Risk factors for skeletal-related events in patients with stage IV lung adenocarcinoma and bone metastases receiving denosumab: a retrospective cohort analysis
Hui Zhang, Daochen Wen, Zhou Liao, Xiaoyong Tan, Hao Wang, Jianxia Xiang, Bing Yan

TL;DR
The study identifies risk factors for bone-related complications in lung cancer patients treated with denosumab, highlighting the protective role of bisphosphonate use and risks from low blood calcium and smoking.
Contribution
First study to show bisphosphonate use protects against skeletal events during denosumab treatment in lung cancer patients with bone metastases.
Findings
A prior history of bisphosphonate use reduces the risk of skeletal-related events during denosumab treatment.
Pretreatment hypocalcemia and smoking are significant risk factors for skeletal-related events.
24.3% of patients experienced skeletal-related events during follow-up.
Abstract
This study aimed to identify independent risk factors for skeletal-related events(SREs) during denosumab treatment in patients with bone-metastatic stage IV lung adenocarcinoma by integrating multidimensional clinical parameters, thereby providing an evidence-based foundation for risk stratification and targeted management. In this retrospective cohort study, patients with stage IV lung adenocarcinoma and radiologically confirmed bone metastases diagnosed at Xuanhan County People's Hospital between July 2021 and December 2023 were enrolled. All patients received standardized denosumab therapy (120 mg subcutaneously every 4 weeks ± 7 days). Baseline demographic, laboratory, and treatment response data were extracted from the electronic medical record system. Univariate analyses were used to screen candidate variables, followed by multivariate logistic regression to identify independent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
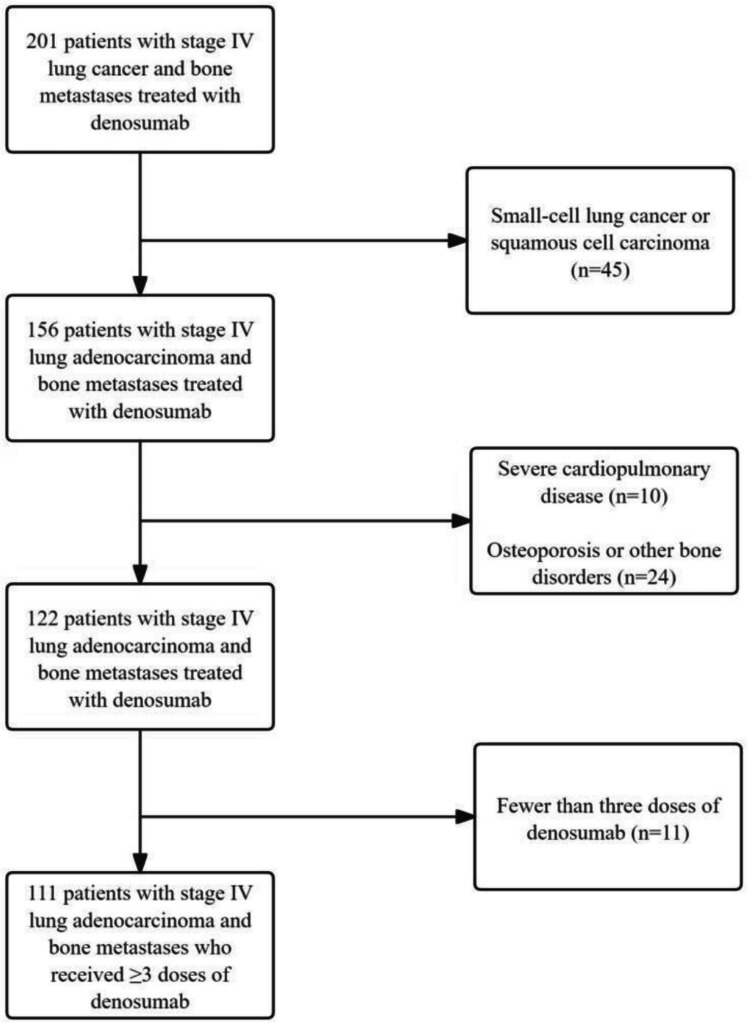 Figure 1
Figure 1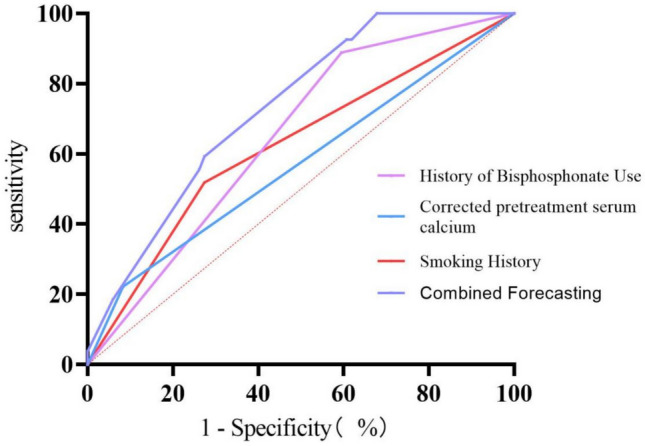 Figure 2
Figure 2- —Xuanhan County Science and Technology Plan Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone health and treatments · Management of metastatic bone disease · Medical Imaging and Pathology Studies
Introduction
Lung cancer remains the leading cause of cancer-related mortality worldwide, with its disease burden continuing to rise. According to the Global Cancer Statistics 2022, approximately 2.47 million new cases and 1.76 million deaths from lung cancer were reported globally, accounting for 18.7% of all cancer-related deaths [1]. In China, lung cancer also ranks first in cancer-related mortality, with non–small-cell lung cancer (NSCLC) comprising approximately 85% of all cases [2]. At the time of initial diagnosis, bone metastases are present in approximately 67% of patients with NSCLC, and over half will experience