The role of high-sensitivity troponin in identifying patients with cardiac allograft rejection
André A. Scussel, Fabiana G. Marcondes-Braga, Cristhian V. Espinoza Romero, Daniel C. de Marchi, Mônica Samuel Ávila Grinberg, Fernanda Barone Alves do Santos, Ana Maria Peixoto Cardoso Duque, Sandrigo Mangini, Luís Fernando Bernal Seguro, Iáscara Wozniak Campos, Fabio Gaiotto

TL;DR
This study shows that high-sensitivity troponin I can help identify heart transplant patients with acute rejection, especially in a Latin American population with diverse causes like Chagas disease.
Contribution
The study is the largest Latin American cohort to assess hs-TnI after heart transplant and the first to explore its performance in specific etiologies including Chagas disease.
Findings
Higher hs-TnI levels were significantly associated with acute cellular rejection (ACR >2R) compared to lower grades.
A cutoff of 19 ng/L for hs-TnI showed 88% sensitivity and 92% negative predictive value for ACR >2R.
hs-TnI demonstrated significant discriminatory power for ACR >2R in patients with Chagas disease.
Abstract
Biomarkers for acute rejection diagnosis are frequently searched, and data from medical literature are conflicting. The role of high-sensitivity troponin I in the diagnosis of acute cellular rejection (ACR) after heart transplant (HT) is uncertain. However, it is a widely used and accessible tool in developing countries. This study aims to determine whether hs-TnI can serve as a reliable and accessible tool to identify patients with clinically significant rejection (ACR >2R) in a real-world Latin American cohort that has different etiologies than the epidemiology of the main trials. In this retrospective cohort, we evaluated data from electronic records of HT recipients submitted to HT from March, 2020 to September, 2022 using REdCAp database. All patients who underwent endomyocardial biopsies (EMB) between 3 months and 2 years of HT and had samples of HS-troponin I previously…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
