Locoregional Recurrence after Biochemical Incomplete Response in Differentiated Thyroid Cancer Patients: Insights into Influencing Clinicopathological Factors and the Potential Role of 18 F-FDG PET/CT
Mai Amr Elahmadawy, Ismail Mohamed Ali, Ibrahim Mansour Nasr, Omnia Talaat

TL;DR
This study explores factors influencing locoregional recurrence in thyroid cancer patients who don't fully respond to treatment, and finds that rising thyroglobulin levels and 18F-FDG PET/CT scans are strong indicators of recurrence.
Contribution
The study identifies thyroglobulin trends and 18F-FDG PET/CT as key tools for detecting locoregional recurrence in thyroid cancer patients with biochemical incomplete response.
Findings
Rising thyroglobulin levels strongly correlate with locoregional recurrence in thyroid cancer patients.
18F-FDG PET/CT demonstrated 100% sensitivity and specificity in detecting locoregional recurrence.
Papillary thyroid carcinoma and T2/T3 tumor stages are associated with higher recurrence rates.
Abstract
The aim of this study was to evaluate the clinicopathological factors and stimulated thyroglobulin (Tg) course related to the occurrence of locoregional recurrence (LRR) in differentiated thyroid cancer (DTC) patients with biochemical incomplete response (BIR) as well as the value of fluorine-18 fluorodeoxyglucose ( 18 F-FDG) positron emission tomography (PET)/computed tomography (CT) in these patients. A total of 253 DTC adult patients initially treated with total thyroidectomy and iodine-131 (RAI-131) ablation and showed BIR on follow-up were enrolled in the study. All clinical, laboratory, pathological, radiological, and follow-up data were retrieved from their records. Seventy-three out of the 253 BIR patients developed LRR during follow-up with the median time to recurrence of 27 months. In all, 61.6% of those who developed LRR were females, 78.1% were papillary thyroid…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
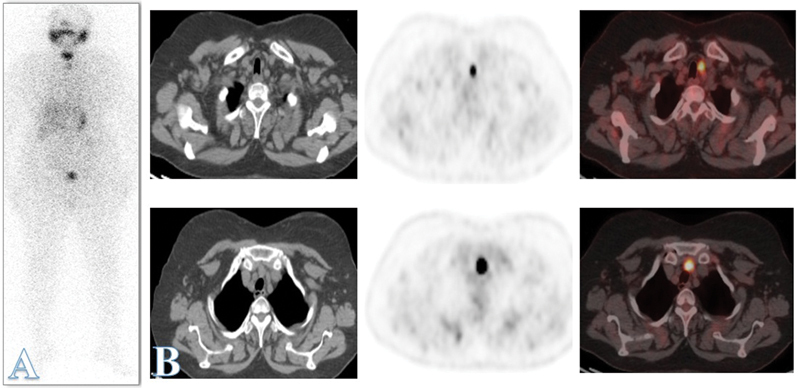 Fig. 1
Fig. 1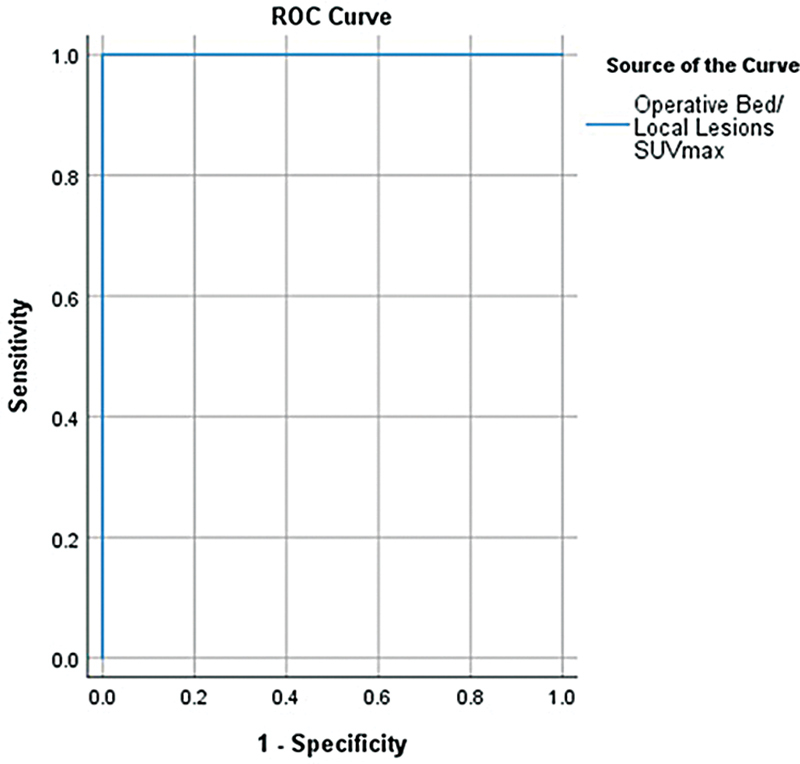 Fig. 2
Fig. 2| Locoregional recurrence | ||||||
|---|---|---|---|---|---|---|
| Positive | Negative | |||||
| Number | % | Number | % | |||
| Age | ≥45 y | 33 | 45.2 | 75 | 41.7 | 0.606 |
| < 45 y | 40 | 54.8 | 105 | 58.3 | ||
| Sex | Female | 45 | 61.6 | 139 | 77.2 | 0.012 |
| Male | 28 | 38.4 | 41 | 22.8 | ||
| Pathology | PTC | 57 | 78.1 | 159 | 88.3 | 0.001 |
| FTC | 8 | 11.0 | 20 | 11.1 | ||
| Hürthle cell | 8 | 11.0 | 1 | 0.6 | ||
| Capsular Invasion | Positive | 22 | 30.1 | 35 | 19.4 | 0.065 |
| Negative | 51 | 69.9 | 145 | 80.6 | ||
| Vascular invasion | Positive | 7 | 9.6 | 14 | 7.8 | 0.636 |
| Negative | 66 | 90.4 | 166 | 92.2 | ||
| Lymph nodes metastases | Positive | 26 | 35.6 | 42 | 23.3 | 0.046 |
| Negative | 47 | 64.4 | 138 | 76.7 | ||
| T | T1a | 3 | 4.1 | 28 | 15.6 | < 0.001 |
| T1b | 13 | 17.8 | 71 | 39.4 | ||
| T2 | 38 | 52.1 | 50 | 27.8 | ||
| T3a | 1 | 1.4 | 6 | 3.3 | ||
| T3b | 18 | 24.7 | 25 | 13.9 | ||
| N | Positive | 26 | 35.6 | 42 | 23.3 | 0.046 |
| Negative | 47 | 64.4 | 138 | 76.7 | ||
| M | Positive | 0 | 0.0 | 0 | 0.0 | – |
| Negative | 73 | 100.0 | 180 | 100.0 | ||
| Initial treatment | Thyroidectomy + RAI-131 ablation | 61 | 83.6 | 142 | 78.9 | 0.398 |
| Thyroidectomy + nodal dissection + RAI-131 ablation | 12 | 16.4 | 38 | 21.1 | ||
|
|
|
| ||
|
|
|
| ||
|
| ||||
| ≥45 y | 1 (50.0%) | 38 (55.9%) | 69 (37.7%) | 0.017 |
| < 45 y | 1 (50.0%) | 30 (44.1%) | 114 (62.3%) | |
|
| ||||
| Female | 2 (100.0%) | 42 (61.8%) | 140 (76.5%) | 0.043 |
| Male | 0 (0.0%) | 26 (38.2%) | 43 (23.5%) | |
|
| ||||