skeletal-related events (SREs) during the disease course [3]. Among NSCLC subtypes, lung adenocarcinoma demonstrates a significantly higher incidence of bone metastases than other histological variants [4]. SREs—which include pathologic fractures, spinal cord compression, bone pain requiring therapeutic intervention, and hypercalcemia—are severe complications that not only substantially impair quality of life but also accelerate disease progression through interactions within the tumor–bone microenvironment, ultimately shortening overall survival [5, 6]. The prevention and mitigation of SREs have thus become central objectives in the comprehensive management of bone-metastatic lung cancer.
Denosumab, a fully human monoclonal antibody targeting receptor activator of nuclear factor-κB ligand (RANKL), inhibits osteoclast-mediated bone resorption by selectively blocking the RANKL–RANK signaling pathway. It is recommended as a first-line bone-targeted agent in patients with solid tumors and bone metastases according to international guidelines [7, 8]. Phase III trials have demonstrated that denosumab significantly delays the time to first SRE and reduces the cumulative risk of subsequent events compared with zoledronic acid in patients with stage IV NSCLC [8, 9]. However, in the subset of patients with stage IV lung adenocarcinoma—a population characterized by a high burden of osseous metastasis and distinct molecular features (e.g., > 50% EGFR mutation rate)—clinical response to denosumab is notably heterogeneous. This observation highlights the need for biomarker-driven stratification strategies to optimize therapeutic decision-making.
Although prior studies have identified several clinical predictors of SREs in patients with NSCLC and bone metastases—including the number of osseous lesions, Eastern Cooperative Oncology Group (ECOG) performance status, smoking history, and hypercalcemia [10–12]—these investigations have notable limitations. First, most existing evidence is derived from heterogeneous NSCLC cohorts without histologic stratification; the distinct molecular characteristics of lung adenocarcinoma, such as high EGFR mutation frequency, may uniquely influence bone microenvironmental dynamics and therapeutic responses, necessitating subtype-specific analyses. Second, few real-world studies have focused specifically on the subset of patients with stage IV lung adenocarcinoma receiving denosumab. To address these gaps, we conducted a retrospective cohort study of 111 patients with bone-metastatic stage IV lung adenocarcinoma treated with denosumab to identify independent predictors of SREs, with a novel focus on the high osseous metastatic burden unique to this clinical population. The findings aim to inform precision bone-targeted therapy in advanced lung adenocarcinoma.
