Aetiology and impact of bacterial bloodstream infections in mechanically ventilated COVID-19 patients: A prospective Swedish multicenter cohort study
Isak Olsson, Anna C. Nilsson, Ingrid Didriksson, Attila Frigyesi, Hans Friberg, Anton Reepalu, Martin Spångfors, Lorenzo Righi, Anton Sokhan, Anton Sokhan, Anton Sokhan

TL;DR
This study found that 17% of critically ill COVID-19 patients on ventilators in Sweden developed bloodstream infections, which were linked to longer ICU stays and higher mortality.
Contribution
The study provides new insights into the risk factors and impact of ICU-acquired bacterial bloodstream infections in ventilated COVID-19 patients in a Nordic setting.
Findings
Staphylococcus aureus was the most common pathogen in ICU-acquired bloodstream infections.
Patients with BSI had significantly longer ICU and hospital stays and higher mortality.
Predictive factors for BSI included higher BMI, diabetes with complications, and longer pre-ICU symptoms.
Abstract
Critically ill COVID-19 patients admitted to the intensive care unit (ICU) are at an increased risk of acquiring bacterial bloodstream infections (BSI). We aimed to describe patient characteristics, risk factors, and the microbiological spectrum in blood cultures and evaluate the impact of ICU-acquired BSI on outcomes in a Nordic setting. A prospective multicenter cohort study was conducted on adult invasively mechanically ventilated (IMV) COVID-19 patients. The primary aim was to identify the proportion of ICU-acquired BSI and its aetiology. Secondary outcomes were duration of IMV, length of stay (LOS), and mortality for individuals with and without BSI, respectively. Logistic regression was used to identify potential predictors of ICU-acquired BSI. Predictors were assessed by calculating an Area Under the Receiver Operating Characteristics (AUROC) curve. Of 354 included patients,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
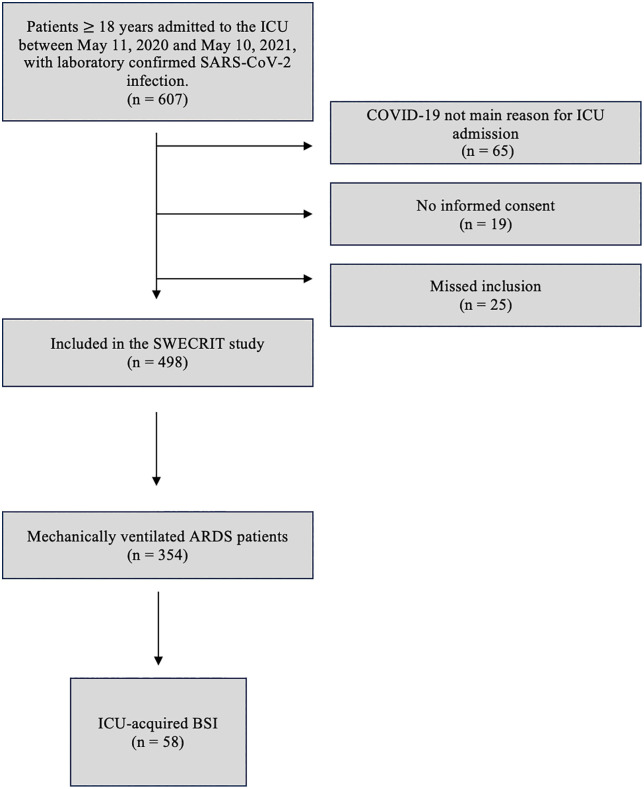 Fig 1
Fig 1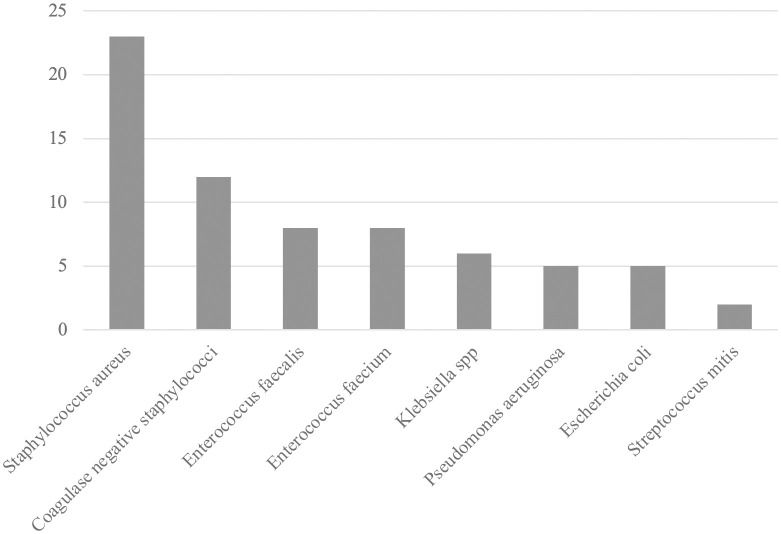 Fig 2
Fig 2- —The Swedish National Health Service (ALF)
- —Region Skåne
- —http://dx.doi.org/10.13039/501100003793Hjärt-Lungfonden
- —http://dx.doi.org/10.13039/501100011077Skånes universitetssjukhus
- —http://dx.doi.org/10.13039/501100017237Hans-Gabriel och Alice Trolle-Wachtmeisters stiftelse för medicinsk forskning
- —Region Skåne
- —Swedish National Health Service (ALF)
- —Swedish National Health Service (ALF)
- —http://dx.doi.org/10.13039/501100003173Crafoordska Stiftelsen
- —Lions Skåne
- —http://dx.doi.org/10.13039/501100011077Skånes universitetssjukhus
- —http://dx.doi.org/10.13039/501100003793Hjärt-Lungfonden
- —http://dx.doi.org/10.13039/501100003793Hjärt-Lungfonden
