dystonic tremor who underwent single-lead PSA-STN DBS at our center (June–December 2024). Clinical outcomes were assessed using the BFMDRS and FTMTRS scales. A formal blinded crossover assessment was performed in three patients to compare PSA-only, STN-only, and combined stimulation. Chronic settings were selected via patient-directed optimization. All six patients completed follow-up (100% retention) and achieved stable chronic stimulation programs. Five patients (83.3%) independently selected combined PSA + STN stimulation; one preferred STN-only. At…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
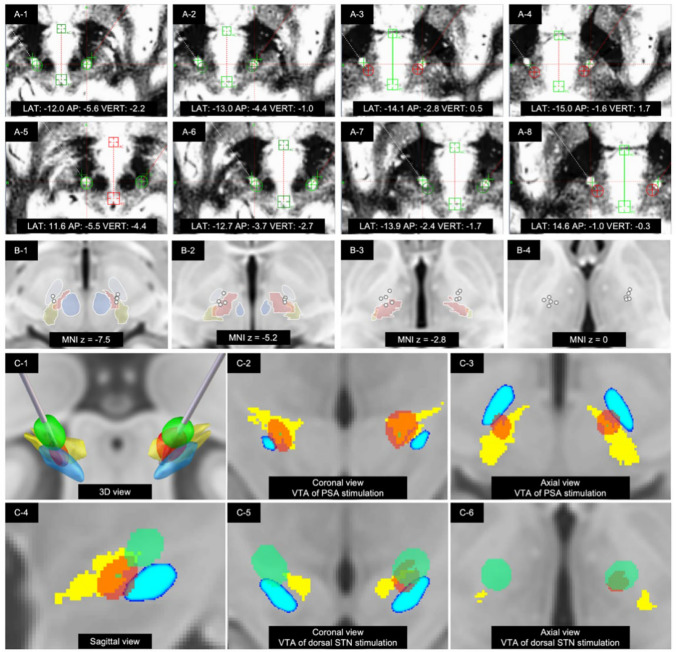 Figure 1
Figure 1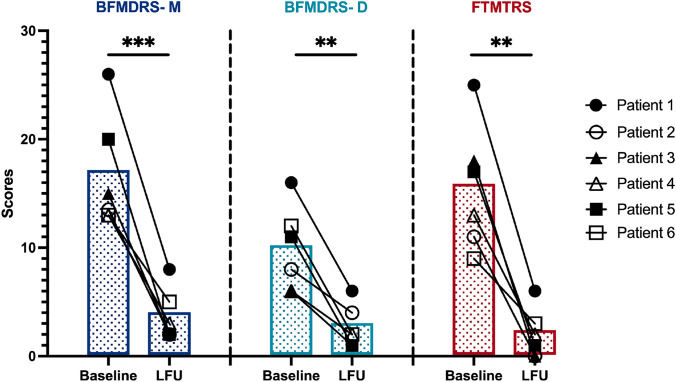 Figure 2
Figure 2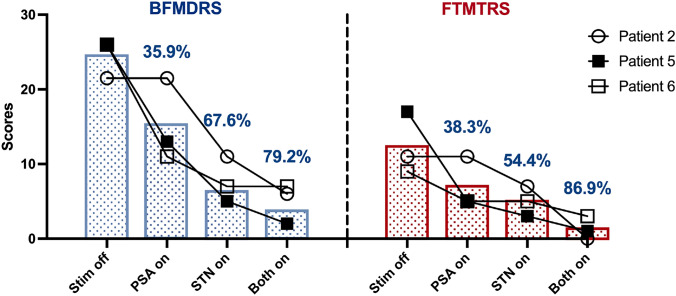 Figure 3
Figure 3- —Shanghai Health and Family Planning Commission research project
- —Shanghai Youth Science and Technology Talents Sailing projects
- —Youth Project of National Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological disorders and treatments · Transcranial Magnetic Stimulation Studies · Botulinum Toxin and Related Neurological Disorders
Introduction
Dystonia with prominent tremor (hereafter referred to as dystonic tremor [DT]) is a complex hyperkinetic phenotype in which dystonia—sustained or intermittent muscle contractions causing abnormal movements and postures—is accompanied by a prominent, often rhythmic tremor in the same or overlapping body part. Recent MDS updates to dystonia definitions recognize that dystonic movements and postures may have a tremulous quality and emphasize careful phenomenological description when tremor coexists with dystonia [1]. While recent expert commentaries encourage more descriptive phenomenological classification of tremor in the context of dystonia, we retain the term dystonic tremor to denote the clinical phenotype of our cohort—patients with isolated dystonia presenting with a prominent, often rhythmic tremor component—consistent with established usage in the Deep brain stimulation (DBS) literature [2–4].