Methods
Study design and participants
This single-center retrospective cohort study included consecutive patients with bone-metastatic stage IV lung adenocarcinoma treated with denosumab at Xuanhan County People’s Hospital between July 1, 2021, and December 31, 2023. Eligible patients met the following criteria: (1) age ≥ 18 years; (2) pathologically or cytologically confirmed stage IV lung adenocarcinoma, according to the 8th edition of the American Joint Committee on Cancer (AJCC) staging system; (3) radiologic evidence of bone metastasis or osteolytic lesions (confirmed by CT, MRI, or PET-CT); and (4) no planned orthopedic surgery or palliative radiotherapy to bone. Exclusion criteria included: (1) severe cardiopulmonary dysfunction (New York Heart Association [NYHA] class III–IV heart failure or Global Initiative for Chronic Obstructive Lung Disease [GOLD] stage 4 COPD); and (2) preexisting bone metabolic disorders (such as osteoporosis or Paget’s disease) or a history of prior major skeletal fractures. The study protocol was approved by the Ethics Committee of Xuanhan County People’s Hospital (Approval No. 2022-KSSC-0005). In accordance with the principles of the Declaration of Helsinki, written informed consent was obtained from all enrolled patients prior to the initiation of the study.
Treatment and follow-up protocol
All patients received systemic therapy according to the 2021 edition of the Chinese Society of Clinical Oncology (CSCO) Guidelines for the Diagnosis and Treatment of Non–Small-Cell Lung Cancer. Denosumab was administered subcutaneously at a dose of 120 mg every 4 weeks (± 7 days). Baseline demographic characteristics, laboratory results, and treatment response data were extracted from the hospital’s electronic medical record system. Treatment continued until the occurrence of intolerable toxicity or disease progression. The follow-up period extended to December 1, 2024. Patients were monitored using a standardized follow-up protocol: (1) medication use and SREs were assessed every 4 weeks; (2) bone metastases were evaluated every 6 months using whole-body bone scintigraphy (99mTc-MDP SPECT/CT) or 18F-FDG PET-CT; and (3) after 12 months of treatment, skeletal evaluation was performed every 3 months using bone CT. Follow-up information was obtained via telephone, text message, outpatient visits, or review of the electronic medical record system.
Study variables
Key variables of interest included: age, sex, smoking history, Eastern Cooperative Oncology Group performance status (ECOG-PS; ≤ 1 vs. ≥ 2), number of visceral metastatic sites (≤ 1 vs. ≥ 2), type of bone metastasis (osteolytic, osteoblastic, or mixed), genetic mutation status, serum albumin (normal: 35–50 g/L), corrected pretreatment serum calcium (≥ 8.50 mg/dL vs. < 8.50 mg/dL), alkaline phosphatase (normal: 40–150 U/L), lymphocyte count (normal: 1.0–4.8 × 10⁹/L), treatment modality (targeted therapy vs. chemotherapy plus antiangiogenic agents or immune checkpoint inhibitors vs. other therapies), prior bisphosphonate use and its treatment duration. The primary endpoint was the occurrence of skeletal-related events (SREs) during denosumab therapy, defined according to the American Society of Clinical Oncology (ASCO) guidelines as any of the following: (1) pathologic fracture (confirmed independently by two radiologists); (2) spinal cord compression (jointly evaluated by neurologists and orthopedic surgeons); (3) bone pain requiring intervention (numerical pain rating ≥ 4 and treated with radiotherapy); or (4) hypercalcemia (corrected calcium > 11 mg/dL or > 2.75 mmol/L).
Statistical analysis
All statistical analyses were performed using SPSS version 26.0 (IBM Corp., USA). The Shapiro–Wilk test was used to assess the normality of continuous variables. Normally distributed data were expressed as means ± standard deviation and compared using the independent-samples t test. Non-normally distributed data were reported as medians and interquartile ranges [M (IQR)] and compared using the Mann–Whitney U test. Categorical variables were expressed as counts and percentages [n (%)] and compared using the chi-square test or Fisher’s exact test as appropriate. Variables with P < 0.10 in univariate analyses were entered into a multivariate logistic regression model using forward stepwise selection (entry criterion: likelihood ratio P < 0.05; removal criterion: P ≥ 0.10). Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. All hypothesis testing was two-sided, and P < 0.05 was considered statistically significant.
