Tachycardia Termination Without Global Propagation: Is the Pacing Site In or Out?
Ozcan Ozeke, Dursun Aras, Serkan Topaloglu

TL;DR
This paper discusses how pacing the heart without full electrical spread can help identify key areas in tachycardia circuits.
Contribution
It introduces a new criterion for identifying re-entrant circuits in tachycardia using non-global pacing capture.
Findings
Non-global capture pacing can identify critical parts of tachycardia circuits.
This method works even without concealed entrainment confirmation.
Extrastimuli can be used intentionally to demonstrate this phenomenon.
Abstract
Ventricular tachycardia termination by pacing with non-global capture is a specific criterion for identifying a critical component of the re-entrant circuit, regardless of whether concealed entrainment can be demonstrated at that site. It is usually observed almost by chance, but it can also be intentionally demonstrated by introducing a single extrastimulus during tachycardia.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
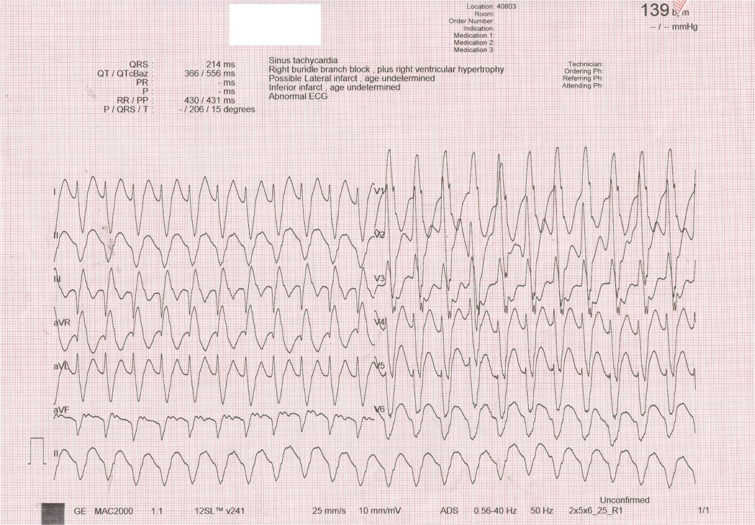 Figure 1
Figure 1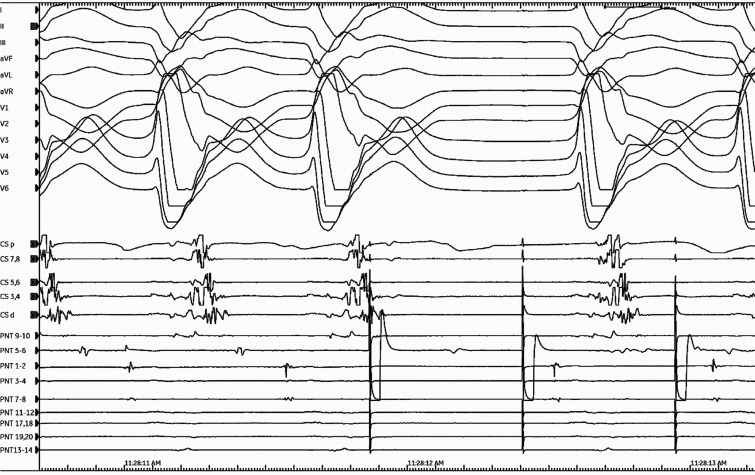 Figure 2
Figure 2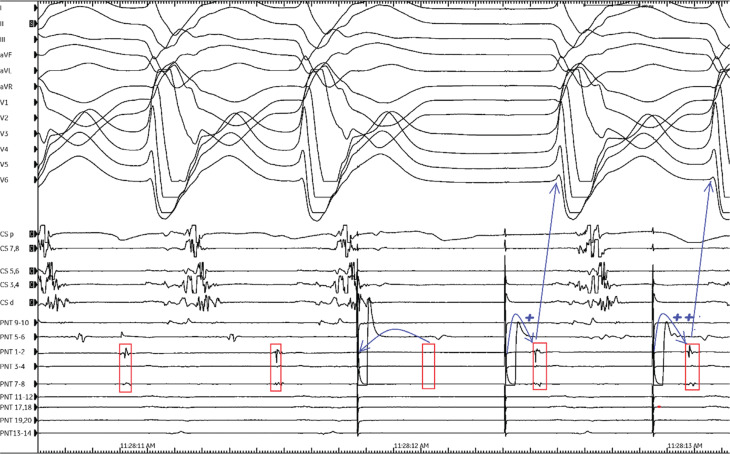 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiac Arrhythmias and Treatments · Cardiac electrophysiology and arrhythmias
Case presentation
A 72-year-old man was referred for catheter ablation of incessant ventricular tachycardia (VT). He had experienced a myocardial infarction 12 years earlier and had previously undergone coronary bypass and mitral valve replacement surgery. An electrocardiogram revealed sustained monomorphic VT characterized by a QRS morphology with a right bundle branch block pattern and a superior axis; the tachycardia cycle length was 430 ms (Figure 1). The clinical VT was spontaneously induced and was hemodynamically tolerated and mapped (Video 1). During the tachycardia, a series of single ventricular extrastimuli was delivered from the putative diastolic potential region. Based on the response to ventricular entrainment attempts (Figure 2), we questioned whether the pacing site was in or out of the re-entrant circuit.
A 12-lead electrocardiogram showing the clinical ventricular tachycardia.
Termination without global propagation by the first stimulus of a pacing train from the PentaRay® catheter (PNT) 5-6 is seen.
Discussion