DBS has emerged as the most effective surgical treatment for medically refractory dystonia [2, 3]. Both the globus pallidus internus (GPi) and subthalamic nucleus (STN) have been established as effective targets for treating dystonia [4]. Our center has extensive experience with STN and GPi DBS for dystonia, and we previously published a comprehensive comparison of STN and GPi efficacy in treating isolated dystonia. We demonstrated that the GPi and STN are safe and effective targets for isolated dystonia [5, 6].
However, while both STN and GPi stimulation can effectively control dystonic symptoms in DT patients, their efficacy in controlling the tremor component remains variable and inconsistent across patients [4, 7]. The ventralis intermedius nucleus (VIM) of the thalamus is commonly targeted for tremor control, and combined GPi and VIM DBS treatment has shown superior outcomes compared to single-target stimulation [8, 9]. Nevertheless, this dual-target approach requires the implantation of two separate DBS devices, increasing invasiveness and cost.
The posterior subthalamic area (PSA) has emerged as a promising target for tremor control in recent years [10–12]. In our 2024 publication, we demonstrated that PSA-DBS is comparable with VIM-DBS in suppressing tremors, superior in improving disease-specific quality of life, and possibly more effective in reducing head tremor [13]. Importantly, the anatomical proximity of the PSA and STN presents a unique opportunity: the possibility of targeting both structures with a single electrode trajectory. Therefore, we explored this alternative combined targeting strategy as a potential solution for DT. This single-electrode, dual-target approach could potentially address both dystonic and tremor components of DT while avoiding the increased surgical trauma and costs associated with implanting two separate DBS systems. Here, we present a retrospective analysis of our initial clinical experience with PSA-STN DBS in six DT patients, including a blinded crossover assessment in three patients to objectively evaluate the individual and combined effects of each target.
Patients and methods
Study design
This retrospective pilot study was designed to assess the feasibility, safety and preliminary clinical outcomes of a novel dual-target DBS approach. Consistent with pilot study methodology[14, 15], our primary objectives were to evaluate: (1) procedural feasibility, (2) safety, (3) patient acceptability, and (4) retention and protocol completion. Efficacy analyses are exploratory and hypothesis-generating, intended to inform future confirmatory trials.
Patients
We conducted a retrospective analysis of the clinical outcomes of six patients with medically refractory isolated dystonia and presented with a prominent rhythmic tremor phenotype in the affected body region who underwent single-lead, dual-target PSA-STN DBS surgery at our center between June 2024 and December 2024. Six patients comprised the complete cohort during this period; no eligible patient was excluded. The date of surgery and follow-up duration for each patient are provided in Table 1. This retrospective pilot study was approved by the Institutional Review Board of Ruijin Hospital (Approval ID: Clinical Ethics Review (2024) No. 84; Approval Date: April 11, 2024). All patients provided written informed consent for the DBS procedure and for the use of their anonymized clinical data for research purposes. The study adhered to the principles of the Declaration of Helsinki. A copy of the IRB approval is available upon request.Table 1. Demographic and clinical characteristicsPatientSexFamily historyAge at onset (year)Age at surgery (year)Surgery date (month/year)Duration of symptoms (month)Dystonia distributionTremor siteLFU (month)Follow-upBFMDRS-Motor scoreBFMDRS-Disability scoreFTMTRSPatient 1FNone5065September 2024190Blepharospasm; mouth; torticollis;upper limb dystoniaarms; head; voice; face6Baseline261625LFU866Patient 2FNone4964June 2024189Blepharospasm; mouth; torticollis/laterocollishead; voice; face12Baseline13.5811LFU240Patient 3MNone5359June 202472Blepharospasm; mouth; torticollis/retrocollis;truncal dystoniahead; face; arms12Baseline15618LFU210Patient 4MNone5765July 2024107Blepharospasm; laryngeal dystonia; anterocollishead; voice; face12Baseline13613LFU322Patient 5FNone4561August 2024199Writer's cramp; torticollis; truncal dystoniahead; voice; arms12Baseline201117LFU211Patient 6FNone2433September 2024104Torticollis; upper limb dystoniahead6Baseline13129LFU523Mean ± SD46.3 ± 11.757.8 ± 12.4143.5 ± 55.410 ± 3.1Baseline16.8 ± 5.39.8 ± 3.915.5 ± 5.8LFU3.7 ± 2.42.8 ± 2.02 ± 2.3P-value^a^ (Baseline vs. LFU)0.0006(0.0312)0.0025(0.0312)0.0012(0.0312)LFU last follow up, All patients had isolated dystonia; secondary causes were excluded by MRI and comprehensive laboratory screening^a^P-values were calculated using the paired Student's t-test, with results from the Wilcoxon signed-rank test shown in parentheses
Inclusion criteria were: (i) a diagnosis of isolated dystonia and presented with a prominent rhythmic tremor phenotype in the affected body region according to MDS consensus criteria [1].The dystonia was the primary and most disabling feature, or the tremor was refractory to medications typically used for essential tremor. (ii) no acquired etiology or neurodegenerative diseases or preoperative brain MRI with any signs of structural brain damage. (iii) accurate electrode position confirmed by pre- and post-operative neuroimaging. (iv) the patient and/or their caregiver needed to demonstrate the ability and willingness to manage the patient programmer to switch between stimulation programs at home.