- —Region Skåne
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNosocomial Infections in ICU · Antibiotic Use and Resistance · Sepsis Diagnosis and Treatment
Introduction
Most patients with Coronavirus Disease 19 (COVID-19) have mild to moderate respiratory tract infection symptoms or remain asymptomatic [1–3]. A minority develop severe symptoms and critical disease with acute respiratory distress syndrome (ARDS), requiring intensive care with advanced respiratory support including invasive mechanical ventilation (IMV) [2,4,5]. Vaccines against the SARS-CoV-2 virus have dramatically decreased progress to a life-threatening disease [6]. SARS-CoV-2 remains in circulation in society, continuously infecting the public since neither vaccine-induced immunity nor immunity acquired through infection offers complete protection, particularly among the immunocompromised and other vulnerable populations [7,8].
In general, patients treated in intensive care units (ICU) are at high risk of acquiring infectious complications like pneumonia, urinary tract infection or bloodstream infection (BSI). Common risk factors are IMV, intravenous lines and urinary catheters [9]. Risk factors of infectious complications in hospitalised COVID-19 patients include use of broad-spectrum antibiotics, longer ICU-length of stay (ICU-LOS) and hospital length of stay (hospital-LOS), development of ARDS and duration of IMV [10–12]. Common secondary infections include respiratory tract infections and BSIs [10,13,14]. Staphylococcus aureus and Escherichia coli are common causes of secondary bacterial BSIs [15]. Bacterial BSIs in COVID-19 patients are associated with worse outcomes, e.g., higher rate of ICU admission, need for IMV and increased mortality [16,17]. A higher frequency of bacterial co-infections has been found in critically ill COVID-19 patients compared to critically ill non-COVID-19 patients [18]. In a Swedish context, one study identified a low rate (6.5%) of positive blood cultures among hospitalised COVID-19 patients [19]. Another study, however, found a higher incidence of hospital-acquired BSIs in COVID-19 patients compared to non-COVID-19 patients [20]. Given the implications of antimicrobial resistance on both acquisition and outcome of BSI, it is important to note that there have been a lower reported rate of antimicrobial resistance in the Nordic countries compared to the other parts of Europe [21]. The rate of deaths by antimicrobial resistance is also lower in the Nordic countries compared to other countries [22]. There is no consensus regarding which factors increase the risk of concurrent infections in critically ill COVID-19 patients [11,14,16,23].