In the setting of structural heart disease, VT is typically associated with a re-entrant mechanism.^1–4^ Successful catheter ablation of VT depends on identifying the critical tissues that sustain the arrhythmia.^5^ Four mapping techniques consistently play a role in successful VT ablation: activation mapping, entrainment mapping, pace mapping, and substrate mapping. Entrainment mapping, or continuous resetting of a re-entrant tachycardia, provides a powerful tool for distinguishing between focal and re-entrant VT, as well as identifying critical circuit components such as the entrance, critical isthmus (CI), and exit sites.^1,6–12^ The detection of the ideal site for ablation within a central CI is a mid-diastolic potential during VT that exhibits concealed fusion with a post-pacing interval equal to the tachycardia cycle length.^13^ Thus, entrainment mapping helps to identify the CI, but it is not always feasible and, in some cases, terminates VT,^14^ as occurred in the current tracing. Indeed, local capture of the CI without global ventricular capture (non-global capture [NGC]) can terminate VT by resulting in a bidirectional block (orthodromic or non-orthodromic capture) within the CI.^15–18^ However, termination might also occur due to a rate-dependent block in the slow-conduction zone during pacing,^4,19,20^ and catheter contact at a critical endocardial site can interrupt postinfarction VT.^21^ The stimulus–QRS (S–QRS) interval was significantly shorter at sites where mechanical trauma affected the re-entrant circuit compared with sites having concealed entrainment.^21^ Therefore, if an arrhythmia terminates during overdrive pacing but several stimuli that should capture do not, then the termination might have been spontaneous or caused by mechanical trauma; such events do not carry the same implications as termination by NGC. Furthermore, all these pacing attempts rely on consistent capture of tissue with each stimulus. While “capture” refers to whether the pacing stimulus depolarizes the local myocardium, “global capture” means that the entire QRS complex (ie, the full ventricular myocardium) is activated by the pacing stimulus and the morphology differs from the VT QRS. On the contrary, NGC (also termed “concealed entrainment”) means that only a part of the VT circuit or surrounding myocardium is depolarized without altering the overall QRS morphology during VT, supporting CI involvement.^15,18^ VT termination by pacing with NGC is a specific criterion for identifying a critical component of the re-entrant circuit, regardless of whether concealed entrainment can be demonstrated at that site.^15,16^ It is usually observed almost by chance, but it can also be intentionally demonstrated by introducing a single extrastimulus during tachycardia.