Patients were excluded if they had severe cognitive impairment or an uncontrolled psychiatric illness that would interfere with informed consent or postoperative management. Exclusion criteria also included the presence of any structural brain anomalies on preoperative MRI that could be responsible for the symptoms or any general contraindications to neurosurgery.
Etiologic evaluation included brain MRI and comprehensive laboratory screening (copper metabolism, thyroid function, vitamin levels, etc.) to exclude secondary causes; no structural lesions or neurodegenerative features were identified. Clinical characteristics, including age at onset, distribution, and family history, are detailed in Table 1. Genetic testing was not performed.
The cohort comprised four women and two men who met MDS consensus criteria. Patient 1 developed limb tremor and cramping that advanced to facial dystonia, torticollis and laryngeal tremor. Patient 2 presented with cervical dystonia (torticollis to the left with laterocollis to the right) that gradually progressed with marked head tremor, facial dystonia, and voice tremor. Patient 3 started with truncal dystonia that spread upward to torticollis–retrocollis and was joined by jerky head tremor plus facial and arm tremor. Patient 4 started with blepharospasm and anterocollis, later adding head tremor and laryngeal dystonia. Patient 5 had writer’s cramp that extended to torticollis with tremor and voice involvement. Patient 6 initially noted mild right torticollis, and eight years later the dystonic head turn and superimposed tremor intensified and postural arm tremor emerged. All had trialed medications and/or botulinum toxin without sustained benefit.
Surgical procedures
The PSA and STN were simultaneously targeted using a single DBS trajectory, as described in our previous work [16]. In contrast to our routine STN-DBS procedure for dystonia, in which the dorsolateral sensorimotor STN serves as the primary target and the trajectory is optimized to maximize intranuclear STN coverage, the present approach designates the PSA as the primary target. The PSA was directly visualized on axial T2-weighted MRI as a hypointense region located medial to the posterior tail of the STN and lateral to the red nucleus, at the level of the maximal diameter of the red nucleus. The STN was similarly identified on T2-weighted images as the hypointense biconvex structure lateral to the red nucleus. The trajectory was planned using the PSA as the primary target; the coronal and sagittal angles were then adjusted to obtain a trajectory that also traversed the dorsal STN, while avoiding sulci, blood vessels, and ventricles. This strategy positions the ventral electrode contacts in the PSA and the dorsal contacts in the dorsal STN region. The Leksell stereotactic frame arc and ring angles for all trajectories are provided in Supplementary Table S1.
Patient 1 received bilateral four-contact cylindrical leads (SceneRay SR1200; contact length 1.5 mm; inter-contact spacing 0.5 mm; total array span 7.5 mm), analogous to Medtronic 3389. Patients 2–6 received bilateral four-contact cylindrical leads (SceneRay SR1210; contact length 1.5 mm; inter-contact spacing 1.5 mm; total array span 10.5 mm), analogous to Medtronic 3387. All patients received a rechargeable implantable pulse generator (SceneRay SR1101). The 1.5 mm spacing configuration (SR1210) was preferred for most patients because its longer electrode array span (10.5 mm vs. 7.5 mm) facilitates simultaneous coverage of both the PSA and region dorsal to the STN within a single trajectory, which is essential for the dual-target stimulation strategy. The latter model was adopted after the first case to provide a longer contact span and potentially finer control over the dual-target region. The placement of all leads was verified by merging the postoperative CT with the preoperative MR. All participants had at least one contact in the PSA and one in the STN.
DBS programming, patient-directed optimization, and crossover assessment
Initial programming commenced approximately one month after DBS implantation and was performed by an experienced movement disorder neurologist. A systematic monopolar review was performed on each contact to map immediate therapeutic effects on tremor and to identify stimulation-induced side-effect thresholds.
