Diagnostic accuracy of reflectance confocal microscopy for acral lentiginous melanoma
Una Milovanovic, Adrianne Pan, Jennifer Laborada, Lucy Lam, Patrick Ottuso, Sairekha Ravichandran, Lilia Correa-Selm

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1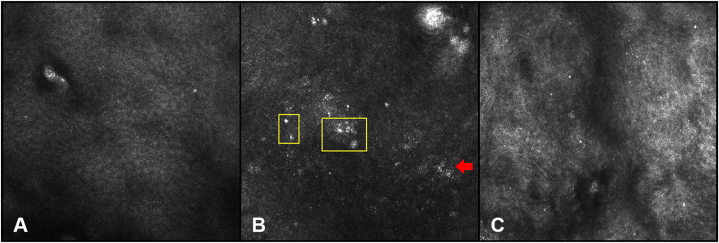 Figure 2
Figure 2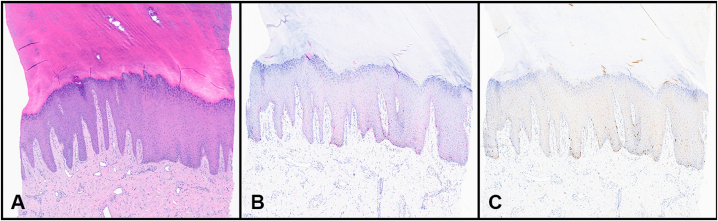 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Ocular Oncology and Treatments · Ocular and Laser Science Research
Clinical presentation
A 51-year-old Caucasian woman with a history of melanoma presented with a brown patch on the right heel. The patient described its onset 10 years ago and reported that the lesion had been changing in size and color in the recent years (Fig 1). Following an initial shave biopsy that was inconclusive, a punch biopsy was subsequently performed. The results suggested lentigo with negative staining for Preferentially Expressed Antigen in Melanoma. An independent dermatopathology review was obtained, which supported the initial findings. However, due to the small sample size, a repeat biopsy was recommended to achieve a more accurate representation of the larger lesion. Given the persistent diagnostic uncertainty and the lesion’s atypical and evolving characteristics, the patient was referred to for reflectance confocal microscopy (RCM) evaluation to have a better assessment of the lesion.Fig 1A 3.5 × 2.3 cm gray-brown macule with irregular borders is seen on the plantar aspect of the right heel.
Confocal microscopy appearance
RCM of the lesion was obtained using a VivaScope 1500 (Caliber Imaging and Diagnostics). The real-time, high-resolution imaging revealed focal collections of atypical melanocytes with bright, pleomorphic nuclei at the dermal–epidermal junction, findings consistent with melanoma (Fig 2).Fig 2A, Stratum spinosum of the epidermis showing a normal honeycomb pattern formed by keratinocytes. B, Nucleated melanocytes (yellow square) and multiple lymphocytes representing inflammation (red arrow). C, Upper dermis represented by collagen fibers.
Histological diagnosis
Following the concerning RCM findings, additional, broader biopsies were performed targeting areas of the lesion that showed atypia under RCM. Histopathologic examination of these samples confirmed the diagnosis of acral lentiginous melanoma (ALM) in situ (Fig 3).Fig 3A, Hematoxylin-eosin–stained tissue section from the right heel reveals increased numbers of single junctional melanocytes, some with nuclear atypia. B, SOX10 immunohistochemical stain with appropriate positive control highlights the distribution of melanocytes within the epidermis and highlights the variable nuclear size of the atypical melanocytes. C, PRAME immunohistochemical stain with appropriate positive control is strongly positive among the atypical junctional melanocytes. PRAME, Preferentially Expressed Antigen in Melanoma.
Key message
Histopathologic diagnosis of early-stage ALM remains challenging, as cytologic atypia is minimal and architectural disorder subtle.1 Evaluation is further complicated in large or clinically heterogeneous acral lesions, where difficulty in obtaining a representative tissue sample increases the risk of diagnostic delay.2 In this context, RCM provides a noninvasive, high-resolution imaging modality that enables real-time, near-histologic evaluation of the entire lesion, thereby improving detection of malignant transformation and optimizing biopsy site selection.