| PTC | 1 (50.0%) | 53 (77.9%) | 162 (88.5%) | < 0.001 |
| FTC | 1 (50.0%) | 7 (10.3%) | 20 (10.9%) | |
| Hürthle cell | 0 (0.0%) | 8 (11.8%) | 1 (0.55%) | |
|
| ||||
| Positive | 1 (50.0%) | 19 (27.9%) | 37 (20.2%) | 0.185 |
| Negative | 1 (50.0%) | 49 (72.0%) | 146 (79.8%) | |
|
| ||||
| Positive | 0 (0.0%) | 7 (10.3%) | 14 (7.7%) | 0.670 |
| Negative | 2 (100.0%) | 61 (89.7%) | 169 (92.3%) | |
|
| ||||
| T1a | 0 (0.0%) | 4(5.8%) | 27 (14.8%) | 0.005 |
| T1b | 1 (50.0%) | 14 (20.6%) | 69 (37.7%) | |
| T2 | 0 (0.0%) | 34 (50.0%) | 54 (29.5%) | |
| T3a | 0 (0.0%) | 1 (1.5%) | 6 (3.2%) | |
| T3b | 1 (50.0%) | 15 (22.1%) | 27 (14.8%) | |
|
| ||||
| N0 | 1 (50.0%) | 45 (24.3%) | 139 (76.0%) | 0.173 |
| N1 | 1 (50.0%) | 23 (33.8%) | 44 (24.0%) | |
|
| ||||
| Thyroidectomy + RAI-131 ablation | 1 (50.0%) | 57 (28.1%) | 145 (79.2%) | 0.289 |
| Thyroidectomy + nodal dissection + RAI-131 ablation | 1 (50.0%) | 11 (22.0%) | 38 (20.8%) | |
|
| ||||
| Positive | 0 (0.0%) | 59 (80.8%) | 14 (7.7%) | < 0.001 |
| Negative | 2 (100.0%) | 9 (5.0%) | 169 (92.3%) | |
|
| ||||
| ≤23 mo | 0 (0.0%) | 33 (55.9%) | 4 (28.6%) | 0.150 |
| > 23 mo | 0 (0.0%) | 26 (44.1%) | 10 (71.4%) | |
|
| ||||
| Complete response | 2 (100.0%) | 48 (70.6%) | 183 (100.0%) | < 0.001 |
| Incomplete response | 0 (0.0%) | 20 (29.4%) | 0 (0.0%) | |
|
| ||||
| Alive | 2 (100.0%) | 60 (88.2%) | 178 (97.3%) | 0.019 |
| Dead | 0 (0.0%) | 8 (11.8%) | 5 (2.7%) | |
| Outcome | 6 months Post-ablation Tg | |||||
|---|---|---|---|---|---|---|
| ≤ 17 | > 17 | |||||
| Number | % | Number | % | |||
| Loco-regional recurrence | Positive | 35 | 27.1 | 38 | 30.6 | 0.633 |
| Negative | 94 | 72.9 | 86 | 69.4 | ||
| Complete/incomplete response | Complete | 120 | 93.0 | 113 | 91.1 | 0.577 |
| Incomplete | 9 | 7.0 | 11 | 8.9 | ||
| Time to recurrence (mo) | ≤23 | 18 | 48.6 | 20 | 51.3 | 0.818 |
| > 23 | 19 | 51.4 | 19 | 48.7 | ||
| Survival | Alive | 124 | 96.1 | 116 | 93.5 | 0.354 |
| Died | 5 | 3.9 | 8 | 6.5 | ||
| Distant metastases | Positive | 2 | 1.6 | 5 | 4.0 | 0.274 |
| Negative | 127 | 98.4 | 119 | 96.0 | ||
| Outcome | 1-year follow-up Tg | |||||
|---|---|---|---|---|---|---|
| ≤5.7 | > 5.7 | |||||
| Number | % | Number | % | |||
| Locoregional recurrence | Positive | 11 | 8.7 | 62 | 49.2 | < 0.001 |
| Negative | 116 | 91.3 | 64 | 50.8 | ||
| Complete/incomplete response | Complete | 127 | 100.0 | 106 | 84.1 | < 0.001 |
| Incomplete | 0 | 0.0 | 20 | 15.9 | ||
| Time to recurrence (mo) | ≤23 | 6 | 46.2 | 32 | 50.8 | 0.761 |
| > 23 | 7 | 53.8 | 31 | 49.2 | ||
| Survival | Alive | 124 | 97.6 | 116 | 92.1 | 0.045 |
| Died | 3 | 2.4 | 10 | 7.9 | ||
| Distant metastases | Positive | 4 | 3.1 | 3 | 2.4 | 1 |
| Negative | 123 | 96.9 | 123 | 97.6 | ||
| Performance | PET/CT | Neck U/S | RAI-131 |
|---|---|---|---|
| Sensitivity | 100.00% | 92.86% | 85.71% |
| Specificity | 99.16% | 99.58% | 100.00% |
| PPV | 87.50% | 92.86% | 100.00% |
| NPV | 100.00% | 99.58% | 99.17% |
| Accuracy | 99.21% | 99.21% | 99.21% |
| Lymph nodes level | Number of lymph nodes detected | |
|---|---|---|
| 18 F-FDG PET/CT | US | |
| Level I | 6 | 5 |
| Level II | 25 | 22 |
| Level III | 19 | 14 |
| Level IV | 32 | 25 |
| Level V | 10 | 6 |
| Level VI | 51 | 35 |
| Supraclavicular LNs | 8 | 4 |
| Total number of lymph nodes | 151 | 111 |
| End point | SUVmax | ||||||
|---|---|---|---|---|---|---|---|
| AUC | 95% confidence interval | Cutoff | Sensitivity (%) | Specificity (%) | |||
| Lower bound | Upper bound | ||||||
| Local recurrence | 1.000 | < 0.001 | 1.000 | 1.000 | 3.65 | 100 | 100 |
| Response | 0.545 | 0.787 | 0.216 | 0.875 | – | – | – |