Based on this initial mapping and our dual-target hypothesis, a flexible, patient-centric programming strategy was implemented. Patients were offered three distinct stimulation programs: (1) PSA stimulation; (2) STN stimulation; (3) interleaved PSA + STN stimulation. The specific contact configuration (single- or dual-cathode) within each target was individualized based on the monopolar review; detailed programming parameters for each patient are provided in Table 2. Patients were given autonomy to switch between programs at home and to adjust stimulation amplitude within predefined safe ranges. Patients were instructed to alternate between programs during the initial two-month optimization period, maintaining each program for at least one week to allow adequate assessment of therapeutic effects. At the two-month follow-up, patient preferences were formally recorded; non-preferred programs were subsequently deactivated to simplify device management. Five of six patients independently selected combined PSA + STN stimulation; Patient 3 preferred STN-only stimulation based on his symptom profile. Non-preferred programs were subsequently deactivated to simplify device management.Table 2. Optimal stimulation parametersPatientSideParametersPatient 1Leftc + 8–9-, 50 μs, 160 Hz, 4.0 mAc + 11-, 60 μs, 160 Hz, 0.5 mARightc + 0–1-, 30 μs, 160 Hz, 4.0 mAc + 3-, 50 μs, 160 Hz, 0.25 mAPatient 2Leftc + 9-, 50 μs, 160 Hz, 2.5 Vc + 10–11-, 60 μs, 160 Hz, 3.7 VRightc + 1-, 50 μs, 160 Hz, 2.75 Vc + 2–3-, 60 μs, 160 Hz, 3.95 VPatient 3Leftc + 10–11-, 50 μs, 160 Hz, 2.15 Vc + 11-, 60 μs, 160 Hz, 3.45 VRightc + 2–3-, 50 μs, 160 Hz, 2.45 Vc + 3-, 60 μs, 160 Hz, 3.75 VPatient 4Leftc + 9-, 60 μs, 125 Hz, 1.7 Vc + 10-, 60 μs, 125 Hz, 2.9 VRightc + 0-, 60 μs, 125 Hz, 1.5 Vc + 2–3-, 60 μs, 125 Hz, 2.7 VPatient 5Leftc + 9–10-, 50 μs, 145 Hz, 2.55 Vc + 11-, 50 μs, 145 Hz, 3.5 VRightc + 0–1-, 30 μs, 145 Hz, 2.35 Vc + 3-, 50 μs, 145 Hz, 3.75 VPatient 6Leftc + 8-, 30 μs, 160 Hz, 3.45 Vc + 10–11-, 50 μs, 160 Hz, 3.75 VRightc + 0-, 30 μs, 160 Hz, 3.15 Vc + 2–3-, 50 μs, 160 Hz, 3.85 VThe numbers 0 to 3 and 8 to 11 were assigned to the left and right DBS lead from the ventral-most to dorsal-most contacts
During the last follow-up visit, a formal blinded crossover assessment was conducted in three patients (Patients 2, 5, and 6; at 12 months for Patients 2 and 5, and at 6 months for Patient 6). The other three patients declined due to personal time constraints or concerns about the extended assessment duration. Four stimulation conditions were tested: Off-stimulation, PSA-only, STN-only, and combined PSA + STN. After an initial 30 min Off period, baseline assessments were performed. The order of the three active stimulation conditions was randomized. Each active condition was tested following a 30 min wash-in period; a 30 min washout (Off) period was interposed between each active condition. Both the patient and evaluating neurologist were blinded to the active stimulation settings. Clinical assessments (BFMDRS and FTMTRS) were performed under each of the four conditions, yielding 8 scale administrations per patient. The complete protocol required approximately 4 h. All six patients were invited to participate; three volunteered and completed the protocol without adverse events. This protocol was designed primarily to assess acute tremor responses; dystonia findings are exploratory given the limited washout duration.
Outcome measures
Clinical outcome data were retrospectively collected from patient records. These records included assessments performed preoperatively and at follow-up visits in the outpatient setting, with the last available assessment for each patient defined as the last follow-up (LFU). The Burke Fahn Marsden Dystonia Rating Scale (BFMDRS) was used to rate the severity of dystonia. Changes in tremor severity and functional impact were assessed using the Fahn-Tolosa-Marin tremor rating scale (FTMTRS). Because this was a retrospective pilot cohort, early postoperative BFMDRS and FTMTRS assessments were not uniformly available for all six patients at standardized time points. Therefore, the primary efficacy evaluation focused on comparisons between baseline and the LFU to avoid potentially biased inferences from incomplete early datasets. Patients were regularly followed up at the outpatient department by a specialist knowledgeable of the patients’ condition. Adverse events were recorded.
Statistical analysis [17, 18]
Analysis population: All six implanted patients were included in safety, feasibility, and exploratory efficacy analyses. There were no missing data for primary outcomes.
