Comparison of Meta-Analytical Estimates Between Surgical Repair and Transcatheter Edge-to-Edge Repair for Atrial Functional Mitral Regurgitation
Sherif Khairallah, Mohamed Rahouma, Michelle Demetres, Leonardo Girardi, Mario Gaudino, Aina Hirofuji, Mark Reisman, Stephanie L Mick

TL;DR
This study compares surgical and transcatheter treatments for atrial functional mitral regurgitation, finding that surgery may offer better long-term outcomes.
Contribution
The study provides a meta-analysis comparing surgical and transcatheter repair for atrial functional mitral regurgitation, highlighting long-term benefits of surgery.
Findings
Surgery was associated with decreased late severe MR and mortality compared to transcatheter repair.
Short-term outcomes were comparable between the two treatments.
High heterogeneity in long-term outcomes suggests the need for further validation.
Abstract
Atrial functional mitral regurgitation (MR) lacks well-defined treatment guidelines. Medical therapy alone is insufficient, and either TEER (transcatheter edge-to-edge) or surgery is recommended. Short- and long-term comparative outcomes remain unclear. We aim to address this gap using available data. We performed a meta-analysis of studies examining the outcomes of surgery and/or transcatheter edge-to-edge. MEDLINE, EMBASE, and the Cochrane Library were assessed. The incidence rate of late severe MR was the primary outcome. A random model was performed. Leave-one-out, subgroup, and meta-regression analyses were conducted. Thirty-two studies (1923 patients); 20 in surgery (1166) vs 12 in TEER (757), were selected. TEER patients were, on average, 10 years older, with twice the rate of New York Heart Association Classification (NYHA) III/IV symptoms and more than double the Society of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
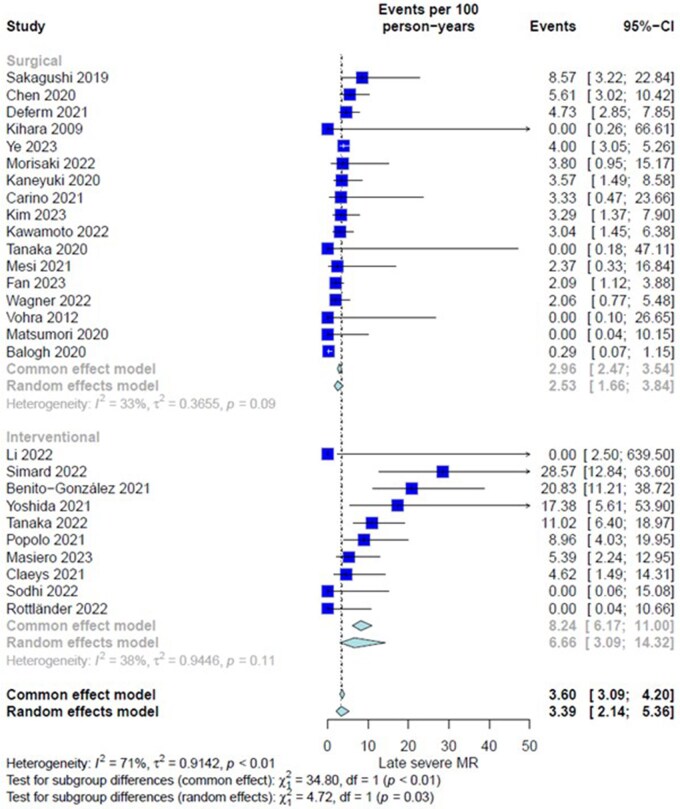 Figure 1
Figure 1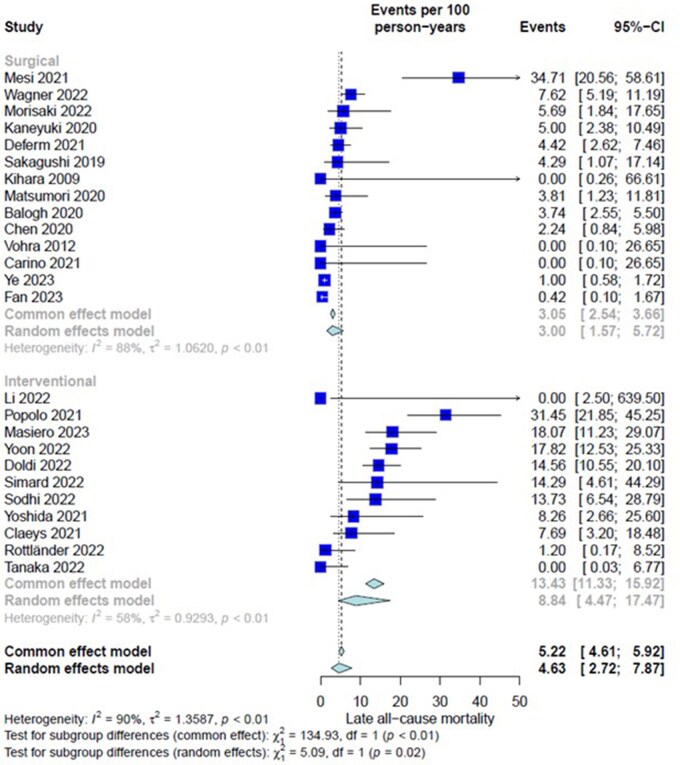 Figure 2
Figure 2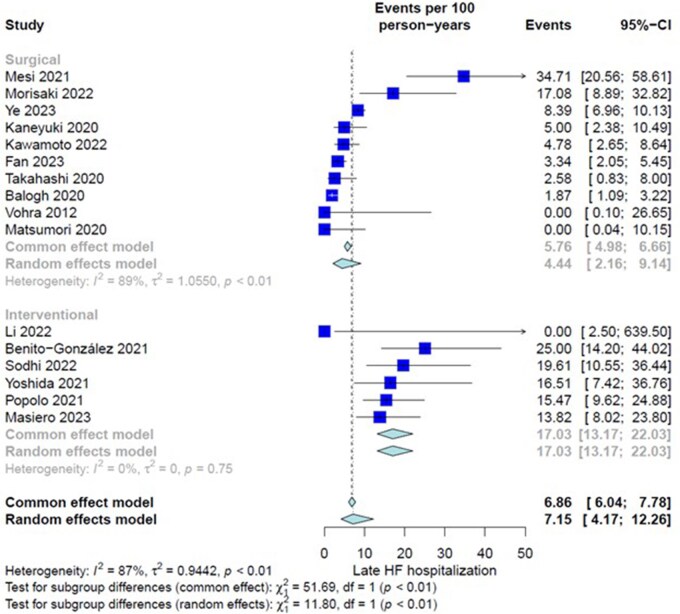 Figure 3
Figure 3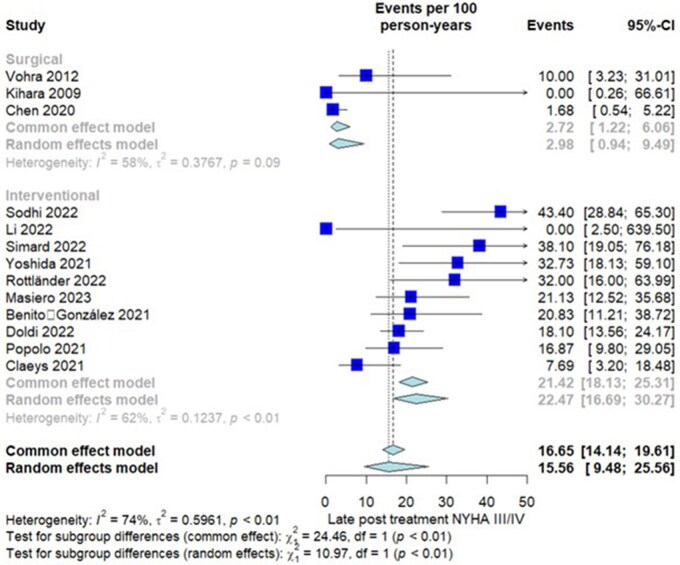 Figure 4
Figure 4| Study | Arm | Study years | Study type | Patients no | Age (years) (mean/median) | Female % | Preprocedural EF | Hypertension % | Diabetes % | CKD % | CAD % | COPD % | Dyslipidaemia % | Smoking % | Preprocedural NYHA III and IV | Preprocedural concomitant A Fib % | Preprocedural EuroSCORE II mean/median | Preprocedural STS risk score mean/median | Follow-up (months) (mean/median) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hirji et 2020 | S | 2002-2019 | R | 94 | 67.6 | 70.2 | 60 | 63.8 | 70.2 | 6.4 | 0 | 5.3 | 51.1 | NA | 42.6 | 37.2 | NA | 2.48 | 84 |
| Takahashi 2020 | S | 2008-2016 | R | 45 | 72 | 46.7 | 63 | 36 | 46.7 | 16 | 4 | 11 | 7 | NA | 67 | 100 | NA | NA | 31 |
| Deferm 2021 | S | 2010-2018 | R | 97 | 73 | 68 | 55 | 87.6 | 68 | 2.1 | 12.4 | NA | 67 | NA | 54 | 76.3 | 4.2 | NA | 39.6 |
| Balogh 2020 | S | 2003-2017 | R | 131 | 71.99 | 21.4 | 59.05 | 60.5 | 0.8 | 0.8 | 0 | 10 | NA | NA | 71 | 93.1 | NA | NA | 63.6 |
| Sakagushi 2019 | S | NA | R | 20 | 68 | 55 | 63.3 | 60 | 25 | 25 | NA | NA | 30 | NA | 35 | 100 | 3.4 | NA | 28 |
| Morisaki 2022 | S | 2008-2021 | R | 31 | 72.5 | 25 | PA: 60, MVR: 63 | 56.3 | 6.3 | 6.3 | NA | 12.5 | 12.5 | 50 | 56.3 | 100 | 2.81 | NA | 20.4 |
| Ohba Masanao 2020 | S | NA | R | 3 | 69.6 | 0 | 66.6 | NA | NA | NA | NA | NA | NA | NA | 0 | 100 | NA | NA | NA |
| Vohra 2012 | S | 2007-2011 | R | 20 | 77.5 | 70 | NA | 65 | 10 | 10 | 10 | NA | 65 | 30 | 50 | 100 | 8.1 | NA | 18 |
| Kaneyuki 2020 | S | 2011-2018 | R | 40 | 69 | 32 | NA | NA | NA | NA | NA | NA | NA | NA | 7.5 | 100 | NA | NA | 42 |
| Chen 2020 | S | 2008-2018 | R | 82 | 63.6 | 52.2 | 61.3 | 32.9 | 7.3 | 7.3 | NA | 4.9 | NA | 11 | 72 | 100 | NA | NA | 26.1 |
| Matsumori 2020 | S | 2000-2019 | R | 22 | 73.5 | 31.9 | 63.8 | 18.1 | 27.2 | 27.2 | NA | 63.6 | 27.2 | 36.3 | 31.7 | 100 | NA | NA | 42.96 |