| Time to recurrence | 0.520 | 0.901 | 0.199 | 0.841 | – | – | – |
| Survival | 0.417 | 0.696 | -0.001- | 0.834 | – | – | – |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Radiomics and Machine Learning in Medical Imaging · Radiation Dose and Imaging
Introduction
The management of differentiated thyroid cancer (DTC) has undergone significant changes over the past decades, driven by large-scale biological studies, improved diagnostic tools, and therapeutic advances. 1
Initial risk stratification constitutes a starting point that guides initial management and follow-up but represents a static picture that does not consider response to initial treatment. 2 Hence, Tuttle and Alzahrani proposed the dynamic risk assessment (DRA) based on new integrated data that become available during the initial follow-up. 3 Such a strategy has been well received and has been adopted by several societies. 4 5 6
The DRA approach involves restratification of the initial risk assessment of DTC patients taking into account different responses to treatment: excellent, indeterminate, biochemical incomplete response (BIR), and structural incomplete response (SIR). This is done using data obtained during follow-up: thyroglobulin (Tg) and anti-Tg values, imaging techniques, including neck ultrasound (US), radioactive iodine-131 (RAI-131) whole-body scans, computed tomography (CT), and fluorine-18 fluorodeoxyglucose positron emission tomography CT ( ^18^ F-FDG PET/CT). 2
BIR is not an uncommon event after initial treatment with reported prevalence varying from 11 to 22%. BIR encompasses persistent elevated Tg values or anti-Tg antibodies (TgAb) without evidence of structural disease. 7 The incidence of developing structural recurrence varies across published data and the outcomes of such patients remain quite heterogeneous. A comprehensive data analysis of the factors linked to clinical outcome in this scenario is not adequately addressed. 8
^18^ F-FDG PET/CT scan has an established role in the detection of local and distant recurrence in DTC patients, especially when the Tg level is elevated and other imaging modalities are negative. 9 Also, the magnitude of the metabolic activity may reflect disease aggressiveness, and thus can provide information about the long-term outcome. 10 Therefore, the findings provided by ^18^ F-FDG PET/CT might modify the therapeutic approach in up to 30% of patients. 11 The present study aims at assessing the relation of various clinicopathological factors with the occurrence of locoregional recurrence in DTC patients with BIR, the role of posttreatment stimulated Tg in the dynamic assessment of such patients, and the performance of ^18^ F-FDG PET/CT in the detection and prediction of outcome of structural recurrence versus standard techniques.
Patients and Methods
Study Population
In total, 2,000 files for DTC patients who have received radioactive iodine therapy at the Nuclear Medicine Unit, National Cancer Institute (NCI), Cairo University, were reviewed in the period from 2000 to 2021. A total of 253 DTC adult patients who were initially treated with total thyroidectomy and RAI-131 ablation and showed BIR on follow-up were enrolled in the study. All demographic, clinical, laboratory, pathological, radiological, and follow-up data were retrieved from their records. All methods were performed in accordance with relevant guidelines and regulations. The study was approved by the Ethical Committee at NCI, with Institutional Review Board (IRB) number RO2311–309–062. Informed consent was waived due to the retrospective nature of the study and the analysis used anonymized clinical data.