Chronic stimulation outcomes (N = 6): Clinical outcomes (BFMDRS-Motor, BFMDRS-Disability, FTMTRS) were assessed at baseline and last follow-up (LFU). Within-patient changes are summarized as means ± standard deviations and percentage improvements. Paired t-tests were used for within-patient comparisons; Wilcoxon signed-rank tests were performed as sensitivity analyses, yielding consistent results (Table 1). Effect sizes (Cohen's d for paired samples, calculated as mean difference divided by standard deviation of differences, with 95% confidence intervals) are reported to facilitate interpretation and future sample size calculations. No adjustment for multiple comparisons was applied given the exploratory nature of these analyses; p-values should be interpreted descriptively.
Crossover assessment (N = 3): Given the very small sample, results are presented descriptively with individual patient data; no inferential statistics were performed.
Analyses were performed using R (version 4.3).
Results
Patient characteristics and electrode placement
Table 1 presents the demographic and clinical characteristics of the six patients enrolled in this study, comprising four females and two males. The age at surgery ranged from 33 to 65 years. The mean age at disease onset was 46.3 ± 11.7 years, while the mean age at the time of surgery was 57.8 ± 12.4 years. Figure 1 provides an illustration of the pre- and post-operative fused imaging for a representative patient, confirming the final electrode location. The optimized stimulation parameters for each patient at the LFU are detailed in Table 2. The mean duration of symptoms prior to surgery was 143.5 ± 55.4 months.Fig. 1. Single-trajectory PSA-STN dual-target DBS. (A-1)‒(A-8) Representative contact locations shown from the ventral-most to the dorsal-most positions, with AC-PC-based stereotactic coordinates. (B-1)‒(B-4) Active contact locations displayed in relation to subthalamic area in MNI standard space (blue, red nucleus; light blue, subthalamic nucleus [STN]; rose red, fasciculus cerebellothalamicus [fct]; yellow brown, caudal zona incerta [cZI]). (C) A representative volume of tissue activated in relation to the subthalamic area. (C-1)‒(C-6) A representative VTA shown in 3D and 2D axial views. The ventral stimulation site is referred to as the PSA/cZI-border contact and the dorsal stimulation site as the dorsal STN/Zi-border contact, reflecting relative electrode position along the single trajectory (blue, subthalamic nucleus [STN]; yellow, posterior subthalamic area [PSA]; red, VTA of PSA stimulation; green, VTA of dorsal STN stimulation)
The mean anterior commissure-posterior commissure-based stereotactic coordinates of the chronically active contacts are detailed in Table 3. The mean coordinates for active PSA contacts were |X|= 10.8 ± 1.1 mm, Y = −4.9 ± 0.9 mm, and Z = −2.4 ± 1.2 mm. The mean coordinates for active STN contacts were |X|= 12.8 ± 1.4 mm, Y = −1.9 ± 1.2 mm, and Z = 1.5 ± 1.5 mm.Table 3. Stereotactic coordinates of active contactsPatientSidePSASTNXYZXYZPatient 1Left−12.5−5.0−1.6−15.0−1.61.7Right12.1−4.6−3.614.6−1−0.3Patient 2Left−12.1−6.8−1.9−13.7–4.51.8Right11.2−5.8−0.212.9−3.43.5Patient 3Left‒‒‒−11.8−2.71.6Right‒‒‒13.0−0.42.1Patient 4Left−10.0−3.9−2.7−10.9−1.8−0.7Right10.1−5.2−4.213.7−2.3−0.8Patient 5Left−9.7−3.5−0.8−10.7−1.91.5Right9.9−5.1−3.211.6−1.80.8Patient 6Left−10.9−4.5−2.4−13.5−1.03.8Right9.8−4.6−3.512.6−0.22.5Average^b^10.8 ± 1.1−4.9 ± 0.9−2.4 ± 1.212.8 ± 1.4−1.9 ± 1.21.5 ± 1.5The stereotactic coordinates of PSA and STN of the optimal stimulation parameters were shownPSA posterior subthalamic area, STN subthalamic nucleus^a^The midcommissural point was set as origin (0,0,0)^b^The average of the absolute value of X coordinates was calculated
Feasibility outcomes
Feasibility was assessed across six predefined objectives. (i) Procedural implementation: All six patients (100%) underwent successful bilateral DBS implantation, with postoperative imaging confirming accurate electrode placement ensuring at least one contact in the PSA and one in the STN for each patient. (ii) Retention and data completeness: All patients (100%) completed their designated follow-up periods (6 months for Patients 1 and 6; 12 months for Patients 2–5) with complete primary outcome data. (iii) Patient-directed programming: All patients successfully managed the three-program switching paradigm at home. (iv) Crossover completion: All three patients assigned to the blinded crossover assessment completed all four stimulation conditions. (v) Patient acceptability: Five of six patients (83.3%) independently selected combined PSA + STN stimulation as their preferred chronic setting. (vi) Safety: The procedure was well-tolerated with no serious adverse events, hardware complications, infections, or intracranial hemorrhages. Transient stimulation-induced paresthesias occurred during programming but resolved with parameter adjustment. One patient (16.7%) experienced mild STN-induced dyskinesia at higher stimulation levels, which was effectively managed through the programming flexibility afforded by the dual-target approach.