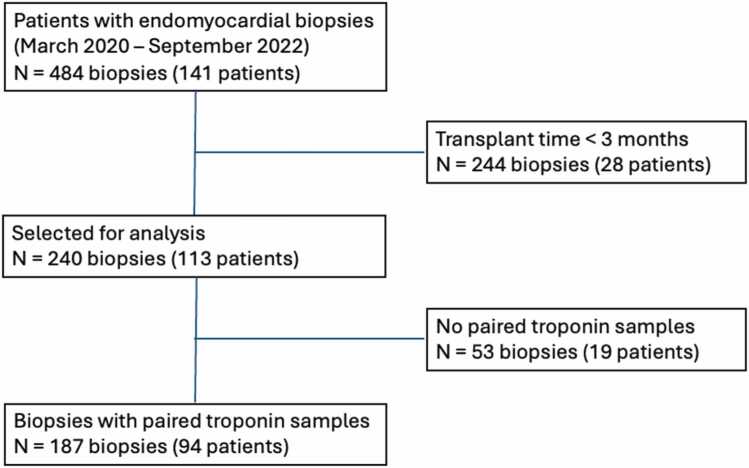 Figure 1
Figure 1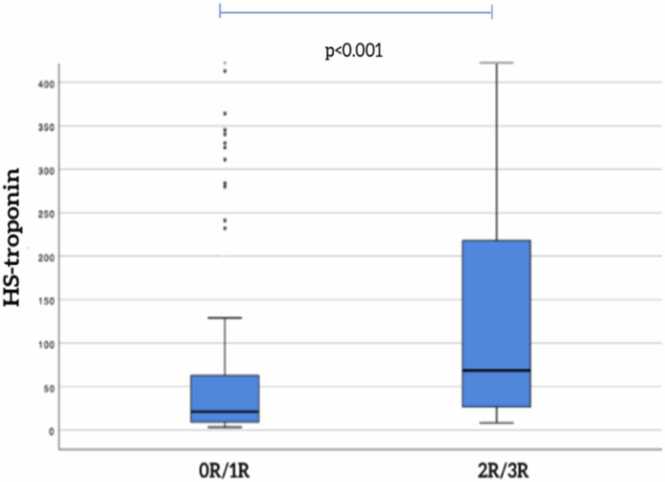 Figure 2
Figure 2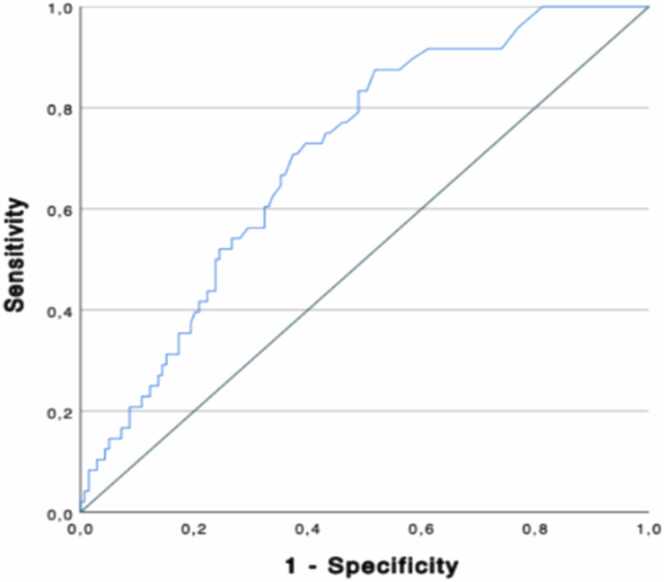 Figure 3
Figure 3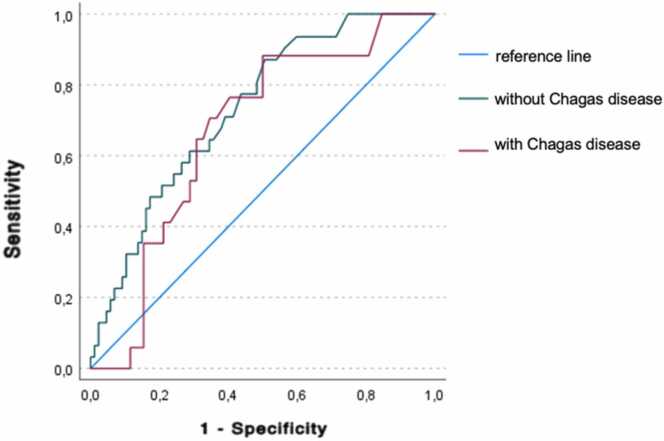 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Mechanical Circulatory Support Devices · Immune Response and Inflammation
Heart transplantation (HT) has become a life-saving therapeutic option for patients with end-stage heart failure (HF). However, acute cellular rejection (ACR) remains a significant concern in the first year following transplantation, affecting approximately 30% of recipients and often presenting with asymptomatic features.1 Early recognition and timely treatment of ACR are crucial to improve long-term outcomes and graft survival.1 Currently, endomyocardial biopsy (EMB) serves as the gold standard for diagnosing ACR.1, 2 Despite its diagnostic accuracy, EMB is an invasive procedure with associated risks and limitations as an interobserver variability by pathologists and tricuspid valve lesions.3, 4 The need for less invasive diagnostic tests with reasonable predictive capacity has led to the investigation of alternative biomarkers.
Among the noninvasive tests assessed, the gene expression profile (Allomap) has demonstrated promising results for ACR surveillance, comparable to EMB. However, the practicality of Allomap is restricted by its low positive predictive value, high cost, and time-consuming process.5, 6 Another method for ACR monitoring is the measurement of donor-derived cell-free DNA, which can assist in detecting both ACR and antibody-mediated rejection (AMR).16 However, it has similar practical limitations in terms of cost and availability.