The patients were stratified using the eighth edition of the American Joint Committee on Cancer/International Union against Cancer (AJCC/UICC) staging system. 12 Fixed doses of RAI-131 ablation were given (range: 30–100 mCi). The response assessment was evaluated at 6 and 12 months after RAI-131 therapy and at last follow-up. The follow-up included serum Tg assessment, neck US, and RAI whole-body scan. Neck US was performed by an experienced radiologist, and RAI-131 whole-body scan was performed 4 to 7 days after therapeutic RAI-131 and 2 days after diagnostic RAI-131 and was interpreted by an experienced nuclear physician. ^18^ F-FDG PET/CT was used during follow-up to detect structural recurrent disease in patients who showed BIR.
Therapy response was categorized according to the American Thyroid Association (ATA) management guidelines into excellent response (ER), indeterminate response (IR), BIR, and SIR. The patients were divided into a complete response group and an incomplete response group (including patients showing IR, BIR, or SIR) according to the response to therapy for the purpose of predictive correlations with response to therapy. 13
Locoregional structural recurrence was defined as tumor in the operative bed or regional lymph nodes detected by RAI-131, US, and/or ^18^ F-FDG PET/CT and proven histologically, after a documented tumor-free period.
Imaging Techniques and Diagnostic Procedures
RAI-131 Therapy
One to 2 weeks prior to the 131-I therapy, the patient begins a low-iodine diet. Radioiodine therapy was given after T4 withdrawal for approximately 4 weeks to ensure the thyroid-stimulating hormone (TSH) level was greater than 30 mU/L, which was measured at therapy day in association with measuring the serum Tg level. Patients were hospitalized for 3 to 5 days according to the therapy dose given. T4 treatment was resumed on the fourth day with a posttherapy whole-body scan performed 5 to 7 days after oral intake of I-131.
In between therapy doses, patients were maintained on thyroxine suppressive therapy to keep the TSH level around 0.01 mU/L.
Serum Thyroglobulin Measurement
Serum Tg was assessed in our institute's laboratory using one commercial immunometric assay, and the same assay was used throughout a patient's follow-up. Stimulated Tg (TSH ≥30 mU/L after thyroid hormone withdrawal) was evaluated in the current study.
Neck Ultrasound
Neck US was performed in all patients by experienced sonographers using high-resolution US linear array transducer (7–15 MHz). The patients were placed in the supine position with the neck hyperextended. Any suspicious operative bed lesions or regional lymph nodes (>10 mm) were reported with their characteristics including site and size.
18
F-FDG PET/CT Protocol and Interpretation
^18^ F-FDG PET/CT study was performed using a Discovery PET/CT scanner (GE Medical System, Milwaukee, WI, United States). The study protocol was performed in accordance with the European Association of Nuclear Medicine (EANM) procedure guidelines for tumor imaging, version 2.0. 14 Images were reconstructed according to our departmental protocol.
^18^ F-FDG PET/CT images were reviewed and analyzed on the manufacturer's GE review station, which provided multiplanar reformatted images and enabled the display of the PET images, CT images, and fused PET/CT images. The images were interpreted by an experienced nuclear medicine physician.
Positive scan findings were considered when abnormal/nonphysiological focal FDG uptake was noted at PET images above the background activity. The spherical volume of interest (VOI) was drawn over the regions of interest (operative bed or regional nodal metastases) and the maximum standardized uptake value (SUVmax) was recorded. The whole-body images were also evaluated for distant sites of metastases.
Statistical Analysis
Data were coded and entered using the Statistical Package for the Social Sciences (SPSS) version 28 (IBM Corp., Armonk, NY, United States). Data were summarized using mean, standard deviation, median, minimum and maximum in quantitative data, and frequency (count) and relative frequency (percentage) for categorical data. Comparisons between quantitative variables were done using the nonparametric Kruskal–Wallis and Mann–Whitney tests. 15 For comparing categorical data, the chi-squared ( χ ^2^ ) test was performed. The exact test was used instead when the expected frequency was less than 5. 16 Standard diagnostic indices including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic efficacy were calculated as described by Galen. 17 The receiver operating characteristic (ROC) curve was constructed with area under curve analysis performed to detect the best cutoff value of Tg and SUV for the detection of different outcomes. A p -value less than 0.05 was considered statistically significant.
Results
Biochemical Incomplete Response
This study enrolled 253 DTC patients treated with surgery and RAI-131 ablation and showed BIR. Females comprised 184 (72.7%) patients in the study group and 69 (27.3%) were males, with the female-to-male ratio of 2.7:1.
Their median age was 43 (range: 19–82) years. In all, 108 patients (42.7%) were ≥45 years. Papillary thyroid carcinoma (PTC) was the predominant pathology, representing 85.4% of the group, followed by follicular thyroid carcinoma (FTC) at 11.1%, and the Hürthle cell at 3.6%. The median size of the primary tumor was 2.4 cm (range, 0.8–9 cm). The initial staging was T1 in 115 (45.45%) patients, T2 in 88 (34.78%) patients, and T3 in 50 (19.76%) patients. In all, 68 (26.9%) patients were classified as N1, and all of them were M0. The capsular invasion was positive in 57 patients (22.5%). The vascular invasion was positive in 21 (8.3%) patients.
Initial management of the enrolled group was surgery, followed by RAI-131 ablation. Surgery was total thyroidectomy in 203 patients (80.2% of the group) and was total thyroidectomy with lymphadenectomy in the remaining 50 patients (19.8% of the group). After initial radio-surgical management, all patients started thyroxine suppressive therapy. All the patients revealed complete structural response with no radiologically detectable gross residual tumor, but an incomplete biochemical response, where the median value of the Tg level—while off Eltroxin—was 17 (range: 10–93) 6 months postablation. An additional 1-year follow-up revealed a gradual rise of Tg in 96 patients (37.9%) of the group; 148 (58.5%) patients had declining levels and 9 (3.6%) had stable Tg levels.