| Tanaka 2020 | S | 2015-2018 | R | 10 | 72.4 | 60 | 52.2 | 60 | 10 | 10 | NA | NA | NA | NA | NA | 60 | NA | NA | 20.36 |
| Carino 2021 | S | NA | R | 20 | 72.2 | 90 | 55 | 55 | 20 | 20 | 5 | 10 | 15 | NA | 40 | 100 | 3.8 | NA | 18 |
| Kim 2023 | S | 2000-2020 | R | 36 | 66.5 | 53 | 57.9 | 39 | 23 | 23 | 0 | NA | NA | NA | 27 | 100 | NA | NA | 50.7 |
| Mesi 2021 | S | 2010-2018 | R |
| 70.4 | 56.4 | 60 | 94.9 | 46.2 | 46.2 | 48.7 | NA | 74.4 | 53.8 | 51.3 | 77 | NA | NA | 22 |
| Kihara 2009 | S | 2000- 2004 | R | 12 | 69 | 50 | 63 | NA | NA | NA | 0 | NA | NA | NA | 0 | 100 | NA | NA | 12 |
| Kawamoto 2022 | S | 2001-2019 | R | 50 | 74 | 42 | 69 | 66 | 4 | 4 | NA | 54 | 24 | NA | NA | 82 | NA | NA | 55.2 |
| Ye 2023 | S | 2010 - 2019 | P | 247 | 62.6 | 50.7 | 51 | 21.4 | 27.1 | 27.1 | 22.5 | 14.9 | NA | 42.6 | 65 | 100 | 2.3 | NA | 63.6 |
| Fan 2023 | S | 2012- 2015 | R | 60 | 63 | 36.7 | 56 | 26.7 | 16.7 | 16.7 | 18.3 | 6.7 | NA | NA | 33.3 | 100 | 2.5 | NA | 95.76 |
| Wagner 2022 | S | 2000-2020 | R | 123 | 62 | 55.3 | 58 | 58 | NA | 0 | NA | NA | NA | NA | 60.2 | NA | NA | 33.3 | |
| Tanaka 2022 | I (E-E) | 2010-2021 | R | 118 | 80 | 60.2 | 59.7 | 75.4 | 28.8 | 28.8 | 69.5 | 17.8 | NA | NA | 89 | 90.7 | 3.4 | NA | 12 |
| Doldi 2022 | I (E-E) | 2008-2019 | R | 126 | 80.3 | 61.1 | 57.1 | 84.9 | 17 | 17 | 41.4 | 16.7 | NA | NA | 85.7 | 78.6 | 4.7 | NA | 24.2 |
| Yoon 2022 | I (E-E) | 2007- 2020 | R | 116 | 78.8 | 56 | 61.9 | 83.6 | 30.2 | 30.2 | 42.2 | 7.8 | NA | NA | 94.8 | 72.4 | NA | 8.5 | 18 |
| Benito‐González 2021 | I (E-E) | 2012-2021 | R | 48 | 78 | 52.1 | 58 | 75 | 35.4 | 35.4 | 56.3 | 29.2 | 50 | NA | 89.6 | 100 | 4 | 4.6 | 12 |
| Claeys 2021 | I (E-E) | 2011-2019 | R | 52 | 79 | 54 | 59 | 79 | 21 | 21 | 30 | NA | NA | NA | 71 | 62 | 8 | NA | 15 |
| Li 2022 | I (E-E) | 6/2021-11/2021 | P | 5 | 70 | 60 | 58 | 60 | 0 | 0 | 0 | NA | NA | NA | 80 | 100 | NA | 5.14 | 3 |
| Simard 2022 | I (E-E) | 2014-2020 | R | 21 | 82 | 23.8 | 60 | 81 | 19 | 19 | 85.7 | 19 | NA | NA | 90.5 | 76.2 | NA | 8.4 | 12 |
| Sodhi 2022 | I (E-E) | 2018-2019 | P | 53 | 79.4 | 60.3 | 60.06 | NA | 26.4 | 26.4 | NA | 17 | NA | NA | 48.9 | 100 | NA | 6.8 | 12 |
| Masiero 2023 | I (E-E) | 2016-2020 | R | 71 | 79 | 58 | 55 | 85 | 26 | 26 | 34 | NA | 46 | 18 | 73 | 76 | 4.2 | NA | 15.9 |
| Rottländer 2022 | I (E-E) | 2014-2020 | R | 20 | 82.8 | 65 | 54 | 85 | 30 | 30 | 55 | NA | NA | 0 | 80 | 80 | NA | NA | 18 |
| Yoshida 2021 | I (E-E) | 2010-2018 | R | 40 | 83 | 52.5 | 58 | 78 | 33 | 33 | 27 | 30 | 30 | NA | 98 | 100 | NA | 7.8 | 10.9 |
| Popolo 2021 | I (E-E) | 2009- 2021 | R | 84 | 81 | 61 | 55 | 83 | 22 | 22 | NA | 21 | 21 | NA | 83 | 100 | 6 | 4 | 15.16 |
| Outcome | Studies | Patients | Estimate % (95% CI) | Heterogeneity ( |
|
|---|---|---|---|---|---|
| Early severe MR | 29 | 1580 | 4.78 (3.02-7.49) | 66%, |
|
| Surgical | 17 | 829 | 2.54 (1.46-4.39) | 0%, | |
| Interventional | 12 | 751 | 8.86 (5.42-14.17) | 71%, | |
| Early stroke | 16 | 1031 | 2.62 (1.72-3.98) | 0%, | .68 |
| Surgical | 13 | 921 | 2.49 (1.59-3.88) | 0%, | |
| Interventional | 3 | 110 | 3.74 (0.56-21.04) | 53%, | |
| Early AKI | 13 | 650 | 4.09 (2.38-6.94) | 17%, | .0504 |
| Surgical | 11 | 558 | 3.20 (1.73-5.85) | 8%, | |
| Interventional | 2 | 92 | 8.06 (3.99-15.61) | 0%, | |
| Early all-cause mortality | 30 | 1860 | 2.37 (1.68-3.34) | 0%, | .0515 |
| Surgical | 19 | 1143 | 1.65 ((1.00-2.72) | 0%, | |
| Interventional | 11 | 717 | 3.27 (2.04-5.21) | 0%, | |
| Early cardiac-specific mortality | 26 | 1418 | 1.92 (1.22-3.02) | 0%, | .33 |
| Surgical | 16 | 749 | 1.49 (0.74-2.95) | 0%, | |
| Interventional | 10 | 669 | 2.34 (1.28-4.24) | 0%, | |
| Early HF hospitalization | 18 | 940 | 3.33 (1.83-5.99) | 44%, | .96 |
| Surgical | 15 | 784 | 3.19 (1.58-6.34) | 47%, | |
| Interventional | 3 | 156 | 3.28 (1.31-8.00) | 0%, | |
| Early reoperation/reintervention | 20 | 969 | 2.96 (1.85-4.69) | 2%, | .22 |
| Surgical | 15 | 721 | 3.26 (1.89-5.56) | 9%, | |