This study aimed to describe patient characteristics and the microbiological spectrum in blood cultures from critically ill COVID-19 patients receiving IMV in the ICU in a Nordic context. Furthermore, we investigated the impact of ICU-acquired BSIs on the duration of IMV, ICU-LOS, hospital-LOS, and 365-day all-cause mortality. Potential patient-specific predictors associated with an ICU-acquired BSI at ICU admission were explored.
Materials and methods
Study design
This study was part of the prospective multicenter cohort study SWECRIT COVID-19, including adult patients (≥18 years old) with laboratory-confirmed critical COVID-19 infection treated at the ICU in any of four participating hospitals in the Skåne region, Sweden [24]. Patients were consecutively included on admission to the ICUs at Helsingborg Hospital, Kristianstad Hospital, Skåne University Hospital in Lund and Malmö between May 11, 2020, and May 10, 2021. The participating hospitals adhered to the same regional recommendations and had equal access to resources, such as alcohol-based hand disinfection, mouthguards, and gloves during the pandemic. The virus strain B.1.1.7 (alpha) prevailed throughout the study period, and the vaccine coverage was low throughout the study period [24]. Patients whose COVID-19 was not the primary cause of ICU admission were excluded. Only patients with ARDS receiving IMV were included in this study.
Data collection
The data collection of background variables has previously been described in detail [22]. In brief, demographic, radiographic, laboratory data, and medication during the ICU stay were obtained from electronic medical records and a regional quality registry, COVID-IR. Data regarding blood culture sets and culture results were extracted from COVID-IR for each patient from five days before hospital admission until the end of the ICU stay. Furthermore, treatment with antibiotic agents during this time frame was collected through COVID-IR.
Ethical approval
Written informed consent was obtained at ICU admission. If the patient could not make an informed decision due to the acute medical condition, consent was obtained up to one year after ICU admission. For deceased patients, consent was presumed. Ethical approval was approved by the Swedish Ethical Review Authority (DNR 2020/01955, 2020/03483 & 2020/05233). The manuscript was prepared following the STROBE guidelines for observational studies [25].
Definitions
The ARDS was defined according to the Berlin definition, which states bilateral opacities on chest radiograph or computed tomography in combination with an arterial oxygen partial pressure ratio to fractional inspired oxygen (PaO_2_/FiO_2_) ≤40 kPa and a positive end-expiratory pressure (PEEP) of ≥5 cm H_2_O. Participants were stratified into mild, moderate or severe ARDS based on the PaO_2_/FiO_2_ ratio [26].
Blood cultures were drawn based on clinical judgment and suspicion of bloodstream infection. There was no local protocol specific for COVID-19 regarding when to collect blood cultures or when to suspect a bloodstream infection. However, regional guidelines state when a clinician should suspect that a patient has sepsis. If a patient presents with clinical signs of sepsis in line with the Surviving Sepsis Campaign Adult Guidelines [27], then a specific sepsis alarm should be activated. If a patient fulfills these criteria blood cultures are routinely collected [28]. However, there might have been situations when blood cultures were drawn based on based on other information or signs of infection that are not specifically stated in the regional guidelines. The regional recommendations state that four blood culture bottles, two aerobic and two anaerobic samples, with a total blood volume of 40 ml, should be obtained before administering intravenous antibiotics. All cultures were analysed using the BD BACTEC FX blood culture system (Becton, Dickinson and Co., USA) at the regional clinical microbiology laboratory in Lund, Sweden, which is accredited according to the ISO 15189 standard.