The median follow-up period was 76 months (range, 13–123 months). During follow-up, 73 patients developed locoregional recurrence and 7 (2.8%) patients developed distant metastases, 2 in the bone, 4 in the lung, and 1 in the brain. Thirteen patients (5.1%) died during follow-up.
Locoregional Structural Recurrence after BIR
In an attempt to investigate patients at higher risk of locoregional recurrence after BIR. Retrospective analyses were performed of those patients who developed pathologically proven locoregional recurrence compared with those who remained free of recurrent disease at the end of the study, to evaluate pretreatment clinicopathological factors that are associated with and perhaps predispose to the occurrence of locoregional recurrence in such patients ( Fig. 1 ).
A 60-year-old female patient with papillary thyroid carcinoma underwent total thyroidectomy and received 100 mCi of RAI-131 for ablation followed by thyroxine suppressive therapy. At 6 months of follow-up, her stimulated thyroglobulin (Tg) level was 13 ng/mL with no evidence of any structural disease residue/recurrence on diagnostic RAI-131 whole-body scan or neck ultrasound (US) or computed tomography (CT) chest. ( A ) On further 3 months of follow-up, the stimulated Tg level showed further elevation to 27 ng/mL; thus, RAI-131 therapy was recommended, and posttherapy scan revealed Iodine uptake at thyroid operative bed and a smaller less active focal lesion is seen at the upper chest region likely nodal lesion. Neck ultrasound (US) revealed operative bed scarring and left paratracheal hypoechoic nodule (1 × 0.6 cm) likely nodal. Fluorine-18 fluorodeoxyglucose ( 18 F-FDG) positron emission tomography (PET)/computed tomography (CT) was performed, which revealed a clear operative bed and FDG avid pre-tracheal and left paratracheal lymph nodes. The largest measured 1.3 × 1.6 cm, with the maximum standardized uptake value (SUVmax) of ∼16.8. ( B ) Pathology revealed metastatic papillary carcinoma.
Female patients represented 61.6% of those patients who developed locoregional recurrence ( p = 0.012). Fifty-seven of the 73 patients who developed recurrence had PTC, representing 78.1% of the population compared with other pathologies ( p = 0.001). In all, 35.6% of the patients who experienced locoregional recurrence had initial regional nodal deposits compared with 23.3% of the other group ( p = 0.046). For patients with locoregional recurrence, the primary tumors were T2 in 52.1% of them, T3 in 26.1%, and T1 in 21.9%, while in 55% of the patients who were negative for locoregional recurrence, the primary tumors were classified as T1 at initial staging, 27.8% as T2, and 17.2% as T3 ( p < 0.001).
No significant association was noted between the initial management, whether it included nodal dissection or not, and the incidence of recurrence ( p = 0.398). No significant age prevalence was noted among both groups ( p = 0.606). Vascular invasion did not reveal any significant association in both groups ( p = 0.636). Although no statistically significant association was found, a trend for prevalence of capsular invasion was observed among patients who developed locoregional recurrence, representing 30.1% compared with 19.4% of those who did not develop recurrence ( p = 0.065; Table 1 ).
Thyroglobulin Course and Structural Locoregional Recurrence
At the first 6 months of follow-up after RAI-131 ablation, the entire group showed an incomplete biochemical response as the median value for Tg was 17 (range, 10–93) ng/mL, and on further 1-year follow-up, the median value of Tg level for the entire group was 5.7 (range, 0.2–220) ng/mL.
The median value of Tg level for the group who later on developed locoregional recurrence compared with those who remained free at the last follow-up was 18 (range, 13–93) versus 17 (range, 10–90) ng/mL. On further 1-year follow-up, the median value spontaneously increased for the positive group to 37.6 (range, 15–220) ng/mL and decreased for those who remained free to 3 (range, 0.2 - 58) ng/mL.
The median time to recurrence was 27 months. The median size of the operative bed lesions was 2.2 (range, 1–5) cm, the median value of their SUVmax was 7.4 (range, 3.5–15.2). The median size of the regional lymph nodes was 1.7 (range, 0.8–8.8) cm, and the median value of their SUVmax was 8.1 (range, 2.9–19.4).
By evaluating the course of the Tg level over a 1-year follow-up in relation to various clinicopathological parameters, 78.6% of the patients aged less than 45 years showed declining Tg levels compared with 63.9% of those ≥45 years ( p = 0.017). In all, 37.7% of males revealed progressive elevation of the Tg level compared with 22.8% of females ( p = 0.043). In total, 88.9% of patients with Hürthle cell tumors had rising Tg levels compared with 24.5 and 25.0% of those with PTC and FTC, respectively ( p < 0.001). Among patients who showed a progressive Tg course, 73.6% were classified as T2 and T3, while 52% of those with a declining course were classified as T1 ( p = 0.005). Eighty percent of the patients with a rising Tg level developed structural locoregional recurrence compared with 7.7% of those with a declining course ( p < 0.001). One-hundred percent of those with declining and stable Tg levels showed complete response to therapy compared with 70.6% of those with a rising Tg level ( p < 0.001). Among patients with a rising Tg level, 11.8% died on follow-up compared with 2.7 and 0% of patients with a declining and stable course ( p = 0.019). No significant correlation was observed between capsular invasion, vascular invasion, N-stage, primary treatment, and time to recurrence in respect to the course of Tg ( Table 2 ).