| Interventional | 5 | 248 | 1.50 (0.48-4.57) | 0%, | |
| Postoperative mean LVESD (mm) | 10 | 705 | 32.93 (30.71-35.15) | 89%, | .30 |
| Surgical | 7 | 544 | 33.94 (32.36-35.52) | 80%, | |
| Interventional | 3 | 161 | 30.42 (24.01-36.83) | 95%, | |
| Postoperative mean LVEDD (mm) | 13 | 776 | 51.69 (46.57-56.81) | 94%- | .33 |
| Surgical | 9 | 517 | 49.18 (47.48-50.88) | 89%, | |
| Interventional | 4 | 259 | 57.78 (40.43-75.12) | 98%, | |
| Postprocedural Lt atrial diameter (mm) | 10 | 555 | 51.10 (48.91-53.28) | 87%, | .34 |
| Surgical | 7 | 345 | 50.45 (48.11-52.79) | 86%, | |
| Interventional | 2 | 210 | 56.15 (44.64-67.66) | 87%, | |
| Postprocedural mean EF | 15 | 1014 | 57.27 (55.38-59.15) | 95%, | .79 |
| Surgical | 9 | 643 | 57.03 (54.80-59.26) | 94%, | |
| Interventional | 6 | 371 | 57.60 (54.07-61.13) | 97%, | |
| Late severe MR (3+ and 4+) | 27 | 1478 | 3.39 (2.14-5.36) | 71%, |
|
| Surgical | 17 | 1021 | 2.53 (1.66-3.84) | 33%, | |
| Interventional | 10 | 457 | 6.66 (3.09-14.32) | 38%, | |
| Late reoperation | 17 | 690 | 1.62 (1.03-2.55) | 0%, | .17 |
| Surgical | 12 | 525 | 1.45 (0.87-2.41) | 0%, | |
| Interventional | 5 | 165 | 3.12 (1.18-8.24) | 0%, | |
| Late all-cause mortality | 25 | 1617 | 4.63 (2.72-7.87) | 58%, |
|
| Surgical | 14 | 924 | 3.00 (1.57-5.72) | 88%, | |
| Interventional | 11 | 693 | 8.84 (4.47-17.47) | 58%, | |
| Late cardiac-specific mortality | 16 | 859 | 1.36 (0.54-3.45) | 80%, | .23 |
| Surgical | 11 | 552 | 1.06 (0.47-2.40) | 51%, | |
| Interventional | 5 | 307 | 3.33 (0.61-18.09) | 40%, | |
| Late stroke | 13 | 884 | 0.51 (0.32-0.83) | 64%, | .35 |
| Surgical | 10 | 774 | 0.47 (0.28-0.78) | 18%, | |
| Interventional | 3 | 110 | 1.99 (0.10-39.25) | 74%, | |
| Late HF hospitalization/readmission | 16 | 968 | 7.15 (4.17-12.26) | 87%, |
|
| Surgical | 10 | 666 | 4.44(2.16-9.14) | 89%, | |
| Interventional | 6 | 302 | 17.03(13.17-22.03) | 0%, | |
| Late posttreatment NYHA III/IV | 13 | 587 | 15.56 (9.48-25.35) | 96%, |
|
| Surgical | 3 | 114 | 33.95 (24.90-46.28) | 51%, | |
| Interventional | 10 | 473 | 43.80 (24.59-78.01) | 97%, |
| Entire group | Surgery group | Intervention | |
|---|---|---|---|
|
| |||
| (β | (β | (β | |
| Late severe MR | |||
| Age | 0.0455 ± 0.0306, | −0.0554 ± 0.0456, | 0.0266 ± 0.1881, |
| Female % | 0.0058 ± 0.0151, |
| − |
| Preprocedural EF | −0.0048 ± 0.0599, | −0.0102 ± 0.0463, | 0.1833 ± 0.1559, |
| Preprocedural HF (NYHA class III/IV) | 0.0224 ± 0.0088, | −0.0017 ± 0.0121, |
|
| Hypertension | 0.016 ± 0.01, | 0.0006 ± 0.0101, | −0.0876 ± 0.0486, |
| Diabetes | 0.0211 ± 0.0157, | 0.0153 ± 0.0112, | 0.0168 ± 0.0624, |
| CKD | 0.0299 ± 0.02, | 0.0104 ± 0.0199, | 0.0168 ± 0.0624, |
| CAD | 0.0294 ± 0.0076, | 0.0222 ± 0.0198, | 0.0207 ± 0.0156, |
| COPD | −0.0064 ± 0.0232, | −0.0116 ± 0.0183, | 0.0725 ± 0.0476, |
| Dyslipidaemia | −9e−04 ± 0.0132, | 0.0055 ± 0.0081, | 0.0089 ± 0.0233, |
| Smoking | 7e−04 ± 0.0092, | −0.0095 ± 0.011, | ——— |
| Publication year | 0.1796 ± 0.1462, | 0.1287 ± 0.1238, | −0.5031 ± 0.5210, |
| Preprocedural concomitant AF | 0.0034 ± 0.0169, | 0.0064 ± 0.0161, | 0.0138 ± 0.0271, |
| Procedural EuroSCORE II mean | −0.0014 ± 0.1258, | 0.0005 ± 0.1335, | −0.186 ± 0.1356, |
| Preprocedural STS risk score mean | 0.0751 ± 0.2382, | NA | 0.0751 ± 0.2382, |
| Preprocedural Lt atrial diameter (mm) | 0.0189 ± 0.0317, | 0.0341 ± 0.0583, | −0.0086 ± 0.0404, |
| Preprocedural Lt atrial volume (mL) | −0.0085 ± 0.0066, | 0.0022 ± 0.0057, | 0.0167 ± 0.0092, |
| Preprocedural Lt atrial volume index (mL/m2) | 0.0035 ± 0.0088, | 0.0011 ± 0.0071, | 0.0689 ± 0.0536, |
| Group surgical LVEDD (mm) | 0.0136 ± 0.0255, | 0.0091 ± 0.0585, | 0.021 ± 0.0248, |
| Group surgical LVEDV (mL) | −0.0036 ± 0.0082, | −0.0009 ± 0.005, | −0.007 ± 0.0249, |
| Group surgical LVESD (mm) | −0.0496 ± 0.0471, | −0.0608 ± 0.0372, | 0.0195 ± 0.0512, |
| Preprocedural EROA (cm2) | 0.1464 ± 5.1177, | 27.7745 ± 16.9037, | 11.4679 ± 7.1088, |