Results
Patient selection
Of 201 patients screened, 90 were excluded for the following reasons: small cell or squamous cell carcinoma (n = 45); presence of severe cardiopulmonary comorbidities, osteoporosis, or other bone disorders (n = 34); or fewer than three doses of denosumab (n = 11). A total of 111 eligible patients were included in the final analysis (Fig. 1).Fig. 1. Flow diagram of patient selection and enrollment
Baseline characteristics
Baseline characteristics are summarized in Table 1. The median age was 65.5 years (range, 53–73), with 56 men (50.45%) and 55 women (49.55%). The median BMI was 22.63 kg/m^2^ (IQR, 21.22–24.44), and 74 patients (66.67%) had normal body weight (18.5–24 kg/m^2^). A majority (66.67%, n = 74) were never smokers. Most patients (88.29%) had good performance status (ECOG 0 in 31.53%, ECOG 1 in 47.75%). At baseline, 68 patients (61.26%) had already experienced an SRE, Among these patients, 40 presented with isolated bone pain, while 27 had bone pain complicated by either fracture or spinal cord compression. Only one patient presented with isolated fracture without concomitant bone pain. 73 patients (65.77%) had additional sites of metastasis. Osteolytic lesions were the predominant type of bone metastasis (53.15%). A total of 49 patients had confirmed genetic alterations (e.g., EGFR, ALK, or ROS1). Forty-nine patients (44.14%) received targeted therapy, while the remainder received chemotherapy, antiangiogenic therapy, or immunotherapy (monotherapy or in combination). Prior bisphosphonate therapy was documented in 37 patients (33.33%),Among these patients, 33 (89.2%) received zoledronic acid as the primary treatment, while the remaining cases included ibandronate (n = 3) and pamidronate (n = 1). The median treatment duration was 2.6 months. Table 1. Baseline characteristics and univariate analysis of skeletal-related events (SREs) in stage IV lung adenocarcinoma patients with bone metastases receiving denosumabVariablesNo SRE Group (n = 84)SRE Group (n = 27)PSexMale41(48.81)15(55.56)0.659Female43(51.19)12(44.44)Age (Years)65.5(20.00)65.50(18.00)0.652BMI(kg/m^2^) < 18.55(6.00)1(3.70)0.80518.5 ~ 2457(67.90)17(63.00) ≥ 2422(26.20)9(33.30)Smoking HistoryNo61(72.60)13(48.10)0.033Yes23(27.40)14(51.90)Eastern Cooperative Oncology Group Performance Status (score)0–174(88.10)24(88.90)1.0002–310(11.90)3(11.10)History of Skeletal-Related Events (SREs)No32(38.10)11(40.70)0.806Yes52(61.90)16(59.30)Number of Visceral Metastatic Sites ≤ 155(65.50)17(63.0)0.812 ≥ 229(34.50)10(37.00)Type of Bone MetastasisOsteolytic40(47.60)19(70.40)0.100Osteoblastic27(32.10)6(22.20)Mixed17(20.20)2(7.40)Genetic Mutation StatusAbsent47(55.95)15(55.56)0.971Present37(44.05)12(44.44)Treatment RegimenTargeted Therapy37(44.00)12(44.40)0.334Chemotherapy plus Antiangiogenic Agents/ICIs26(31.00)5(18.50)Other Therapies21(25.00)10(37.00)History of Bisphosphonate UseAbsent50(59.50)24(88.90)0.005Present34(40.50)3(11.10)Duration of bisphosphonate therapy(months) < 653(63.1)18(66.7)0.2496 ~ 923(27.4)4(14.8) ≥ 98(9.5)5(18.5)Serum Albumin (g/L)40.75 ± 4.2639.83 ± 4.040.322Lymphocyte Count (10⁹/L)1.08(0.63)1.22(0.47)0.392Alkaline Phosphatase (U/L)103.5(60.3)112.0(37.0)0.201Corrected pretreatment Serum Calcium (mg/dL) ≥ 8.5077(91.67)21(77.78)0.08 < 8.507(8.33)6(22.22)Exact probability methods were used for variables marked with an asterisk (*); categorical variables were analyzed using the chi-square test. Serum albumin, as a continuous variable with normal distribution, was analyzed using the t test, while other continuous variables were assessed using the Wilcoxon rank-sum test
Incidence of skeletal-related events
During denosumab treatment, 27 patients (24.32%) experienced SREs. These included 17 cases of bone pain requiring radiotherapy (62.96%), 4 cases of spinal cord compression (14.81%), 3 cases of pathologic fracture (11.11%), and 3 patients who required orthopedic surgery (11.11%).
Risk factor analysis for SREs
In univariate analysis, smoking history (P = 0.033), prior bisphosphonate use (P = 0.005), and pretreatment hypocalcemia (P = 0.008) were significantly associated with SRE risk (Table 1).