Exploratory clinical efficacy (N = 6)
Exploratory efficacy analyses revealed substantial improvements across all clinical outcomes (Table 1, Fig. 2). The mean BFMDRS-Motor score decreased by 78.1%, from 16.8 ± 5.3 at baseline to 3.7 ± 2.4 at LFU (6 months for Patients 1 and 6; 12 months for Patients 2–5) (Cohen's d = 3.2, 95% CI: 1.8–4.5; p = 0.0006). The BFMDRS-Disability score improved by 72.9%, from 9.8 ± 3.9 to 2.7 ± 2.0 (Cohen's d = 2.3, 95% CI: 1.2–3.4; p = 0.0025). Tremor showed the most robust improvement, with the mean FTMTRS score decreasing by 87.1%, from 15.5 ± 5.8 to 2.0 ± 2.3 (Cohen's d = 2.7, 95% CI: 1.5–3.9; p = 0.0012).Fig. 2. Individual severity of dystonia (BFMDRS-M and BFMDRS-D) and tremor (FTMTRS) before surgery (Baseline) versus the last follow-up (LFU) postoperatively. LFU was 6 months after surgery for Patients 1 and 6, and 12 months for Patients 2, 3, 4, and 5. LFU, last follow-up; BFMDRS-M, BFMDRS movement; BFMDRS-D, BFMDRS disability. The bars represent the mean values for each group. P-values for comparisons between Baseline and LFU are analyzed by parametric tests (Student paired-sample t-tests). A p-value of < 0.05 was considered statistically significant
Comparison of efficacy between stimulation conditions (crossover assessment, N = 3)
The blinded crossover assessment in three patients (Patients 2, 5, and 6) provided individual-level data on the differential effects of each stimulation condition (Table 4, Fig. 3). Given the very small sample size, results are presented descriptively with emphasis on individual patient responses. The crossover assessment was performed at 12 months post-surgery for Patients 2 and 5, and at 6 months for Patient 6.Table 4. Comparison of efficacy between single−target and dual−target stimulationPatientTargetBFMDRS−Motor scoreBFMDRS−Disability scoreBFMDRS^a^FTMTRSMean improvement, %(BFMDRS)Mean improvement, %(FTMTRS)Patient 2Stim off13.5821.511PSA on13.5821.51100STN on7411748.836.4Both on246072.1100Patient 5Stim off14122617PSA on851355070.6STN on235380.882.4Both on112192.394.1Patient 6Stim off1412269PSA on8311557.744.4STN on527573.144.4Both on527373.166.7Mean ± SDStim off13.8 ± 0.310.7 ± 2.324.5 ± 2.612.3 ± 4.2PSA on9.8 ± 3.25.3 ± 2.515.2 ± 5.67.0 ± 3.535.9 ± 31.338.3 ± 35.7STN on4.7 ± 2.53.0 ± 1.07.7 ± 3.15.0 ± 2.067.6 ± 16.754.4 ± 24.6Both on2.7 ± 2.12.3 ± 1.55.0 ± 2.71.3 ± 1.579.2 ± 11.486.9 ± 17.8^a^BFMDRS=(BFMDRS−Motor score)+(BFMDRS−Disability score)Fig. 3. Individual BFMDRS movement and disability scores and FTMTRS scores were evaluated under four conditions: Stim off, PSA on, STN on, and Both on. Bars represent group means, with values above indicating the percentage improvement compared to the Stim off condition
Individual patient responses: Patient 2 showed no response to PSA-only stimulation (0% improvement in both BFMDRS and FTMTRS), moderate response to STN-only (BFMDRS: 48.8%; FTMTRS: 36.4%), and excellent response to combined stimulation (BFMDRS: 72.1%; FTMTRS: 100%); Patient 5 demonstrated responses across all conditions, with progressive improvement from PSA-only (BFMDRS: 50.0%; FTMTRS: 70.6%) to STN-only (BFMDRS: 80.8%; FTMTRS: 82.4%) to combined stimulation (BFMDRS: 92.3%; FTMTRS: 94.1%); Patient 6 showed similar dystonia improvement with STN-only and combined stimulation (both BFMDRS: 73.1%), but better tremor control with combined stimulation (FTMTRS: 66.7% vs. 44.4% with STN-only).