The role of high-sensitivity troponin (hs-TnI) as a potential diagnostic biomarker for various cardiovascular conditions has gained considerable attention.7 Cardiac troponins I and T, sarcomeric structural proteins, are released into the bloodstream following myocardial injury and cardiomyocyte damage.7 With the advent of hs-Tn assays, boasting 10 times greater sensitivity than conventional tests, hs-Tn exhibits favorable sensitivity and negative predictive value.2 For this reason, the recent guidelines of the International Society of Heart and Lung Transplantation (ISHLT) recommend the integration of biomarkers such as high-sensitivity troponin into a rejection monitoring strategy to identify higher-risk patients who may benefit from further evaluation for ACR.8, 9 This study aims to determine whether hs-TnI can serve as a reliable, accessible tool for identifying patients with clinically significant rejection (ACR >2R) in a real-world Latin American cohort. The high sensitivity and negative predictive value of hs-TnI offer promising prospects for a noninvasive and reliable diagnostic tool, enabling early identification and management of ACR in patients with HT.
Methods
Study design, setting, and participants
This is a single-center retrospective cohort study in which we evaluated data from electronic records of patients of our institution that were submitted to HT between March 2020 and September 2022. We analyzed values of hs-TnI measured until 48 hours before EMB and their association with ACR incidence. Evidence suggests that biomarker measurements within the first 3 months postheart transplant lack reliability due to a high incidence of false positives. This can be attributed to the continuous release of troponin observed over a 2 to 3 months period following heart transplantation.16 Therefore, biopsies performed before 3 months of heart transplant were excluded. The flowchart of the study is represented below.
Statistical analysis
All statistical analyses were performed using SPSS for Windows, version 26.0. Categorical variables were expressed as absolute (n) and relative frequencies (%), and were compared using the Pearson’s Chi-square test. Numerical variables were initially tested for normality using the Kolmogorov-Smirnov test with Lilliefors correction to assess normality.
Variables with normal distribution were presented as mean ± standard deviation (SD) and compared between groups using the independent samples Student’s t-test. Non-normally distributed variables were expressed as median and interquartile range (IQR), and compared using the Mann-Whitney U test.
To evaluate the diagnostic accuracy of troponin levels in predicting rejection, receiver operating characteristic (ROC) curve analysis was performed. The area under the ROC curve (AUC) was calculated to assess sensitivity, specificity, and overall diagnostic performance.
The institutional ethical committee approved the study (CAAE:42622215.9.0000.0068).
Results
In this analysis, we included data from 187 biopsies performed at least 3 months after HT in 94 recipients who had paired Hs-troponin I samples collected. Clinical data are shown in Table 1.Table 1. Clinical and Demographic Data of Heart Transplant Patients in This CohortTable 1Patients’ characteristics (n = 94)ValueAge at heart transplant (y)48.0 ± 10.7Male sex n (%)54 (57.4)Etiology of Cardiomyopathy (n [%]) Dilated41 (43.6) Chagas Disease34 (36.2) Ischemic8 (8.5) Other11 (11.7)Donor age (y)29.8 ± 9.5Donor male sex (%)72 (76.6)Heart transplant in priority condition (n [%]) Total93 (98.9) Inotropes47 (50.0) IABP40 (42.6) Other6 (6.4)CM, cardiomyopathy; IABP, intraaortic balloon pump. Numerical variables are expressed as mean ± standard deviation or median and interquartile range, depending on the result of the normality test.