| Preprocedural MR volume ml mean | −0.0004 ± 0.1687, | NA | 0.1085 ± 0.0486, |
| Preprocedural concomitant ≥2+ TR | 0.0013 ± 0.0109, | 0.003 ± 0.0095, | 0.0214 ± 0.0142, |
| MVr % | NA | 0.0004 ± 0.0114, | NA |
| MVR % | NA | −0.0156 ± 0.0229, | NA |
| Group surgical tricuspid | NA | 0.0167 ± 0.0126, | NA |
| Associated CABG % | NA | 0.0153 ± 0.012, | NA |
| Associated aortic valve % | NA | 0.0082 ± 0.013, | NA |
|
| |||
| Age | 0.0750 ± 0.0338, | 0.0496 ± 0.067, | −0.0711 ± 0.1577, |
| Female % | −0.0011 ± 0.01790, | −0.0067 ± 0.02, | −0.0179 ± 0.0322, |
| Preprocedural EF | 0.0669 ± 0.0842, | 0.12 ± 0.0858, | −0.0078 ± 0.1333, |
| Preprocedural HF (NYHA class III/IV) | 0.0171 ± 0.0110, | 0.0047 ± 0.0174, | −0.0085 ± 0.0245, |
| Hypertension |
|
|
|
| Diabetes | 0.0187 ± 0.0200, | 0.0238 ± 0.0179, | −0.0483 ± 0.0484, |
| CKD | 0.0338 ± 0.025, | 0.0312 ± 0.0253, | −0.0483 ± 0.0484, |
| CAD | 0.0155 ± 0.0148, | 0.0403 ± 0.0316, | −0.0201 ± 0.0191, |
| COPD | 0.0130 ± 0.0268, | 0.0144 ± 0.0174, | −0.0236 ± 0.0634, |
| Dyslipidaemia | 0.0093 ± 0.0165, | 0.0228 ± 0.0157, | −0.0219 ± 0.013, |
| Smoking | 0.0272 ± 0.0267, | 0.0507 ± 0.0334, | NA |
| Publication year | 0.1781 ± 0.1519, | 0.0951 ± 0.1473, | −0.0767 ± 0.5434, |
| MVr % | NA | − | NA |
| MVR % | NA |
| NA |
| Group surgical tricuspid | NA | −0.0205 ± 0.0164, | NA |
| Associated CABG % | NA | 0.0508 ± 0.0464, | NA |
| Associated aortic valve % | NA | 0.0773 ± 0.0371, | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Atrial Fibrillation Management and Outcomes · Cardiovascular Function and Risk Factors
FUTURE PERSPECTIVE
While we hypothesize that the superior outcomes of surgery compared to isolated TEER is related to the direct repair of the dilated mitral annulus, concomitant tricuspid valve repair and atrial fibrillation ablation, the causal relationship remains unclear. Randomized controlled trials are needed to further address this issue and establish optimal treatment recommendations for atrial functional mitral regurgitation.
INTRODUCTION
Functional mitral regurgitation (FMR) is classified into 2 subtypes: atrial functional mitral regurgitation (AFMR) and ventricular functional mitral regurgitation (VFMR), each with distinct pathophysiological mechanisms.1–3 VFMR typically results from ischaemic cardiomyopathy, characterized by reduced ejection fraction (EF), left ventricular dilation leading to papillary muscle displacement, and mitral annular dilation. AFMR, on the other hand, is often a long-term consequence of atrial fibrillation (AF), typically with preserved EF and progressive mitral annular dilation due to left atrial remodelling.3–5 AFMR was first described in 2010 by Gertz et al. Additionally, there is no consensus regarding the accurate definitions6 and specific echocardiographic parameters for AFMR.5 Some definitions focus on the presence of AF with progressive left atrial dilation, while others consider a history of AF exceeding 1 or 3 years. EF cutoffs also differ, ranging between 45% and 55%. Alternatively, some define AFMR as progressive left atrial dilation with preserved EF in patients with heart failure (HF), regardless of heart rhythm.6 Given the increasing prevalence of heart failure with preserved ejection fraction and AF over the past 50 years,7 AFMR is anticipated to become a more common form of FMR in the future.8
Treatment strategies differ. For VFMR, the primary approach combines medical management of HF with surgical mitral annulus reduction or transcatheter edge-to-edge repair (TEER).9^,^10 For AFMR, there is no consensus on the optimal treatment strategy (surgery vs TEER). Recent guidelines suggest surgery as a class IIb recommendation following failure of medical treatment, but there is still no consensus on utilizing TEER in AFMR.11–13 This meta-analysis aims to consolidate the evidence, with preliminary evaluation and comparison of surgical intervention vs TEER for AFMR using currently available data.