Positive blood cultures obtained >48 hours after ICU admission to <48 hours after ICU discharge were defined as ICU-acquired infections [10]. Positive blood cultures obtained 5 days before hospital admission and up to 48 hours after hospital admission were defined as community-acquired BSIs, whilst positive cultures obtained >48 hours after hospital admission but <48 hours after ICU admission were defined as hospital ward-acquired BSIs [15]. Furthermore, ICU-acquired BSIs were divided into early and late, depending on whether the positive culture was obtained ≤7 days after ICU admission or later [29]. If a patient acquired an early and late infection, the patient was only included in the first group, i.e., the early infection subgroup.
In the participating ICU’s, the first line of antibiotic treatment used for empirical treatment of ICU patients with Covid-19 and suspected bacterial co-infection was third generation Cephalosporins (mainly Cefotaxime), and the second line of treatment was Carbapenems or Piperacillin-tazobactam.
Coagulase-negative staphylococci, “viridans”-group streptococci, Bacillus species, Corynebacterium species, Micrococcus species, Cutibacterium acnes and related species were considered probable skin contaminants in blood samples [30,31]. Probable skin contaminants had to be identified in more than one blood sample drawn on the same occasion to be considered a significant finding [30,31]. See S1 Table for the complete classification of pathogens.
The updated version by Quan et al. (2011) was used to calculate the Charlson Comorbidity Index (CCI) [32].
Outcome measures
The primary outcome was the proportion and aetiology of ICU-acquired BSIs. The secondary outcomes were duration of IMV, ICU-LOS, hospital-LOS, and ICU-, hospital-, and 365-day all-cause mortality measured from ICU admission for individuals with and without BSI, respectively. Demographical and ICU admission characteristics were explored as potential predictors of an ICU-acquired BSI.
Statistical analysis
Parametric data were presented as mean and standard deviation (SD), whilst non-parametric data were presented as median and interquartile range (q1-q3). Categorical data were presented as numbers (n) and percentages (%). Nominal data were analysed using the Chi-squared test, parametric data using the t-test, and non-parametric data using the Mann-Whitney U test. Univariable and multivariable logistic regressions were performed to explore the variables’ association with acquiring an ICU-acquired BSI and to adjust the 365-day mortality for significant confounders. Before the logistic regressions, variables with missing values were imputed by multiple imputations in SPSS using an iterative Markov chain Monte Carlo method [33]. The rate of missing data was generally low, ranging from 0–23%, and data were missing at random (S2 Table). Before entering the regression analysis, laboratory values were log-transformed (base 10) due to skewness. In line with the “rule of ten”, variables with at least ten events per variable and a p-value<0.2 in univariable analysis were entered in a single step in the multivariable logistic regressions after ruling out multicollinearity by testing for strong correlations with Spearmans- and Point-Biserial-test. [34]. The Hosmer-Lemeshow test was performed to evaluate the goodness of fit in the regression model, and a p-value>0.05 was considered a good fit [35]. Results of the logistic regressions are presented as unadjusted (OR) and adjusted Odds Ratio (aOR) with 95% Confidence Interval (CI), respectively.
The prediction was assessed by creating receiver operating characteristic (ROC) curves from the logistic regression models, and Areas Under the Receiver Operating Characteristics (AUROC) were calculated.
A sensitivity analysis was performed by comparing the results of the multivariable logistic regressions using the imputed and original data sets with missing variables included (S3 Table). Statistical significance was set to p < 0.05, and statistical analyses were conducted using IBM SPSS version 28.0.0.0.