As a trial to investigate the impact of 6 months of postablation Tg and 1-year follow-up Tg levels on disease outcome, the ROC curve was first tested to mark the cutoff point with compromised sensitivity and specificity for postablation Tg (6 months) and 1-year follow-up Tg, to discriminate positive versus negative locoregional recurrence; however, such cutoff points could not be obtained ( p > 0.05). Thus, their median values have been used instead as cutoffs and for correlations in respect to different clinicopathological parameters. The 6-month postablation Tg did not reveal any significant correlations with the occurrence of locoregional recurrence, treatment response, time to recurrence, survival, or occurrence of distant metastases ( Table 3 ). Meanwhile assessing the median value of the 1-year follow-up stimulated Tg revealed significant correlations with the occurrence of locoregional recurrence. Among those who remained recurrence free, 91.3% had a Tg level lower than 5.7 ng/mL compared to only 8.7% who developed locoregional recurrence ( p < 0.001). One-hundred percent of those with Tg ≤ 5.7 ng/mL showed complete therapy response compared with 84.1% of those with Tg > 5.7 ng/mL ( p < 0.001). Ten out of the 13 patients who died on follow-up had T9 > 5.7 ng/mL ( p = 0.045). No significant correlations were obtained in relation to time to recurrence or the occurrence of distant metastases ( p = 0.761 and 1) respectively ( Table 4 ).
18
F-FDG PET/CT versus Other Standard Techniques Modalities on Diagnostic and Prognostic Basis
With regard to the diagnostic performance of ^18^ F-FDG PET/CT in the detection of structural locoregional recurrence in comparison to other standard techniques, ^18^ F-FDG PET/CT revealed the highest sensitivity and NPV of 100% compared to sensitivity of 92.86 and 85.71% and NPV of 99.58 and 99.17%, respectively, with US and RAI-131 scan. Meanwhile, the highest specificity and PPV (100%) were observed with RAI-131 compared to specificity values of 99.16 and 99.58% and PPV of 87.50 and 92.86%, respectively, with ^18^ F-FDG PET/CT and US ( Table 5 ).
Table 5: Diagnostic performance of 18 F-FDG PET/CT versus US versus RAI-131 in detection of structural locoregional recurrence in DTC patients
On per nodal analysis, a higher number of lymph nodes were detected by ^18^ F-FDG PET/CT compared with US at different levels where ^18^ F-FDG PET/CT exceeded the US in the total number of nodes detected by 40 lymph nodes. The highest difference was at level VI, followed by level IV, and the least difference was at level I ( Table 6 ).
Table 6: Number of lymph nodes detected by 18 F-FDG PET/CT versus neck US at different levels
Predictive Value of
18 F-FDG PET/CT
The ROC curve was tested to mark the cutoff point for SUVmax with compromised sensitivity and specificity to discriminate patients with positive versus negative structural local recurrence, complete response versus incomplete response, long versus short time to recurrence (using the median value as a cutoff), and survival (alive versus dead). A cutoff point (SUVmax = 3.65) was successfully marked to discriminate positive versus negative local recurrence with sensitivity and specificity of 100% and p -value less than 0.001. Other cutoff points, in respect to response, time to recurrence, and survival, could not be obtained ( p > 0.05; Fig. 2 ; Table 7 ).
Receiver operating characteristic (ROC) curve to test the maximum standardized uptake value (SUVmax) capability to differentiate differentiated thyroid cancer patients who were positive versus negative for structural local recurrence ( p < 0.001).
Discussion
BIR in DTC is one of the most challenging events that may occur post radio-surgical treatment with still unclear predisposing factors and concerns about its outcomes. 7 Since Tg level is a cornerstone parameter in follow-up of treated DTC for early detection of structural recurrence, its failure to decline to undetectable level postthyroidectomy and RAI-131 ablation makes the follow-up problematic. This raises concerns for microscopic disease that remains beyond radiological detectability. 18 In clinical practice, BIR does not seem to be restricted to only patients initially classified as high risk; hence, few studies attempted to explore specific risk factors that may be linked to BIR. Lim et al aimed at constructing a nomogram to determine the predictors of BIR. 19 Their multivariate analysis demonstrated that age ≥55 years, male sex, site of lymph node metastasis, presence of extrathyroidal extension, and presence of lymphovascular invasion were significantly associated with BIR. In our group, 72.7% of patients who experienced BIR were females, 42.7% were ≥45 years, and 26.9% were classified as N1. Capsular invasion was positive in 22.5% and vascular invasion was positive in only 8.3% patients. PTC was found in 85.4% of the group, the median size of the primary tumor was 2.4 cm, 45.45% patients were classified as T1, and all were M0.