METHODS
This study was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).14 PROSPERO registration number is: CRD42024504022.
Search strategy
A medical librarian performed comprehensive searches to identify studies that compared or adopted surgical repairs and/or TEER for AFMR.
Searches were run on 6 December 2023, in the following databases: Ovid MEDLINE (1946 to Present), Ovid EMBASE (1974 to present), and The Cochrane Library (Wiley). Search strategy included all appropriate controlled vocabulary for the concepts of “atrial fibrillation” and “functional mitral regurgitation”. Full search strategies for all databases are available in Table S1. To limit publication bias, there were no restrictions on language, publication date, or article type in the search strategy.
Study selection
Retrieved studies were screened for inclusion. Titles and abstracts were reviewed against predefined inclusion/exclusion criteria by 2 independent reviewers. Discrepancies were resolved by consensus. For final inclusion, the full text was then retrieved and screened by 2 independent reviewers (S.K. and S.M.). No automation tools used for this process. Inclusion and exclusion criteria of studies are provided in Table S2.
Clinical outcomes and definitions
The primary outcome was the incidence rate (IR) of late severe MR (3+, and 4+). Secondary outcomes were early (30-day) stroke, early acute kidney injury (AKI), early all-cause mortality, early cardiac-specific mortality, early HF hospitalization, early reoperation/reintervention, postprocedural atrial, and ventricular reverse remodelling (left atrial diameter [mm], mean left ventricular end-systolic diameter (LVESD) [mm], mean left ventricular end-diastolic diameter (LVEDD) [mm], mean EF, late (beyond 30-day follow-up) reoperation, late all-cause mortality, late cardiac-specific mortality, late postprocedural New York Heart Association Classification (NYHA) III/IV, late stroke, late HF hospitalization/readmission). Data extracted from included studies were study details, baseline patient data such as demographics and comorbidities/history, echocardiographic data, procedural details, and outcomes such as postprocedural MR and all-cause mortality; a complete list of extracted data variables are given in Table S3.
Risk of bias (quality) assessment
Retrospective studies were assessed using the Newcastle-Ottawa scale (NOS).15 Using NOS, each study was judged on a total of 8 quality items from 3 categories: selection of study groups, comparability of groups, and the ascertainment of either the exposure or outcome of interest for case-control or cohort studies, respectively. Stars added for each quality item serve as a quick visual assessment with the highest quality studies receiving a maximum of 9 stars (Table S4). Two independent reviewers (S.K., M.R.) performed the quality assessment, and disagreements were resolved by a senior reviewer (S.M.). Publication bias was assessed visually using a funnel plot and statistically using Egger’s test.
Statistical analysis
Continuous variables were expressed as mean (SD). Short-term categorical variables were presented as proportions (pooled events), and time-to-event variables were presented as IR, with 95% CI. The minimum number of studies required to generate meta-analytic estimates was 3. All analyses were performed using “metafor”16 and “meta”17 packages in the R program (version 4.1.1) within RStudio.
For long-term events that were reported using Kaplan-Meier curves, the curves were digitized, and the individual patients’ data were reconstructed using an iterative algorithm18 that was applied to solve the Kaplan-Meier equations originally used to produce the published graphs. This algorithm used digitized Kaplan–-Meier curve data obtained by the Graph Grabber software package (Quintessa, Oxfordshire, UK) to find numerical solutions to the inverted Kaplan-Meier equation. To account for different follow-up times in the studies, an underlying Poisson process with a constant event rate was assumed with a total number of events observed within a group of the total person-time of follow-up for that group calculated from study follow-up.
Study heterogeneity was assessed using the Cochran Q statistic and the I^2^ test. For the primary outcome as well as for late all-cause mortality, a leave-one-out sensitivity analysis and funnel plots were performed for each of the study groups and for the whole cohort.
Analysis of subgroups or subsets
Subgroup analysis was used to compare surgery vs TEER for primary and secondary outcomes. There were no studies directly comparing both approaches; hence, we used a meta-analytical approach where a test for subgroup differences that checks whether the random effects estimate in the 2 subgroups differ was applied to the estimate for each reported cohort. This was done via metagen() or rma.uni() to calculate the Q statistic and P-value in meta or metafor packages, respectively16^,^17; This approach has been successfully utilized in prior meta-analyses.19–21 Meta-regression was used to assess the effect of age, female%, preprocedural factors (EF, NYHA class III/IV, hypertension, diabetes, chronic kidney disease, coronary artery disease [CAD], chronic obstructive pulmonary disease, dyslipidaemia, smoking, concomitant AF, EuroSCORE II and Society of Thoracic Surgeons Risk (STS)-PROM score means, left atrial diameter [mm], left atrial volume [mL], left atrial volume index [mL/m^2^], LVEDD [mm], LVEDV [mL], LVESD [mm], effective regurgitation orifice area [cm^2^], MR volume [mL], and concomitant ≥2+ TR), publication year, mitral valve repair %, mitral valve replacement (MVR)%, associated coronary artery bypass grafting%, associated aortic valve (AV) procedures% on the IR of the primary outcome (for the entire cohort, and for each study group separately). A random-effect model (inverse variance method) was used.
RESULTS
Characteristics of eligible studies
A total of 5516 articles were retrieved, and deduplication yielded 3877 articles. Thirty-two studies were ultimately included; the PRISMA flowchart is shown in Figure S1. A total of 1923 patients were included in this analysis (1166 in surgery vs 757 in TEER). The weighted mean follow-up time was 3.26 years (4.48 in surgery vs 1.41 in TEER). The weighted mean age was higher in the TEER group (69.52 [4.68] years in surgery vs 79.44 [1.4] years in TEER). The proportion of female patients was greater in the TEER group (55.33 [4.96%]) vs surgery (48.32 [14.22%]). The weighted mean preprocedural NYHA class III/IV was higher in the TEER group (81.96 ([10.66]) vs surgery (41.4 [12.9]). No significant difference was observed in the weighted mean preoperative EF (59.68 [15.6%] in surgery vs 57.98 [6.74%] in TEER). Systemic hypertension was more prevalent in the TEER group, with a weighted mean% of 79.08 (4.22%) vs 53.02 (20.7%) in surgery. The weighted mean of the preprocedural EuroSCORE II and STS-PROM scores were lower in surgery compared with TEER (EuroSCORE II: 3.87 [1.75] vs 5.05 [1.57], STS-PROM: 2.48 [3.26] vs 6.46 [1.65] for surgical and TEER groups, respectively). MR severity, indicated by weighted mean preprocedural left atrial and MR volumes, was higher in surgery (left atrial volume: 137.58 [36.48 mL]; MR volume: 58.05 [2.41 mL]) than TEER (left atrial volume: 77.1 [17.27 mL]; MR volume: 46.6 [5.57 mL]). The weighted mean% of preprocedural concomitant TR ≥ 2+ was higher in surgery (71.58 [12.5%]) than in TEER (56.19 [17.22%]). Baseline characteristics of the entire included cohort, the preprocedural echocardiographic data, as well as the weighted mean and weighted mean% of different variables are reported in Table 1, and Tables S5 and S6. No patients in the TEER group underwent transcatheter tricuspid valve (TV) repair or AF ablation procedures (Table S7). Detailed AF ablation and TV repair procedures can be found in Table S8.