Results
General patient characteristics
A total of 354 patients were included (Fig 1). The median age was 66 (57–73) years, 73% were male, and the median body mass index (BMI) was 30 (27–35) kg/m^2^. The median number of symptomatic days before ICU admission was 11 (8–15) days, the median Sequential Organ Failure Assessment (SOFA) score at ICU admission was 8 (6–10) points, and the median Simplified Acute Physiology Score 3 (SAPS 3) was 63 (54–71) points. On day 2 of IMV, 7% had mild ARDS, 60% moderate ARDS and 33% severe ARDS. Of the included patients, 98% received antibiotic therapy at some point during their ICU stay. Blood cultures were drawn from 99% of patients at least once during the hospital stay and from 78% during the ICU stay. The ICU mortality was 37%, hospital mortality was 44%, and 365-day mortality was 45% (Table 1).
Table 1: Baseline characteristics, clinical interventions and outcomes in 354 critically ill COVID-19 patients treated with invasive mechanical ventilation, stratified by an ICU-acquired bacterial bloodstream infection.
Flowchart of the 354 COVID-19 patients with ARDS included in the study.Abbreviations: ARDS: Acute respiratory distress syndrome, BSI: Bloodstream infection, ICU: Intensive care unit.
Bloodstream infections
In all, 12 (3%) patients had a community-acquired BSI, 8 (2%) patients had a hospital ward-acquired BSI, and 58 (17%) patients had an ICU-acquired BSI. Patients with an ICU-acquired BSI had higher BMI, 32 (28–38) kg/m^2^ versus 30 (27–35) kg/m^2^ (p = 0.028), than those who did not acquire BSI. (Table 1).
Fig 2 shows the most frequently identified pathogens causing ICU-acquired BSIs. Staphylococcus aureus (n = 23) was the most common pathogen, followed by coagulase-negative staphylococci (n = 12), Enterococcus faecalis (n = 8), and Enterococcus faecium (n = 8).
Bar chart illustrating the frequency of bacteria causing ICU-acquired bloodstream infections in 354 critically ill COVID-19 patients treated with invasive mechanical ventilation.Only bacterial species occurring in more than one patient are included in the chart. Abbreviation: ICU: Intensive care unit.
A multivariable logistic regression, including variables known at ICU admission, showed that higher BMI (aOR 1.06, 95% CI: 1.01–1.11, p = 0.014), diabetes mellitus with signs of organ complications (aOR 2.66, 95% CI: 1.33–5.29, p = 0.005) and the number of symptomatic days before ICU admission (aOR 1.04, 95% CI: 1.01–1.07, p = 0.008) were significantly associated with a BSI in the ICU (Table 2). The AUROC was 0.66 (95% CI: 0.58–0.74). Sensitivity analysis showed no significant differences from the regression analysis with imputed data.
Table 2: Univariable and multivariable logistic regression for the associations with ICU-acquired bacterial bloodstream infections in 354 critically ill COVID-19 patients treated with invasive mechanical ventilation.
Categorising the 58 patients with an ICU-acquired BSI showed that 79% had a late ICU-acquired BSI, 21% had an early ICU-acquired BSI, and one patient had both an early and late ICU-acquired BSI. The subgroup of patients with a late infection had significantly worse severity of ARDS (p = 0.039). See Table 3 for a detailed description of patient characteristics stratified by early versus late ICU-acquired BSI.
Table 3: Baseline characteristics, clinical interventions and outcomes of 58 critically ill COVID-19 patients treated with invasive mechanical ventilation with an ICU-acquired bacterial bloodstream infection, stratified by early (≤ 7 days after ICU admission) or late (≥ 7 days after ICU admission) infection.
In all, the 58 patients with an ICU-acquired BSI had a longer duration of IMV (20 days versus 9 days, p < 0.001), length-of-ICU stay (24 days versus 11 days, p < 0.001), and length-of-hospital stay (38 days versus 24 days, p < 0.001). Mortality rates were higher, with a 365-day mortality rate of 60% compared to 42% for those who did not acquire a BSI in the ICU (p = 0.01) (Table 1). The association between 365-day mortality and BSI remained after adjusting for age, BMI, Clinical Frailty Scale (CFS), CCI, SAPS 3 and PaO_2_/FiO_2_-ratio at day 2 of IMV in a multivariable regression analysis (aOR 3.21, 95% CI: 1.61–6.38, p < 0.001) (S4 Table).