In multivariate logistic regression analysis, prior use of bisphosphonates was independently associated with a reduced risk of SREs (OR, 0.191; 95% confidence interval CI, 0.049–0.741 P = 0.017). In contrast, pretreatment hypocalcemia (OR, 4.913; 95% CI, 1.268 ~ 19.044; P = 0.021) and smoking history (OR, 3.078; 95% CI, 1.131 ~ 8.378; P = 0.028) emerged as independent risk factors for the development of SREs during denosumab therapy.The final multivariate logistic regression model demonstrated good fit according to the Hosmer–Lemeshow test (χ^2^ = 4.519, df = 7, P = 0.718). Denosumab treatment duration was retained as a covariate in the multivariate logistic regression model due to its clinical relevance and potential confounding effects, despite not reaching statistical significance in univariate analysis(p = 0.249). Existing evidence suggests an association between treatment duration and bone metastasis progression, and this variable may influence the effect estimates of other predictors. Including this covariate enables more accurate estimation of independent variable effects and enhances the model's clinical applicability and interpretability (Table 2). Table 2. Result of Logistic regression modelVariables*P**OR (*95%*CI)*Smoking HistoryNo--Yes0.0283.078(1.131 ~ 8.378)History of Bisphosphonate UseNo--Yes0.0170.191(0.049 ~ 0.741)Corrected pretreatment Serum Calcium (mg/dL) ≥ 8.50-- < 8.500.0214.913(1.268 ~ 19.044)Duration of bisphosphonate therapy(months) < 66 ~ 90.150.385 (0.105 ~ 1.413) ≥ 90.5021.586 (0.413 ~ 6.088)
Based on the multivariate logistic regression model, individualized predicted probabilities for skeletal-related events (SREs) were calculated for each patient. Receiver operating characteristic (ROC) curve analysis demonstrated that the predictive model had moderate discriminative ability, with an area under the curve (AUC) of 0.731 (95% CI: 0.633–0.829), which was statistically significant (P < 0.001). The optimal predicted probability cutoff value of 8.67% was determined by maximizing the Youden index. At this threshold, the model exhibited a sensitivity of 100.0% and a specificity of 32.1% for identifying patients with SREs (Fig. 2).Fig. 2. Receiver operating characteristic (ROC) curve for the model of risk factors
Discussion
Skeletal-related events (SREs) are common and serious complications in patients with stage IV lung adenocarcinoma and bone metastases, substantially impairing quality of life and worsening survival outcomes [13–15]. Although denosumab, a RANKL inhibitor, effectively reduces the incidence of SREs [16, 17], substantial interindividual variability in treatment response exists, and validated predictive models remain lacking. In this study, we conducted multivariable analysis specifically in patients receiving denosumab and suggested prior bisphosphonate use as an independent protective factor (OR, 0.191), while pretreatment hypocalcemia (OR, 4.913) and smoking (OR, 3.078) were independently associated with increased risk of SREs. These findings support the development of risk stratification models and individualized monitoring strategies.
Previous studies have established the efficacy of bisphosphonates in mitigating osteolytic activity through osteoclast inhibition [18], though most prior research has focused on their role as monotherapy for bone metastases [19, 20]. Our study is the first to demonstrate that a history of bisphosphonate use prior to denosumab administration—such as with zoledronic acid—significantly reduces the risk of SREs (OR, 0.191), thereby extending the clinical utility of bisphosphonates. Given that bisphosphonates may influence SRE occurrence by inducing hypocalcemia, we further analyzed their impact on pre-treatment hypocalcemia. The results showed no significant association between prior bisphosphonate use and the incidence of pre-treatment hypocalcemia before denosumab therapy (p = 0.538). This negative finding may be attributed to the relatively short duration of bisphosphonate therapy in our cohort (median 2.6 months), which might be insufficient to exert long-term effects on calcium metabolism. Furthermore, this retrospective analysis has inherent limitations, including incomplete documentation of calcium and vitamin D supplementation. Future prospective studies with systematic long-term data collection on drug metabolism are warranted to validate these findings..Additionally,, emerging evidence suggests that sequential bisphosphonate therapy following prolonged denosumab use may maintain skeletal homeostasis, minimize bone loss, and mitigate the risk of rebound bone turnover upon discontinuation [21, 22]. In light of these findings, clinicians should consider the potential additive value of bisphosphonates when designing bone-targeted strategies for patients with stage IV lung adenocarcinoma and bone metastases, particularly those at high risk for SREs or undergoing treatment transitions.