Across all three patients, combined PSA + STN stimulation consistently provided the best or equivalent symptom control compared to either target alone. The mean BFMDRS improvement was 35.9% ± 29.1% with PSA-only, 67.6% ± 16.7% with STN-only, and 79.2% ± 9.6% with combined stimulation. The mean FTMTRS improvement was 38.3% ± 32.9% with PSA-only, 54.4% ± 21.9% with STN-only, and 86.9% ± 17.0% with combined stimulation.
When comparing the targets, combined stimulation was more effective than STN stimulation alone for improving both dystonia (79.2% vs. 67.6% improvement, respectively) and tremor (86.9% vs. 54.4% improvement, respectively). These individual patterns suggest that while STN stimulation alone provided substantial benefit, the addition of PSA stimulation offered incremental improvement, particularly for tremor control.
Adverse events
Overall, the surgical procedures were well tolerated in this population. There were no hardware-related side effects, infections, intracranial hemorrhages, or extension or lead fractures from DBS implantation during the follow-up period. Transient, stimulation-induced paresthesia occurred in all six patients during initial programming and subsequent parameter adjustments, but these were resolved by modifying stimulation settings and were not a chronic issue. Specifically, Patient 1 experienced mild STN-induced dyskinesia at higher stimulation levels; this was effectively managed by switching to constant current mode and maintaining a low therapeutic current on that contact. No other common adverse events associated with PSA or STN stimulation were observed at therapeutic settings.
Discussion
In this pilot study, we present the first clinical evidence on the efficacy and safety of a novel single-lead, dual-target DBS approach for medically refractory dystonic tremor (DT). Our primary finding is that this strategy showed substantial improvements in all six patients, yielding clinically significant improvements in both dystonia (mean 78.1% BFMDRS-Motor improvement) and tremor (mean 87.1% FTMTRS improvement). A key aspect of our study was a patient-directed optimization strategy, which provided strong, real-world validation of the dual-target concept: five of six patients independently selected the combined PSA + STN stimulation program as their preferred setting for chronic therapy, while the sixth achieved excellent symptom control using STN-only stimulation.
A critical question arising from our blinded crossover assessment is why a combined PSA + STN approach is necessary if STN stimulation alone proved more potent than PSA-only stimulation for both dystonia and tremor. The answer lies in two key findings. First, while STN-only was superior to PSA-only, exploratory comparisons in the crossover assessment suggested that combined stimulation of both targets may provide additional benefit over STN-only, indicating a potential synergistic effect rather than simple additivity. Second, this synergy is powerfully illustrated by the real-world experience of Patient 1 (who did not participate in the crossover trial). In her self-directed programming, she found optimal relief only when both targets were active, titrating the PSA-area contact to a high level while requiring the STN-area contact at a lower, but indispensable, electrical current to provide synergistic benefit without inducing dyskinesia. It is particularly noteworthy that this outcome in Patient 1 was achieved using an electrode with a shorter total contact span (7.5 mm vs. 10.5 mm) and narrower inter-contact spacing (0.5 mm vs. 1.5 mm) compared to the rest of the cohort. This observation suggests that the dual-target concept may be feasible across different lead geometries and underscores the importance of precise, individualized surgical targeting and programming.
The pathophysiology of DT is increasingly understood as a "dual-network" disorder, involving pathological oscillations in both the basal ganglia-thalamocortical loop (primarily driving dystonia) and the cerebello-thalamo-cortical (CTC) circuit (primarily driving tremor) [8, 19].Our dual-target approach is therefore well positioned to address this dual pathology. The STN is a critical node in the basal ganglia circuit, and its high-frequency stimulation is thought to work by overriding pathological beta-band oscillations and irregular firing patterns, effectively creating an "informational lesion" that regularizes network output [20, 21]. This modulation is likely the primary driver for the profound dystonia improvement we observed. Concurrently, the PSA is a critical intersection for fibers of the CTC circuit, most notably the dentato-rubro-thalamic tract (DRTT). High-frequency stimulation of the PSA is believed to directly disrupt the propagation of pathological tremor-related oscillations [12]. Therefore, the synergistic effect of our single-lead approach likely stems from its ability to simultaneously modulate these two distinct, yet functionally related, pathological circuits with a single device.