One of the major prognostic concerns is whether BIR predisposes to higher incidence of recurrence; thus, such patients are usually exposed to unnecessary excessive management. 8 In published literature, only few studies investigated the poor prognostic factors in DTC patients with BIR with a relatively small number of enrolled patients. The number of patients who developed structural recurrent disease was also low. 20 21 22 23 24 In the current study, 253 patients with BIR were enrolled, among which 73 patients (28.85%) developed structural locoregional recurrence with a median time to recurrence of 27 months. Previous studies have reported that 5 to 27% of patients with DTCs develop locoregional recurrences. 25 Such recurrences have been reported to be located in cervical lymph nodes in 60 to 75% of cases and thyroid bed in approximately 20% of cases, worsening the prognosis and leading to a risk of cancer-related death. 25 A slightly higher incidence is noted among our group due to the already present posttreatment elevated Tg level as a risk factor. In another study performed by Ahn et al, they evaluated the long-term outcomes of 102 patients with PTC showing a BIR during the first 12 to 24 months following initial therapy. Structural persistent disease was observed in 43 (42%) patients. 24
An attempt was performed in the present study to further explore those patients at higher risk of structural locoregional recurrence after BIR. Our enrolled population revealed a predominance for female patients (61.6%) among those who developed structural locoregional recurrence; however, the higher incidence of DTC among females and the high number of the female patients already enrolled within the study population can stand behind such predominance. PTC is known for being the most familiar type of thyroid carcinoma, accounting for nearly 90% of all thyroid carcinomas with early dissemination to regional lymph nodes where the postoperative serum Tg is one of its prognostic indicators. 26 In the present study, PTC represented 78.1% of those who developed locoregional recurrence compared with other pathologies ( p = 0.001). A higher number (35.6%) of such patients also had initial regional nodal deposits compared with 23.3% of those who remained free from locoregional recurrence till the last follow-up ( p = 0.046). For patients developed locoregional recurrence; their primary tumors were of higher T stages compared with those who were negative for locoregional recurrence ( p < 0.001). However, age, vascular invasion, and initial management did not reveal a significant association ( p > 0.05). A trend for the prevalence of capsular invasion was observed among patients who developed locoregional recurrence, representing 30.1% compared with 19.4% of those who did not develop recurrence ( p = 0.065).
Current trends in clinical practice adopted DRA in DTC; thus, not only the post–radio-surgical ablation level of Tg matters but also its course overtime should be considered the key parameters for dynamic risk stratification in DTC. 2 At the first 6 months of follow-up after RAI-131 ablation, the entire study group showed an incomplete biochemical response; the median value for stimulated Tg was 17 (range, 10–93), and on further 1-year follow-up, the median value of stimulated Tg level for the entire group was 5.7 (range, 0.2–220). At the initial 6 months of follow-up, no significant difference in respect to the median value of the Tg level for the group who later on developed locoregional recurrence compared with those who remained free at the last follow-up was observed (18 vs. 17, respectively). However, a gap between both groups appeared on further 1-year follow-up, where the median value spontaneously increased for the positive group to 37.6 and decreased for those who remained free to 3. Also, the majority (80%) of the patients with rising Tg level developed structural locoregional recurrence compared with only 7.7% of those with a declining course ( p <0.001). Such results matched those of Wang et al, who concluded that the incremental course of posttreatment Tg is a significant predictor for structural recurrent/persistent disease with high PPV of 81% when it exceeds 20.2 ng/mL, which provides a prompt identification of those at higher risk and paves the way to enable subsequent intensive management and follow-up. 7 Also, several studies revealed a strong association between rising TG level and recurrence in DTC. 27 28 29
By evaluating the course of the posttreatment stimulated Tg level over a 1-year follow-up in relation to various clinicopathological parameters, older age (≥45 years), male sex, Hürthle cell tumors, and T2 and T3 primary tumors revealed progressive elevation of the Tg level compared with other parameters ( p < 0.05). A higher number (29.4%) of patients showed a rising Tg course had incomplete therapy response at last follow-up, while all patients with a declining and stable Tg level showed complete response ( p < 0.001) and 11.8% of them with a rising Tg died on follow-up compared with 2.7 and 0% of a declining and stable course ( p = 0.019). But no significant correlation between capsular invasion, vascular invasion, N-stage, primary treatment, and time to recurrence in respect to the course of Tg was observed.
In respect to the median Tg value at the initial 6-month versus 1-year follow-up, the former did not significantly correlate with risk of locoregional recurrence or any different clinicopathological factors. On the contrary, longer follow-up at the 1-year median Tg value revealed significant correlations between locoregional recurrence, therapy response, and mortality ( p <0.05). No significant correlations were also obtained with time to recurrence or the occurrence of distant metastases ( p = 0.761 and 1, respectively).
As previously mentioned, the main seriousness of BIR stands behind the risk of developing structural disease that is detected by morphological imaging and calling for a strategic therapeutic approach. 23 Standard diagnostic imaging techniques in DTC are neck US, CT, magnetic resonance imaging (MRI), and nuclear imaging, such as postdiagnostic or therapeutic radioiodine whole-body scan and/or ^18^ F-FDG PET/CT. 30 31 US is cost-effective and accessible for detecting cervical recurrence, but it is not without limitations such as false-positive results. 32 RAI imaging is crucial for RAI-avid disease but is ineffective in RAI-refractory cases. ^18^ F-FDG PET/CT is cost-effective and indispensable in high-risk or RAI-refractory disease but is limited by its high cost and availability. 33 Therefore, a more widely adopted stepwise approach, using US and RAI 131 as first-line tools, and reserving ^18^ F-FDG PET/CT for high-risk or complex cases, offers an optimal balance between cost-effectiveness and accessibility in clinical practice.