In the current tracing, VT was terminated with NGC by a single extrastimulus at this site; however, concealed entrainment could not be assessed due to the termination of the VT. In general, amplifier saturation from pacing typically obscures the local electrogram (EGM) on the pacing electrodes at the time of pacing, as seen in Figure 2 (5-6 with PentaRay^®^ [JNJ Medtech, New Brunswick, NJ, USA]); thus, a careful examination of adjacent electrode recordings (PentaRay^®^ 1-2 and 7-8, Figure 3) is important to confirm evidence of local capture. Examination of the adjacent electrode recording (red rectangles in Figure 3) confirms that the similarly timed component was captured just downstream of the stimulus, as it is no longer observed at the expected interval (red blank rectangle in Figure 3 indicates absent EGM).^14^
Illustration corresponding to Figure 2. Local electrograms on PentaRay® 1-2 and 7-8 (red rectangles) confirm stimulus-induced capture (blank red rectangle). Conduction delay is evident by gradual stimulus–QRS prolongation after tachycardia termination by non-global capture (blue plus signs).
Following termination of VT, stimuli directly captured the local CI myocardium, probably including the exit site, as confirmed by the QRS morphology matching that of the VT.^19^ The S–QRS interval is a well-known indicator of the conduction time from the pacing site to the exit VT.^22^ If it is prolonged and furthermore reveals a conduction delay in the isthmus after VT termination by NGC, these support the NGC location as a critical position in the re-entrant circuit.^15^ In the current tracing, there was also evidence of a conduction delay (Figure 3, note the blue “plus sign”), with gradual prolongation of the S–QRS interval following tachycardia termination by NGC. Combining all these observations, ablation at this site rendered the clinical VT non-inducible.
Supporting information
Supplementary Video 1:Activation mapping shows the re-entry circuit at the inferior left ventricle.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Waldo AL Henthorn RW Use of transient entrainment during ventricular tachycardia to localize a critical area in the reentry circuit for ablation Pacing Clin Electrophysiol 1989121 Pt 223124410.1111/j.1540-8159.1989.tb 02652.x 2466258 · doi ↗ · pubmed ↗
- 2Stevenson WG Sager PT Friedman PL Entrainment techniques for mapping atrial and ventricular tachycardias J Cardiovasc Electrophysiol 19956320121610.1111/j.1540-8167.1995.tb 00771.x 7620645 · doi ↗ · pubmed ↗
- 3Stevenson WG Sager PT Natterson PD Saxon LA Middlekauff HR Wiener I Relation of pace mapping QRS configuration and conduction delay to ventricular tachycardia reentry circuits in human infarct scars J Am Coll Cardiol 199526248148810.1016/0735-1097(95)80026-d 7608454 · doi ↗ · pubmed ↗
- 4Stevenson WG Nademanee K Weiss JN Programmed electrical stimulation at potential ventricular reentry circuit sites. Comparison of observations in humans with predictions from computer simulations Circulation 198980479380610.1161/01.cir.80.4.7932791244 · doi ↗ · pubmed ↗
- 5Miller JM Szwed JM Chakka MN Postextrastimulus delay of ventricular tachycardia return cycle: indicator of a good ablation site Heart Rhythm 20063787087110.1016/j.hrthm.2005.12.02516818226 · doi ↗ · pubmed ↗
- 6Ozcan Cetin EH Ozeke O Kara M Electrophysiological mechanism of wide QRS complex tachycardia revealed by an unexpected intervention J Cardiovasc Electrophysiol Published online August 19202510.1111/jce.7006540827678 · doi ↗ · pubmed ↗
- 7Ozcan Cetin EH Korkmaz A Kara M Multiple wide QRS tachycardias in the same individual with ischemic cardiomyopathy J Cardiovasc Electrophysiol 202334124124510.1111/jce.1577636511469 · doi ↗ · pubmed ↗
- 8Kara M Korkmaz A Ozeke O Wide QRS tachycardia with alternating QRS morphologies: what is the mechanism?Pacing Clin Electrophysiol 202043114614810.1111/pace.1384731774186 · doi ↗ · pubmed ↗