Meta-analysis
Primary outcome: incidence rate of late severe mitral regurgitation (3+ and 4+)
Twenty-seven studies (1478 patients) were assessed. Overall IR of late severe MR for the entire cohort was 3.39 event per 100 person-year (PY) (CI = 2.14-5.36). There was high heterogeneity among included studies (I^2^ = 71%, *P *< .01). Subgroup analysis based on the repair intervention showed IR of 2.53 event per 100 PY (CI = 1.66-3.84) and 6.66 event per 100 PY (CI = 3.09-14.32) in Surgery and TEER groups, respectively (interaction-*P *= .03) (Figure 1, Table 2). Leave-one-out analysis showed robustness of the obtained estimate. Funnel plot (Figure S2) demonstrates absence of publication bias in both groups (Egger intercept was −0.786 [0.492], *P *= .131 vs −1.467 [1.0693], *P *= .207 in surgery and TEER groups, respectively).
Forest Plot, Subgroup Differences Between Surgery Group and Transcatheter Edge To Edge Repair Group for Incidence Rate of Late (Follow-Up) Recurrent Severe Mitral Regurgitation (MR).
On meta-regression, there was a significant association between increased IR of late severe MR and preprocedural NYHA class III/IV (β = 0.0224 [0.0088], *P *= .0111), and preprocedural CAD (β = 0.0294 [0.0076], *P *< .00001) across the entire group. In the surgery group, female gender was associated with increased IR of late severe MR (β = 0.0262 [0.0099], *P *= .0084). In the TEER group, preprocedural NYHA class III/IV (β = 0.0812 [0.0217], *P *< .001) and mean MR volume (β = 0.1085 [0.0486], *P *= .0256) were associated with increased IR of late severe MR, while female gender (β = −0.055 [0.023], *P *= .0167) was associated with decreased IR of late severe MR (Table 3).
Secondary outcomes
Late all-cause mortality
Twenty-five studies (1617 patients) were assessed. Overall IR of the entire group was 4.63 event per 100 PY (CI = 2.72-7.87). There was significant heterogeneity among included studies (I^2^ = 58%, *P *< .01). Subgroup analysis showed significantly higher IR of late all-cause mortality in the TEER group (3.00 [1.57-5.72] in surgery vs 8.84 [4.47-17.47] in TEER, interaction-P = .02) (Figure 2). On meta-regression, significant associations were found between increased IR of late all-cause mortality and both advanced age (β = 0.0750 [0.0338], *P *= .0263) and preprocedural hypertension (β = 0.0365 [0.0087], *P *< .001) across the entire cohort (Table 3). Within the surgical group, preprocedural hypertension (β = 0.0343 [0.0090], *P *< .001), MVR (β = 0.0508 [0.0131], *P *< .001), and associated AV surgery were significantly linked to an increased IR of late all-cause mortality. In the TEER group, hypertension was the sole variable associated with an increased IR of late all-cause mortality (β = .2034 [0.1057], *P *= .0542) (Table 3).
Forest Plot, Subgroup Differences Between Surgery Group and Transcatheter Edge To Edge Repair Group for Incidence Rate of Late (Follow-Up) All-Cause Mortality.
Late HF hospitalization/readmission
Sixteen studies (968 patients) were assessed. Overall IR in the entire group was 7.15 events per 100 PY (CI = 4.17-12.26). There was significant heterogeneity among included studies (I^2^ = 87%, *P *< .01). Subgroup analysis showed a significantly higher IR of late HF readmission in the TEER group (4.44 [2.16-9.14] in surgery vs 17.03 [13.17-22.03] in TEER, interaction-*P *< .01) (Figure 3).
Forest Plot, Subgroup Differences Between Surgery Group and Transcatheter Edge To Edge Repair (TEER) Group for Incidence Rate of Late (Follow-Up) Heart Failure (HF) Hospitalization/Re-Admission.
Late postprocedural NYHA III/IV
Thirteen studies (587 patients) were assessed. Overall IR in the entire group was 15.56 event per 100 PY (CI = 9.48-25.56). There was significant heterogeneity among included studies (I^2^ = 96%, *P *< .01). Subgroup analysis showed significantly higher IR of late postprocedural NYHA III/IV in the TEER group (2.98 [0.94-9.49] in surgery vs 22.47 [16.69-30.27] in TEER, interaction-*P *= .01) (Figure 4).
Forest Plot, Subgroup Differences Between Surgery Group and Transcatheter Edge To Edge Repair Group for Incidence Rate of Late (Follow-Up) Postprocedural New York Heart Association Classification (NYHA) III/IV.
Early AKI
Thirteen studies (650 patients) were assessed. Overall pooled events in the entire cohort were 4.09 events per 100 PY (CI = 2.38-6.94). There was mild heterogeneity among included studies (I^2^ = 17%, *P *= .27). Subgroup analysis showed no significant difference between groups (interaction-*P *= .0504) (Figure S3).
Early all-cause mortality
Thirty studies (1860 patients) were assessed. Overall pooled events in the entire cohort were 2.37 events per 100 PY (CI = 1.68-3.34). There was no heterogeneity among included studies (I^2^ = 0%, *P *= .84). Subgroup analysis did not show a significant difference between groups (interaction-*P *= .0515) (Figure S4).
Early cardiac-specific mortality
Twenty-six studies (1418 patients) were assessed. Overall pooled events in the entire cohort were 1.92 event per 100 PY (CI = 1.22-3.02). There was no heterogeneity among included studies (I^2^ = 0%, *P *= .95). Subgroup analysis did not show significant difference between groups (interaction-*P *= .33) (Figure S5).
Early stroke
Sixteen studies (1031 patients) were assessed. Overall pooled events in the entire cohort were 2.62 events per 100 PY (CI = 1.72-3.98). There was no heterogeneity among included studies (I^2^ = 0%, *P *= .72). Subgroup analysis showed no significant difference between groups (interaction-*P *= .68) (Figure S6).
Early HF hospitalization
Eighteen studies (940 patients) were assessed. Overall pooled events in the entire cohort were 3.33 events per 100 PY (CI = 1.83-5.99). There was significant heterogeneity among included studies (I^2^ = 44%, *P *= .02). Subgroup analysis did not show significant difference between groups (interaction-*P *= .96) (Figure S7).
Early reoperation/reintervention
Twenty studies (969 patients) were assessed. Overall pooled events in the entire cohort were 2.96 events per 100 PY (CI = 1.85-4.69). There was no significant heterogeneity among included studies (I^2^ = 2%, *P *= .44). Subgroup analysis did not show significant difference between groups (interaction-*P *= .22) (Figure S8).