The role of ^18^ F-FDG PET/CT in DTC has been specifically highlighted in the cases with rising Tg and negative radioactive iodine WBS. Meanwhile, ^18^ F-FDG PET/CT is not only a noninvasive whole-body screening tool but also may reflect disease aggressiveness and provide information about the long-term outcome, which might influence and even modify the therapeutic approach in some patients. 31 There were controversial data about the impact of TSH stimulation on the accuracy of ^18^ F-FDG PET/CT, with the clinical benefit not clearly identified. 34 With regard to Tg, although there is no consensus on the cutoff value that provides the optimum diagnostic accuracy of ^18^ F-FDG PET/CT to detect local and/or distant disease recurrence, the ATA guidelines recommend that a stimulated Tg level greater 10 ng/mL should be an adequate indicator. 35 In the current study, the diagnostic performance of ^18^ F-FDG PET/CT in the detection of structural locoregional recurrence was 100, 99.16, and 87.50% in terms of sensitivity, specificity, and PPV, respectively. Abelleira et al 36 reported a sensitivity of 95% and a specificity of 87.5%, while Lu et al 37 reported a sensitivity and PPV of 93.30 and 91.40%, respectively. In respect to other standard techniques, the highest sensitivity and NPV of 100% were obtained by ^18^ F-FDG PET/CT compared to sensitivity values of 92.86 and 85.71% and NPV of 99.58 and 99.17%, respectively, with US and RAI-131 scan, while the highest specificity and PPV (100%) were observed with RAI-131 compared to specificity values of 99.16 and 99.58% and PPV of 87.50 and 92.86%, respectively, with ^18^ F-FDG PET/CT and US. The median size of the operative bed lesions was 2.2 cm, the median value of their SUVmax was 7.4, the median size of the regional lymph nodes was 1.7, and the median value of their SUVmax was 8.1. A higher number of regional lymph nodes were detected by ^18^ F-FDG PET/CT compared to US and was specially noted at level VI, followed by level IV, and the least difference was at level I.
Quantitation is one of the main advantages of PET/CT. A predefined SUVmax cutoff value can help in differentiating malignant lesions from benign ones, improving diagnostic accuracy. High SUVmax lesions might indicate a more aggressive phenotype and may predict RAI refractory disease, guiding a shift toward alternative therapies. 38 However, there is still lack of standardization of the SUVmax cutoffs with potential limitation, as there may be false-positive or false-negative results and its role still complementary. In the present study, a cutoff point (SUVmax 3.65) was successfully marked to discriminate positive versus negative local recurrence with specificity of 100% and p -value less than 0.001. A close cutoff point of SUVmax 3.2 was found to be ideal to detect structural disease by Abelleira et al with a specificity of 95%. 36
With regard to the prognostic role of ^18^ F-FDG PET/CT, several previous studies reported PET/CT parameters as promising prognostic markers in terms of disease progression and survival in patients with DTC. Pace et al 39 demonstrated that patients with no FDG avidity in FDG PET/CT scans have better progression-free survival whether in the whole group or in those with elevated TG. Salvatore et al 40 reported that Tg normalization and ^18^ F-FDG PET/CT were independent predictors of disease-free survival at short-term follow-up. Gaertner et al 41 concluded that FDG PET in high-risk DTC patients is predictive for survival when performed at the time of thyroid remnant ablation. In the current study, the ROC curve analysis revealed no cutoff points could be determined to predict the response to therapy or survival, likely due to heterogeneity of the enrolled risk groups.
This study has some limitations due to its retrospective design, which carries certain inherent limitations such as selection bias, as the data were collected from preexisting records. Also, relying on the retrieved data where stimulated Tg levels for all enrolled patients was available but unstimulated Tg and Tg Ab were not available for the entire population and therefore were not evaluated in the current study. This might influence the applicability of the findings. However, a strong point of the study is that to the best of our knowledge, the current study enrolled the largest number of DTC patients with BIR with comprehensive clinicopathological, laboratory, and imaging assessment.
Conclusion
BIR is a challenging event after radio-surgical treatment of DTC patients with no distinct consensus for management. In the current study, a considerable rate of structural locoregional recurrence was noted in such patients and was more commonly associating worse clinicopathological parameters. Tg is a core parameter for DRA in DTC, and its incremental levels carry the worse prognosis in BIR patients and seems to be linked to initial poor clinicopathological parameters and indicate higher incidence of structural disease recurrence. In the current study, ^18^ F-FDG PET/CT demonstrated a valuable diagnostic role rather than prognostic role for structural disease recurrence in BIR patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kim T Y Kim W G Kim W B Shong Y K Current status and future perspectives in differentiated thyroid cancer Endocrinol Metab (Seoul)2014290321722525309778 10.3803/En M.2014.29.3.217PMC 4192824 · doi ↗ · pubmed ↗
- 2Pitoia F Jerkovich F Dynamic risk assessment in patients with differentiated thyroid cancer Endocr Relat Cancer 20192610 R 553R 56631394499 10.1530/ERC-19-0213 · doi ↗ · pubmed ↗
- 3Tuttle R M Alzahrani A S Risk stratification in differentiated thyroid cancer: from detection to final follow-up J Clin Endocrinol Metab 2019104094087410030874735 10.1210/jc.2019-00177 PMC 6684308 · doi ↗ · pubmed ↗
- 4American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer Cooper D S Doherty G M Haugen B R Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer Thyroid 200919111167121419860577 10.1089/thy.2009.0110 · doi ↗ · pubmed ↗
- 5Pitoia F Ward L Wohllk N Recommendations of the Latin American Thyroid Society on diagnosis and management of differentiated thyroid cancer Arq Bras Endocrinol Metabol 2009530788488719942992 10.1590/s 0004-27302009000700014 · doi ↗ · pubmed ↗
- 6Luster M Aktolun C Amendoeira I European perspective on 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: proceedings of an interactive international symposium Thyroid 2019290172630484394 10.1089/thy.2017.0129 · doi ↗ · pubmed ↗
- 7Wang Y Wu J Jiang L Zhang X Liu B Prognostic value of post-ablation stimulated thyroglobulin in differentiated thyroid cancer patients with biochemical incomplete response: a bi-center observational study Endocrine 2022760110911535094313 10.1007/s 12020-021-02976-8 · doi ↗ · pubmed ↗
- 8Tuttle R M Optimal management of a biochemical incomplete response to therapy in differentiated thyroid cancer: aggressive treatment or cautious observation?Endocrine 2014460336336424615658 10.1007/s 12020-014-0213-2 · doi ↗ · pubmed ↗