Discussion
This study aimed to investigate the bacterial aetiology and clinical consequences of ICU-acquired BSIs among patients with critical COVID-19 who required IMV. Our main finding was that 17% of the included patients had an ICU-acquired BSI, the majority occurring more than one week after ICU admission. Staphylococcus aureus was the most common pathogen. An ICU-acquired BSI was independently associated with more than threefold odds of dying within 365 days as well as a longer duration of IMV and longer ICU-LOS.
The incidence of ICU-acquired BSIs in our study is in line with the findings in two large multicenter studies [18,36]. In contrast, two other European studies show that up to one-third of patients acquire a BSI in the ICU [10,37]. One of these studies, however, was a small single-centre study [37], making it less relevant to compare with our larger multi-centre study. We therefore suggest that the rate of ICU-acquired BSIs in this patient population can be estimated to range between 15%−30%.
This multicenter study was performed in a Nordic context. A Finnish study identified positive blood culture rates of close to 6% among COVID-19 patients treated in the ICU. In comparison, Swedish study identified positive blood cultures of approximately 7% among all patients treated in the hospital with COVID-19 [19,38]. These are numbers far below our rate of 17% of ICU-acquired BSIs. The Finnish ICU study, however, included only 132 patients, and it is unclear to what extent they received IMV. Our study included a larger sample, and all patients received IMV, which may explain the difference in incidence rate since critically ill patients receiving IMV are more susceptible to concomitant BSIs [23]. The definition of significant growth versus possible contamination may also differ from ours, possibly affecting the results [19].
Microbiological spectra
We identified Staphylococcus aureus as the dominating microbiological agent, a well-known cause of ICU-acquired BSIs [10,15,18]. Previous studies have found equally high or higher frequencies of species like Klebsiella pneumoniae, coagulase-negative staphylococci, Enterococcus species. Escherichia coli and Pseudomonas aeruginosa [15,18,36]. Studies investigating ICU-acquired BSIs vary regarding the cause of ICU admission, treatments and interventions during ICU stay, as well as regional differences in microbiological spectra, antimicrobial resistance patterns and deaths associated with antimicrobial resistance. Hence, it is difficult to draw any conclusions on the dominating pathogens in other settings [10,15,18,21,22,36]. Of note, the second to fourth most common causative agents behind BSI in our study were organisms frequently harboring resistance mechanisms conferring reduced susceptibility or resistance to third generation cephalosporins, the first-line empiric antibiotic used at the participating ICUs [39,40]. With this in mind, we consider it essential to emphasize that this study provides valuable insights into the Nordic context in general and the Swedish context in particular.
Early versus late ICU-acquired bloodstream infections
Almost 80% of the ICU-acquired BSIs in the present study occurred late (more than 7 days) after ICU admission, which aligns with previous findings in COVID-19 patients [23]. Late infections in the ICU are not only specific to patients with COVID-19; the large EUROBACT-2 study showed that late ICU-acquired BSIs were more common among general ICU patients [29].
Outcomes and risk factors
An ICU-acquired BSI was associated with a more than twice as long duration of IMV and ICU-LOS and close to twice as long hospital-LOS compared to those not acquiring a BSI, which is similar to what has previously been reported [10,11,37]. It is worth highlighting that these differences were seen when comparing two groups of patients with no significant differences in variables like C-reactive protein (CRP), SOFA score and SAPS3 score at ICU admission as well as severity of ARDS at day 2 of intubation. With the granularity of our data we cannot conclude whether a secondary BSI in our study significantly increased the hospital- and ICU-LOS or if the contrary is true, i.e., that the prolonged hospital- and ICU-LOS increased the risk of developing a BSI, which has been shown in previous studies [23,29,36,41]. However, it was out of the scope of the current study to further analyse possible causal relationships.