Postprocedural atrial and ventricular reverse remodelling
Mean left atrial diameter (mm)
Ten studies (555 patients) were assessed. There was significant heterogeneity among included studies (I^2^ = 87%, *P *< .01). Subgroup analysis did not show significant difference between groups (50.45 [CI = 48.11-52.79] in surgery vs 56.15 [CI = 44.64-67.66] in TEER, interaction-*P *= .34) (Figure S9).
Mean LVESD (mm)
Ten studies (705 patients) were assessed. There was significant heterogeneity among included studies (I^2^ = 89%, *P *< .01). Subgroup analysis did not show significant difference between groups (33.94 [32.36-35.52] in surgery vs 30.42 [24.01-36.83] in TEER, interaction-*P *= .30) (Figure S10).
Mean LVEDD (mm)
Thirteen studies (776 patients) were assessed for this outcome. There was significant heterogeneity among the included studies (I^2^ = 94%, P < .01) (Figure S11). Subgroup analysis did not show any significant difference between both groups (49.18 [47.48-50.88] in surgery vs 57.78 [40.43-75.12] in TEER, interaction-P = .33) (Figure S11).
Postprocedural mean EF
Fifteen studies (1014 patients) were assessed. Mean EF in the entire cohort was 57.27 (55.38-59.15) with significant heterogeneity among included studies (I^2^ = 95%, *P *< .01). Subgroup analysis did not show significant difference between groups (57.03 [54.80-59.26] in surgery vs 57.60 [54.07-61.13] in TEER, interaction-*P *= .79) (Figure S12).
Late reoperation
Seventeen studies (690 patients) were assessed. Overall IR in the entire group was 1.62 events per 100 PY (CI = 1.03-2.55). There was no significant heterogeneity among included studies (I^2^ = 0%, *P *= .52). There was no significant difference between groups in the subgroup analysis (interaction-*P *= .17) (Figure S13).
Late cardiac-specific mortality
Sixteen studies (859 patients) were assessed. Overall IR in the entire group was 1.36 events per 100 PY (CI = 0.54-3.45). There was significant heterogeneity among included studies (I^2^ = 80%, *P *= .01). There was no significant difference between groups in the subgroup analysis (interaction-*P *= .23) (Figure S14).
Late stroke
Thirteen studies (884 patients) were assessed. Overall IR in the entire group was 0.51 events per 100 PY (CI = 0.32-0.83). There was significant heterogeneity among included studies (I^2^ = 64%, *P *< .01). There was no significant difference between groups in the subgroup analysis (interaction-*P *= .35) (Figure S15).
DISCUSSION
To the best of our knowledge, this is the only meta-analysis comparing early and late outcomes of surgical and transcatheter MV interventions for AFMR. Our main findings were that, compared to isolated mitral TEER, surgical intervention (including mitral annuloplasty, concomitant AF ablation, and/or TV repair) was associated with decreased IR of:
Late severe MR (2.53 vs 6.66 events per 100 PY, P-interaction = .03)Late all-cause mortality (3.00 vs 8.84 events per 100 PY, P-interaction = .024)Late HF hospitalization/readmission (4.44 vs 17.03 events per 100 PY, P-interaction < .01)Late NYHA III/IV (2.98 vs 22.47 events per 100 PY, P-interaction < .01)Both groups were comparable in IR of early all-cause mortality, early cardiac-specific mortality, late cardiac-specific mortality, postprocedural morbidities (AKI and early stroke), and postprocedural atrial and ventricular reverse remodelling.
We attribute the better outcome of surgical intervention over TEER to concomitant interventions such as mitral annuloplasty, AF ablation, and TR repair that address other aspects of AFMR pathophysiology including atrial fibrillation and TR.
Early and late severe mitral regurgitation
Our study demonstrated that IR of early and late recurrent MR was significantly higher in TEER compared to surgery. An explanation is that surgery directly repairs annular dilation, the primary cause of AFMR, while TEER only approximates leaflets, and its effect on the annulus is not as direct as surgery.
Several studies have reported mitral annular diameter decrease following TEER, particularly in patients with FMR,22–27 supporting the treatment rationale. Patzelt et al. reported a reduction in mitral annular diameters in VFMR at patient follow-up28; however, we could not analyse this reduction due to data unavailability. Therapeutic left ventricular remodelling after TEER can also be assessed by a reduction in LVEDD.29 Our analysis showed both interventions resulted in comparable reductions in left atrial and left ventricular diameters, with slight benefit associated with the surgical group despite their relatively larger preprocedural left atrial and left ventricular diameters and volumes. These findings further suggest that superior outcomes associated with surgery may stem from its direct repair of the mitral annulus, while TEER relies on delayed cardiac remodelling.
To our knowledge, no comparative studies or randomized controlled trials (RCTs) have directly compared surgery to TEER for AFMR, as opposed to VFMR. The EVEREST II trial30^,^31 is the only trial comparing TEER to surgical interventions, but for different aetiologies of MR. The trial reported superior safety and similar improvements in clinical outcomes for TEER, despite less MR reduction than surgery. In a subgroup of patients with unspecified FMR, freedom from death, MV surgery, and MR grade ≥3+ was 54% in TEER vs 50% in surgery (*P *= .02). At 5 years, the incidence of 3+/4+ MR and surgery for MV dysfunction increased in the TEER group, particularly during the first year.32 Despite different aetiologies for MR between trials, our results align with those of the EVEREST II trial regarding the incidence of late recurrent MR and safety of the TEER procedure. The EVEREST II trial and our results suggest that, regardless of baseline comorbidities, surgery offers better outcomes. It is well documented that surgical outcomes are generally better for AFMR compared to VFMR with regard to operative and all-cause mortality, survival, and MR recurrence,33^,^34 whereas superior results of TEER vs surgery in the VFMR group have been reported.35 However, our meta-analysis suggests that surgical outcomes are better for AFMR than for TEER group. We believe that differences in TEER outcomes between VFMR and AFMR stem from anatomical and pathophysiological differences. Mitral leaflets in VFMR often have tethering and an anatomic target for TEER, while AFMR generally has MR across the entire coaptation plane without a focused target. Additionally, follow-up period for the TEER group in our meta-analysis was only 12 months, leaving the possibility of outcome improvement with longer follow-up after TEER. Another concern is the different generations of TEER devices used across various studies and enrolment periods, as there have been technological advancements linked to improved outcomes and durability, as indicated by the EXPAND study.36 The novel PASCAL (Precision Transcatheter Valve Repair System, Edwards Lifesciences, Irvine, CA) system has not yet been used for AFMR,37 and there have been no direct comparative studies between Mitra-Clip (Abbott, Santa Clara, CA) and PASCAL until the ongoing Clinical Long-term Assessment of the Safety and Performance of the PASCAL System (CLASP) IIF RCT in FMR patients (NCT03706833) that might introduce more definitive data.