In this case, a patient with a rapidly evolving plantar macule underwent a punch biopsy with inconclusive results, followed by a shave biopsy consistent with lentigo. However, the clinical and dermoscopic features remained concerning for malignancy, prompting further evaluation with RCM. Imaging revealed a melanoma-characteristic pattern, guiding a single targeted rebiopsy that confirmed the diagnosis of ALM in situ. Absent confocal guidance, the next step in management would have required a broad incisional biopsy or multiple mapping biopsies. Both approaches have important limitations, including an association of the former with increased 5-year mortality in cutaneous melanoma and the inability of the latter to guarantee sampling of the most diagnostically relevant sites.3^,^4
Current studies support the value of RCM in identifying features of acral lesions that distinguish ALM from benign nevi, with a reported diagnostic accuracy of 90.3%, and show strong concordance with histopathology.5, 6, 7, 8 RCM likewise demonstrates high concordance with histopathology for presurgical margin mapping in lentigo maligna.9 Based on existing evidence and our experience, we recommend considering RCM as an adjunctive tool for precise biopsy site selection in diagnostically challenging acral lesions.
This case provided an opportunity to diagnose melanoma in a patient with high clinical suspicion despite nondiagnostic pathology, serving as an important reminder for dermatologists to continue pursuing their clinical judgment when discordant findings arise.
Conflicts of interest
Dr Lilia Correa-Selm reports consulting relationships with Accutec Blades, Enspectra Health, and Novartis. She has served as a researcher for Novartis, Pfizer, and Sanofi. She has also participated as a speaker for La Roche-Posay. All other authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fernandez-Flores A.Cassarino D.S.Histopathological diagnosis of acral lentiginous melanoma in early stages Ann Diagn Pathol 262017646910.1016/j.anndiagpath.2016.08.00527601330 · doi ↗ · pubmed ↗
- 2Kim T.H.Kim J.C.Kwon J.E.Kim Y.C.Choi J.W.Effect of changes in breslow thickness between the initial punch biopsy results and final pathology reports in acral lentiginous melanoma patients Sci Rep 11120211988510.1038/s 41598-021-99422-6PMC 849493934615974 · doi ↗ · pubmed ↗
- 3Swetter S.M.Tsao H.Bichakjian C.K.Guidelines of care for the management of primary cutaneous melanoma J Am Acad Dermatol 801201920825010.1016/j.jaad.2018.08.05530392755 · doi ↗ · pubmed ↗
- 4Liszewski W.Stewart J.R.Vidal N.Y.Demer A.M.Incisional biopsy technique is associated with decreased overall survival for cutaneous melanoma Dermatol Surg 485202248649110.1097/DSS.000000000000343035298451 · doi ↗ · pubmed ↗
- 5Zou Y.Li L.Xia R.Wang F.Accuracy of confocal microscopy for the diagnosis of acral lentiginous melanoma and acral melanocytic nevi Am J Dermatopathol 4710202576977410.1097/DAD.000000000000309940767501 · doi ↗ · pubmed ↗
- 6Chello C.Cappilli S.Pellegrino L.In vivo reflectance confocal microscopy applied to acral melanocytic lesions: a systematic review of the literature Diagnostics (Basel)14192024213410.3390/diagnostics 1419213439410538 PMC 11475194 · doi ↗ · pubmed ↗
- 7Zou Y.Zhu X.Xia R.Concordance between reflectance confocal microscopy and histopathology for the diagnosis of acral lentiginous melanoma Skin Res Technol 3012024 e 1357010.1111/srt.13570 PMC 1078188938200620 · doi ↗ · pubmed ↗
- 8Cinotti E.Debarbieux S.Perrot J.L.Reflectance confocal microscopy features of acral lentiginous melanoma: a comparative study with acral nevi J Eur Acad Dermatol Venereol 30720161125112810.1111/jdv.1339926428577 · doi ↗ · pubmed ↗