In the adjusted analyses, including variables at ICU admission, we found that a higher BMI, diabetes mellitus with organ complications, and the number of symptomatic days before ICU admission were risk factors associated with an ICU-acquired BSI. Obesity has, in line with our previous findings, been identified as a risk factor for BSIs in critically ill COVID-19 patients [23]. Diabetes mellitus has also been associated with secondary infections in critically ill COVID-19 patients [37]. However, considering the limited predictive ability of our regression model (AUROC = 0.66), it remains difficult to predict which patients will have an ICU-acquired BSI using the chosen pre-ICU admission risk factors [42].
The study aimed to investigate patient-specific risk factors associated with an ICU-acquired BSI. We acknowledge that there exist other potential risk factors such as the use of central venous lines and external risk factors like to what extent clinical staff adhered to infection control measures like basic hand hygiene routines. Exploring those non-patient-specific risk factors was beyond the scope of the current study, but they would be interesting to further investigate and explore in future studies.
In the present study, an ICU-acquired BSI was associated with a more than threefold increase in the odds of dying within 365 days of ICU admission, even when adjusting for confounders. This is in line with previous studies where an ICU-acquired BSI has been associated with a twofold or more increase in the odds of dying among critically ill COVID-19 patients [43–45]. Importantly, although we found a significant association between mortality and ICU-acquired BSI, the results must be interpreted with caution. We cannot rule out that some patients acquiring a BSI during the ICU stay were more severely ill, with an expected increased mortality rate even without a secondary BSI.
Strengths and limitations
This study’s major strength is the large population of prospectively included consecutive, critically ill COVID-19 patients receiving IMV from multiple centres over 12 months. The rate of missed inclusions and patients excluded due to not receiving consent was very low. Furthermore, the rate of missing data was low, generating more robust results.
Our study’s limitations include its observational design, which does not allow for causal conclusions but merely associations. The protocol did not include systematic blood cultures before antibiotic treatment in the ICU. Yet, the routinely obtained blood culture rate was high, minimising the risk of misclassified BSIs. Furthermore, the study design did not allow for exploring temporal associations between ICU-LOS and BSI. No adjustments for multiple testing were made, and the results should only be considered hypothesis-generating due to the exploratory design. Additionally, the depth and details of the data regarding information about the administration of antibiotics could have been more detailed than what was collected for this study. For example, administration of antibiotic agents could have been collected as a continuous variable, allowing for temporal comparisons. Hence, we consider this a potential limiting factor in this study.
Conclusion
Secondary ICU-acquired BSIs are common, occurring in 17% of critically ill COVID-19 patients receiving IMV. Most infections occurred more than one week after ICU admission, and the most common pathogen was Staphylococcus aureus. An ICU-acquired BSI was associated with more than threefold odds of dying within 365 days as well as a longer duration of IMV and longer ICU-LOS. We found several factors associated with ICU-acquired BSIs at ICU admission. However, their ability to predict BSIs was poor.