Associated AF ablation procedures
In our study, approximately 89% of the surgical group and 86% of the TEER group had preprocedural AF. Most patients in the surgical group underwent concomitant AF ablation with or without left atrial appendage exclusion (863/1162, 74.3%), without any in the TEER group where the majority received medical treatment for AF (Tables S7 and S8). It is well established that AF is a significant predictor of worse early and late survival after surgical repair of MR,38^,^39 regardless of aetiology,40 and is associated with subsequent HF deterioration,41 even after TEER.42-44
A meta-analysis involving 7678 patients revealed that persistent AF after TEER was associated with increased risks of 1-year all-cause mortality, HF hospitalization, and bleeding.42 Although medical management of AF was associated with an equivalent reduction in MR severity compared to transcatheter ablation,45 many studies revealed superior long-term outcomes with transcatheter ablation.2^,^46–50 The CAMERA-MRI RCT reports an improvement in left ventricular ejection fraction (LVEF) with transcatheter AF ablation compared with medical AF management (16.4% vs 8.6%, *P *= .001) in patients with AF and systolic dysfunction.48 In patients with FMR, transcatheter ablation demonstrated similar results, along with a significant reduction in MR severity.47 Moreover, combining surgery with transcatheter ablation demonstrated greater reduction in MR severity and a decrease in late HF readmissions as compared with transcatheter ablation alone.51
Based on prior studies, lack of proper AF control after TEER may explain the superior outcomes of surgery, given the feasibility, safety, and good outcomes of transcatheter ablation after TEER as reported by Rottner et al.52 This underscores the importance of rhythm control in patients with AF undergoing mitral valve interventions, whether surgical or percutaneous.
Associated tricuspid repair procedures
Our analysis revealed that 71.58% of the surgical group and 56.18% of the TEER group had concomitant TR >2+. AFMR is frequently accompanied by atrial functional TR (AFTR).40^,^53–57 Many studies report that moderate to severe TR adversely affect survival, independent of EF or pulmonary artery systolic pressure,58–61 particularly in patients with impaired LVEF, but not for those with end-stage HF.62 Despite poor prognosis and the class IIa indication by the American College of Cardiology/American Heart Association valve disease guidelines for patients with symptomatic severe AFTR,11 open-heart repair was seldom performed for isolated AFTR due to concerns regarding mortality.63 There is currently no consensus on optimal timing for intervention in AFTR, given the paucity of data regarding TR severity, annular size, or right ventricular (RV) function.64 Another important note is, surgical referral is often delayed until the condition progresses to severe right ventricular dysfunction adding to higher procedural risks.64 However, many studies recommend TR repair, for its greater benefits with intervention before the onset of RV, hepatic, and/or renal dysfunction.64
In addition, recent evidence suggests that rhythm control for AF via transcatheter ablation and/or electrical cardioversion can significantly reduce TR severity.65 The role of percutaneous interventions for AFTR is still evolving, data from the international multicentre TriValve registry demonstrate the safety and feasibility of percutaneous interventions.57 Procedural success was achieved in 62% of cases, with all-cause mortality of 3.7% and major adverse cardiac and cerebrovascular events in 26% of patients, and 58% of patients improved to NYHA class I or II at 30 days.57
In this meta-analysis, we did not find explanations of the absence of TR intervention nor AF ablative procedure in the TEER group despite the established efficacy and safety of such procedures; This could have accounted for the superior outcomes in the surgical group (746/1165, 64.0% in the surgery group underwent concomitant TR repair). This highlights the need for a more comprehensive approach in managing concomitant TR in AFMR patients.
Limitations
First, there is variability in the definitions,6 inclusion criteria,6 and echocardiographic characteristics5 across the included studies in both groups. Also, missing data and inconsistencies in reporting among the included studies hindered our ability to conduct subgroup analyses. Moreover, there were limitations related to the meta-analytical approach itself, as there were no direct comparative studies between both approaches. Another limitation is the heterogeneity of the baseline preoperative characteristics between both groups. Most patients in the TEER group were older, had more associated comorbidities and higher STS-PROM and EuroSCORE II values, which may have introduced selection bias and affect outcomes.
Advancement of technology, especially TEER devices, may have influenced outcomes. Different generations of Mitra-Clip were used in the included TEER studies, which could have affected the results.
Also, the follow-up duration for the TEER group was significantly shorter. This constraint prevents us from assessing longer-term outcomes. Lastly, heterogeneity among the surgical techniques employed in the surgical group may have contributed to the observed differences in outcomes. Because of these limitations, it is difficult to arrive at definitive conclusions from this limited data, and the findings from this study are perhaps best regarded as hypothesis-generating.
CONCLUSION AND RECOMMENDATION
Based on the results of this meta-analysis, both surgical intervention and TEER for AFMR confer comparable results regarding short-term outcomes (early HF hospitalization, early mortality, and early intervention). TEER patients were older and had higher comorbidity indices. However, surgery appears to be superior to TEER in terms of immediate reduction in MR severity and beneficial long-term outcomes, including lower rates of late recurrent severe MR, HF hospitalization, all-cause mortality, and NYHA Class III and IV symptoms. This might be attributed to correction of mitral annular dilatation, more complete AF ablation, intervention to TR when necessary, and more adverse comorbidities of the TEER group. However, given the proven feasibility, safety, and effectiveness of transcatheter approaches, whether combining transcatheter TR repair and AF ablation with MR TEER could potentially enhance the outcomes of TEER vs surgery is not known and should be further tested and explored in clinical practice.
Supplementary Material
ivaf269_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Asgar AW , Mack MJ, Stone GW. Secondary mitral regurgitation in heart failure: pathophysiology, prognosis, and therapeutic considerations. J Am Coll Cardiol. 2015;65:1231-1248.25814231 10.1016/j.jacc.2015.02.009 · doi ↗ · pubmed ↗
- 2Gertz ZM , Raina A, Saghy L, et al Evidence of atrial functional mitral regurgitation due to atrial fibrillation: reversal with arrhythmia control. J Am Coll Cardiol. 2011;58:1474-1481.21939832 10.1016/j.jacc.2011.06.032 · doi ↗ · pubmed ↗
- 3Abe Y , Takahashi Y, Shibata T. Functional mitral regurgitation, updated: ventricular or atrial? J Echocardiogr. 2020;18:1-8.31728977 10.1007/s 12574-019-00453-w · doi ↗ · pubmed ↗
- 4Reid A , Zekry SB, Naoum C, et al Geometric differences of the mitral valve apparatus in atrial and ventricular functional mitral regurgitation. J Cardiovasc Comput Tomogr. 2022;16:431-441.35361564 10.1016/j.jcct.2022.02.008 · doi ↗ · pubmed ↗
- 5Farhan S , Silbiger JJ, Halperin JL, et al Pathophysiology, echocardiographic diagnosis, and treatment of atrial functional mitral regurgitation: JACC state-of-the-art review. J Am Coll Cardiol. 2022;80:2314-2330.36480974 10.1016/j.jacc.2022.09.046 · doi ↗ · pubmed ↗
- 6Amabile A , Fereydooni S, Mori M, et al Variable definitions and treatment approaches for atrial functional mitral regurgitation: a scoping review of the literature. J Card Surg. 2022;37:1182-1191.35179258 10.1111/jocs.16312 · doi ↗ · pubmed ↗
- 7Schnabel RB , Yin X, Gona P, et al 50 Year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386:154-162.25960110 10.1016/S 0140-6736(14)61774-8PMC 4553037 · doi ↗ · pubmed ↗
- 8Chen J , Wang Y, Lv M, et al Mitral valve repair and surgical ablation for atrial functional mitral regurgitation. Ann Transl Med. 2020;8:1420.33313165 10.21037/atm-20-2958 PMC 7723636 · doi ↗ · pubmed ↗