The case of Patient 3, who preferred chronic STN-only stimulation and did not undergo the crossover assessment, also provides valuable insight. While a direct, blinded comparison of conditions for this patient is not possible, his preference may reflect a patient-specific profile where the dystonic symptoms were overwhelmingly dominant, and the profound relief from STN stimulation was sufficient for an excellent outcome. Rather than a limitation of the dual-target hypothesis, this outcome underscores the versatility of the surgical strategy. The ability of a single, well-placed lead to provide robust relief—either through selective stimulation of the STN or combined stimulation of both targets—highlights the platform's powerful adaptability to the significant inter-patient heterogeneity inherent in dystonic tremor.
Stimulation-induced dyskinesia (SID) is a recognized adverse effect of STN-DBS in dystonia, with variable incidence across published series. The relatively low rate observed may relate to the dorsal location of our active contacts (mean z = + 1.5 mm), as prior studies have associated more ventral/inferior STN stimulation with higher dyskinesia risk [22, 23]. In addition, the single-lead dual-target approach may reduce the required therapeutic load on the STN contact by allowing symptom control to be distributed across PSA and STN stimulation. In Patient 1, SID at higher STN levels was managed by maintaining lower STN current while increasing PSA stimulation, highlighting the practical value of this programming flexibility.
Several anatomical considerations merit clarification. In this study, the terms ‘PSA contact’ and ‘STN contact’ are used to denote ventral and dorsal positions along a single trajectory rather than strict histological boundaries. As illustrated in Fig. 1C, the VTA of the ventral ‘PSA’ contact primarily encompasses the posterior subthalamic area and caudal zona incerta, with partial extension into the ventromedial border of the STN, whereas the VTA of the dorsal ‘STN’ contact primarily involves the dorsal border of the STN and adjacent zona incerta/Forel region. This dorsal subthalamic stimulation site is in line with recent observations [5, 23, 24] that effective stimulation for dystonia often lies at or above the dorsal STN border within the zona incerta-subthalamic region. The inevitable overlap of VTAs across these closely packed structures represents an inherent limitation of conventional omnidirectional DBS electrodes and precludes precise attribution of clinical effects to a single subregion. Future studies employing directional leads and higher-resolution imaging may help to more precisely dissect the respective contributions of PSA/cZI, dorsal STN, and zona incerta modulation.
Several limitations should be acknowledged. This study's primary contribution is demonstrating the feasibility of a novel dual-target DBS approach. While exploratory efficacy improvements were substantial, the retrospective design, small sample size (N = 6), and single-center nature preclude definitive efficacy conclusions. The heterogeneity in follow-up timing (6 vs. 12 months), final chronic stimulation programs (combined PSA + STN in 5/6 vs. STN-only in 1/6), and electrode models (SR1200 vs. SR1210) introduces additional variability and may confound cross-patient comparisons in this retrospective series. Genetic testing was not performed; however, given the adult-onset presentation, focal/segmental distribution, and absence of atypical features, the likelihood of identifying a monogenic cause is low. The crossover assessment has specific limitations. The 30 min wash-in/wash-out intervals align with established evidence for rapid tremor responses but are insufficient for complete dystonia assessment; the short-term dystonia improvements observed may reflect acute suppression of phasic dystonic movements. In addition, only three of six patients participated due to personal time constraints or concerns about the extended assessment duration.
Additionally, we did not incorporate formal, time-stamped assessments to quantify the differential onset of improvement for tremor versus dystonia. Literature suggests that tremor responds to PSA/VIM stimulation within seconds [25–28], while dystonia improvement with GPi-DBS typically evolves over weeks to months. However, STN-DBS has been associated with relatively earlier dystonia improvement, with significant benefit observed within the first month [5]. In our cohort, tremor suppression was clinically evident during monopolar screening and the crossover assessment. Short-term reductions in dystonia-related manifestations were also observed in some patients during these evaluations, which may reflect acute suppression of phasic or tremor-coupled dystonic components rather than the full temporal evolution of tonic dystonia. These observations should therefore be interpreted cautiously and considered hypothesis-generating. Future prospective studies should incorporate standardized follow-up intervals, genetic evaluation, objective tremor quantification, extended washout intervals for dystonia assessment, and systematic early assessments to characterize the time course of improvement for each symptom component.
In conclusion, this retrospective pilot study provides strong preliminary evidence that a single-lead, dual-target DBS approach for the PSA and STN is an effective and safe strategy for dystonic tremor. This novel method successfully addresses both dystonic and tremor symptoms and, through a flexible, patient-directed programming paradigm, demonstrates significant potential for truly personalized therapy. While promising, these findings now require validation through larger, multi-center, randomized controlled trials to definitively establish the efficacy of this therapeutic approach.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 15 KB)