Supporting information
S1 TableBacteria occurring in blood cultures in the study, stratified by clinical significance.(DOCX)
S2 TableMissing data.Data presented as numbers (percentages). Abbreviations: Percentages: (%), ARDS: Acute respiratory distress syndrome, BMI: Body mass index, BSI: Bacterial bloodstream infection, CCI: Charlson Comorbidity Index, CRP: C-reactive protein, ICU: Intensive care unit, IL-6: Interleukin-6, IMV: Invasive mechanical ventilation, SAPS 3: Simplified acute physiology score 3, SOFA: Sequential organ failure assessment, IQR: Interquartile range, PaO_2_/FiO_2_: Partial pressure of arterial oxygen to fraction of inspired oxygen, SAPS 3: Simplified acute physiology score 3, SOFA: Sequential organ failure assessment.(DOCX)
S3 TableSensitivity analysis comparing the results of the multivariable logistic regression for the associations with ICU-acquired bacterial bloodstream infection between the original data set with missing variables and the imputed data set.Abbreviations: aOR: Adjusted Odds Ratio, BSI: Bacterial bloodstream infection, BMI: Body mass index, CI: Confidence Interval, ICU: Intensive care unit.(DOCX)
S4 TableUnivariable and multivariable logistic regressions for the associations with 365-day mortality rate in 354 critically ill COVID-19 patients treated with invasive mechanical ventilation.Supplementary Table 4 shows the univariable logistic regression result, including acquiring an ICU-acquired BSI and variables known at ICU admission and their association with 365-day mortality. Data are presented as p-value, Odds Ratio and 95% Confidence Interval. P-values < 0.05 were considered significant. Covariates included in the multivariable logistic regression were age, BMI, CCI, CFS, duration of symptoms before ICU admission, history of smoking (ever smoker), ICU-acquired BSI, medication with immunosuppressive agents before hospitalisation, PaO_2_/FiO_2_ ratio at day 2 of intubation and SAPS 3. Abbreviations: aOR: Adjusted Odds Ratio, AUROC: Area Under the Receiver Operating Characteristics BMI: Body mass index, BSI: Bloodstream infection, CCI: Charlson Comorbidity Index, CI: Confidence Interval, ICU: Intensive care unit, OR: Odds Ratio, PaO_2_/FiO_2_: Partial pressure of arterial oxygen to fraction of inspired oxygen, SAPS 3: Simplified Acute Physiology Score 3 and SOFA: Sequential Organ Failure Assessment.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-n Co V and naming it SARS-Co V-2. Nat Microbiol. 2020;5(4):536–44. doi: 10.1038/s 41564-020-0695-z 32123347 PMC 7095448 · doi ↗ · pubmed ↗
- 2Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708–20.32109013 10.1056/NEJ Moa 2002032 PMC 7092819 · doi ↗ · pubmed ↗
- 3Glenet M, Lebreil A-L, Heng L, N’Guyen Y, Meyer I, Andreoletti L. Asymptomatic COVID-19 Adult Outpatients identified as Significant Viable SARS-Co V-2 Shedders. Sci Rep. 2021;11(1):20615. doi: 10.1038/s 41598-021-00142-8 34663858 PMC 8523690 · doi ↗ · pubmed ↗
- 4Grasselli G, Tonetti T, Protti A, Langer T, Girardis M, Bellani G, et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: a multicentre prospective observational study. Lancet Respir Med. 2020;8(12):1201–8. doi: 10.1016/S 2213-2600(20)30370-2 32861276 PMC 7834127 · doi ↗ · pubmed ↗
- 5Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-Co V-2 Admitted to IC Us of the Lombardy Region, Italy. JAMA. 2020;323(16):1574–81. doi: 10.1001/jama.2020.5394 32250385 PMC 7136855 · doi ↗ · pubmed ↗
- 6Tenforde MW, Self WH, Adams K, Gaglani M, Ginde AA, Mc Neal T. Association Between m RNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA. 2021;326(20):2043–54.34734975 10.1001/jama.2021.19499 PMC 8569602 · doi ↗ · pubmed ↗
- 7Wright BJ, Tideman S, Diaz GA, French T, Parsons GT, Robicsek A. Comparative vaccine effectiveness against severe COVID-19 over time in US hospital administrative data: a case-control study. Lancet Respir Med. 2022;10(6):557–65. doi: 10.1016/S 2213-2600(22)00042-X 35227415 PMC 8881000 · doi ↗ · pubmed ↗
- 8World Health Organization. WHO Coronavirus (COVID-19) dashboard> Cases [Dashboard]. World Health Organization; 2024 [cited 2024 2024-09-16]. Available from: https://data.who.int/dashboards/covid 19/cases