Our study also identified pretreatment hypocalcemia, defined as a corrected serum calcium level < 8.50 mg/dL, as an independent risk factor for SREs (OR, 3.877). The underlying pathophysiological mechanism may involve disruption of skeletal calcium homeostasis, leading to increased bone fragility and a heightened risk of pathologic fractures and related complications. This may be mediated by elevated bone turnover markers such as C-terminal telopeptide of type I collagen (CTX-1) and suppressed osteocalcin (OC) synthesis [23]. Denosumab itself has been associated with a higher risk of treatment-emergent hypocalcemia [24, 25], which may further predispose patients to SREs. Ulas et al. [10]reported that baseline hypercalcemia was inversely associated with SRE risk (OR, 0.33), supporting the present findings. Additionally, Dennis et al. (2020) [26]showed that baseline vitamin D deficiency (25-OH-vitamin D < 20 ng/mL) significantly impaired intestinal calcium absorption and renal calcium reabsorption via downregulation of calbindin-D9k, increasing the risk of hypocalcemia during bone-modifying therapy (OR, 2.546; P = 0.023). That study also confirmed a protective effect of pre-treatment hypercalcemia (serum calcium > 10.2 mg/dL, OR, 0.474; P = 0.032) against developing hypocalcemia. These mechanistic insights suggest that during denosumab therapy, clinicians should: (1) dynamically monitor serum calcium and 25-OH-vitamin D levels; and (2) implement calcium supplementation strategies in patients with persistent hypocalcemia to optimize skeletal metabolism and reduce the risk of SREs.
Smoking is known to impair bone homeostasis through multiple pathologic mechanisms, including enhanced osteoclast activation and reduced intestinal calcium absorption. Experimental studies have shown that cadmium and nicotine in tobacco smoke can suppress the Wnt/β-catenin signaling pathway, thereby disrupting the coupling of bone formation and resorption [27]. Clinical evidence also links smoking to elevated SRE risk. A Korean cohort study demonstrated that non-small cell lung cancer (NSCLC) patients with a smoking history had a significantly higher SRE incidence than nonsmokers (OR, 2.80; 95% CI, 1.32–6.00) [12]. Our study further establishes that this association holds true for the specific population of patients with bone-metastatic stage IV lung adenocarcinoma undergoing denosumab treatment, in whom smoking was identified as an independent predictor (OR, 3.078; 95% CI, 1.131–8.378; P = 0.028). This may reflect a pharmacodynamic antagonism between tobacco-induced upregulation of RANKL signaling and RANKL inhibition by denosumab. Consequently, smoking status should be incorporated into SRE risk assessment tools, and smoking cessation should be strongly reinforced during antiresorptive therapy.
This study established a predictive model for assessing skeletal-related event (SREs) risk in patients with bone-metastatic lung adenocarcinoma by incorporating smoking history, pretreatment hypocalcemia, and prior bisphosphonate use. The model demonstrated good discriminative capacity, with an area under the curve (AUC) of 0.731. The optimal decision threshold was determined as 8.67% using the Youden index. At this cutoff value, the model achieved 100% sensitivity while maintaining limited specificity (32.1%), ensuring comprehensive identification of high-risk patients. This quantitative tool provides an objective basis for clinical risk stratification, facilitates intensified monitoring of high-risk individuals and optimized allocation of medical resources, thereby offering practical evidence for precision management in supportive cancer care.
Several limitations of this study merit consideration. First, as a single-center retrospective analysis with a relatively modest sample size (n = 111), our findings may be subject to selection and information biases. Second, although prior bisphosphonate use emerged as a strong predictor, we did not stratify by dose, duration, or transition regimens (e.g., zoledronic acid 4 mg vs. 8 mg), which may limit the generalizability of our findings. Future studies should adopt multicenter prospective cohort designs with larger sample sizes, incorporate pharmacokinetic variables (e.g., denosumab dosing intervals), and include genomic data (e.g., RANKL expression levels or vitamin D receptor polymorphisms),to improve model specificity while maintaining high sensitivity, thereby establishing a more clinically applicable risk prediction tool.
Conclusion
In this retrospective study of patients with stage IV non–small-cell lung cancer and bone metastases treated with denosumab, prior bisphosphonate use was identified as an independent protective factor against skeletal-related events (OR, 0.191), while pretreatment hypocalcemia (OR, 4.913) and smoking (OR, 3.078) were independently associated with elevated risk. These findings underscore the importance of risk stratification and enhanced surveillance in vulnerable patient subgroups.