The median hs-TnI levels were 29(1(11−118)g/L. ACR >2R was observed in 48 EMB and the median hs-TnI levels were 69(2(26−224)g/L, which was significantly higher than levels observed in patients with grade 0R/1R [21(9 (9−64)g/L, p<0.001 (Figure 1).Figure 1. Flowchart of the studyFigure 1
The characteristics of patients with treated rejection (EMB >2R) or no rejection did not differ in terms of ejection fraction or the presence of RV dysfunction. However, we observed a higher level of serum creatinine in the group of no rejection (Table 2).Table 2. Characteristics of Patients According to Acute Cellular Rejection GroupTable 2VariablesEMB <2R (n = 48)EMB ≥2R (n = 139)pAge (y)49 (40-56)50 (36-56)0.889Echocardiogram findings LVEF (%)61 (55-65)62 (60-65)0.197 RV dysfunction (%)15 (10.8)7 (14.6)0.482Lab tests HS-troponin I (ng/L)21 (11-118)69 (26-224)<0.001 Serum Creatinine (mg/dl)1.50 (1.14-2.03)1.30 (1.08-1.68)0.032Numerical variables are expressed as mean ± standard deviation or median and interquartile range, depending on the result of the normality test.
The ROC curve (depicted in Figure 2) for HS-troponin I indicates an AUC of 0.705, with a p-value of <0.001 for diagnosing ACR ≥2R. Using a cutoff value of 19 ng/L, hs-TnI yielded a sensitivity of 88% and a specificity of 49%, corresponding to a negative predictive value of 92% in this population. Figure 3, Figure 4.Figure 2. Hs-TnI levels according to rejection gradeFigure 2Figure 3ROC curve for hs-TnI in predicting rejectionFigure 3Figure 4ROC curve for hs-TnI in predicting rejection in Chagas disease subgroupFigure 4
The performance of hs-TnI was also analyzed in specific subgroups, including patients with Chagas disease, a population often underrepresented in heart transplant studies. Among these patients, hs-TnI levels were significantly higher in biopsies with ACR >2R [42 ng/L (28-(28−72) compared to those with grade 0R/1R [23 ng/L (11-(11−46) = 0.037). The ROC curve in this subgroup showed an AUC of 0.669 (p = 0.016). No statistically significant difference was observed between the ROC curves of patients with and without Chagas disease (Z-test, p = 0.464).
Discussion
The main findings of the current study were
- (i)The hs-TnI levels in patients with ACR >2R were significantly higher than levels observed in patients with grade 0R/1R;
- (ii)A cutoff value of 19 ng/L for hs-TnI demonstrated a sensitivity of 88% and a specificity of 49% for diagnosing ACR;
- (iii)hs-TnI levels were also significantly elevated in patients with ACR >2R within specific subgroups, such as those with Chagas disease.
The high incidence of ACR during the first posttransplant year underscores the need for reliable diagnostic methods with minimal invasiveness.10 However, biomarker measurements within the first 3 months after the procedure may lead to false positives.10 To address this issue, we reviewed 2 recent meta-analyses, involving a total of 993 and 840 patients, respectively, with significant cellular rejection (defined as ≥2R).2, 11 These studies evaluated the use of conventional troponin (TnC) and hs-TnI in diagnosing ACR. While the use of hs-TnI showed a higher sensitivity and negative predictive value compared to TnC, it also exhibited some limitations, such as high heterogeneity and retrospective nature of some studies.2, 11 Further investigations showed that hs-TnI concentrations were significantly higher in rejection versus nonrejection samples, demonstrating their potential as a diagnostic marker.11 In a retrospective study of 98 patients, hs-TnI showed a sensitivity of 94% and negative predictive value of 99% when adjusted for a cutoff of 15 ng/L.12 Similar results were obtained in another study with a sensitivity of 80% and a negative predictive value of 96%.13
In comparison to noninvasive methods like gene expression profiling (AlloMap), hs-TnI demonstrated excellent negative predictive value and sensitivity in appropriate low-risk patients.14 Although those tools have shown good performance in rejection surveillance, their high costs limit their use, particularly in low-resource settings. In such scenarios, protocols incorporating hs-TnI in selected low-risk patients — ideally within a multimodal approach that includes BNP measurement and transthoracic echocardiography — may help reduce the need for EMB or gene expression profiling.14, 15
While similar studies have been conducted in other populations, this is the first and largest to investigate heart transplant recipients in a Latin American cohort, which presents unique characteristics such as a higher prevalence of Chagas disease. In Latin America in general, access to advanced diagnostic tools—such as gene expression profiling or donor-derived cell-free DNA—is often limited due to economic and structural constraints. In this context, hs-TnI may represent a promising and accessible biomarker to support the identification of patients at higher risk of rejection for whom prioritized EMB may be warranted, used in conjunction with other clinical and echocardiographic parameters.
We also explored whether the few biopsies with grade 3R rejection exhibited disproportionately higher hs-TnI levels; however, the number of 3R events was extremely small, preventing meaningful statistical analysis.
Limitations
This study presents some limitations. First, it is a single-center retrospective cohort, which may limit the generalizability of the results. The analysis was based on data extracted from electronic medical records, which are subject to potential recording bias and missing information. Additionally, although the total number of biopsies was considerable, the number of events with rejection >2R was relatively small, which may reduce the statistical power of the comparisons.
Conclusions
Our study described the potential of hs-TnI as a valuable biomarker for diagnosing ACR posttransplantation. Incorporating hs-TnI into posttransplant surveillance strategies may improve early rejection detection and patient outcomes, particularly in Latin American settings and other regions where access to advanced noninvasive diagnostic tools is limited. Moreover, this study highlights the utility of hs-TnI in patients with Chagas cardiomyopathy—a population often underrepresented in transplant literature. Further research and clinical trials are warranted to validate and optimize the use of hs-TnI in routine clinical practice, ultimately improving patient care and outcomes.
Disclosure statement
The authors declare no conflicts of interest.
Declaration of Generative AI and AI-assisted technologies in the writing process
During the preparation of this work, the author(s) used ChatGPT (OpenAI) to improve language and readability, with caution. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. We have nothing to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Caves P.K.Stinson E.B.Graham A.F.Billingham M.E.Grehl T.M.Shumway N.E.Percutaneous transvenous endomyocardial biopsy JAMA 22519732882914577226 · pubmed ↗
- 2Fitzsimons S.Evans J.Parameshwar J.Pettit S.J.Utility of troponin assays for exclusion of acute cellular rejection after heart transplantation: a systematic review J Heart Lung Transplant 3720186316382942671610.1016/j.healun.2017.12.008 · doi ↗ · pubmed ↗
- 3Baraldi-Junkins C.Levin H.R.Kasper E.K.Rayburn B.K.Herskowitz A.Baughman K.L.Complications of endomyocardial biopsy in heart transplant patients J Heart Lung Transplant 12199363678443204 · pubmed ↗
- 4Crespo-Leiro M.G.Zuckermann A.Bara C.Concordance among pathologists in the second cardiac allograft rejection gene expression observational study (CARGO II)Transplantation 942012117211772322273810.1097/TP.0b 013e 31826 e 19e 2 · doi ↗ · pubmed ↗
- 5Miller C.A.Fildes J.E.Ray S.G.Non-invasive approaches for the diagnosis of acute cardiac allograft rejection Heart 9920134454532325717210.1136/heartjnl-2012-302759 · doi ↗ · pubmed ↗
- 6Pham M.X.Teuteberg J.J.Kfoury A.G.Gene-expression profiling for rejection surveillance after cardiac transplantation N Engl J Med 3622010189019002041360210.1056/NEJ Moa 0912965 · doi ↗ · pubmed ↗
- 7Jeremias A.Gibson C.M.Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded Ann Intern Med 14220057867911586741110.7326/0003-4819-142-9-200505030-00015 · doi ↗ · pubmed ↗
- 8Liu Z.Perry L.A.Penny-Dimri J.C.Prognostic significance of elevated troponin in adult heart transplant recipients: a systematic review and meta-analysis Exp Clin Transplant 20202263364110.6002/ect.2021.038635037610 · doi ↗ · pubmed ↗