Just do the ECV, Just do it - This, I call it a Miracle:” Understanding External Cephalic Version Practices at the Largest Teaching Hospital in Ghana
Dhanalakshmi Thiyagarajan, Yana Astter-Sompel, Thelma Quarshie, Jessica McCoy, Mackenzie Woock, Cheryl A. Moyer, Alim Swarray-Deen, Samuel A. Oppong, Emma R. Lawrence

TL;DR
This study explores how external cephalic version is practiced at a major hospital in Ghana, revealing gaps in counseling and training that could help reduce unnecessary cesarean deliveries.
Contribution
The study provides insights into ECV practices in a low-resource setting and identifies barriers to its adoption, offering actionable recommendations for training and counseling improvements.
Findings
Only 45.7% of eligible patients were offered ECV, and 37.0% underwent the procedure.
Barriers included previous cesarean delivery history and limited training/resources among clinicians.
Patients and clinicians viewed ECV positively but lacked understanding of the procedure and its risks.
Abstract
External cephalic version (ECV) is a proven, low-risk, low-resource, and cost-effective procedure, when performed by a skilled healthcare professional, to reduce cesarean delivery (CD) rates for malpresented fetuses. Information regarding ECV practices in low- and middle-income countries is limited. We sought to understand and evaluate malpresentation counseling, decision-making, and ECV practices from the perspective of clinicians and patients at the largest referral teaching hospital in Ghana. We conducted a prospective, multi-modal cohort study of obstetrics patients who were eligible for ECV at Korle Bu Teaching Hospital in Accra, Ghana between July 1 and December 31, 2024. We enrolled pregnant patients who were ≥ 36 weeks gestation diagnosed with malpresentation. After enrollment, the research team directly observed the patients’ antenatal care visits to collect data on the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
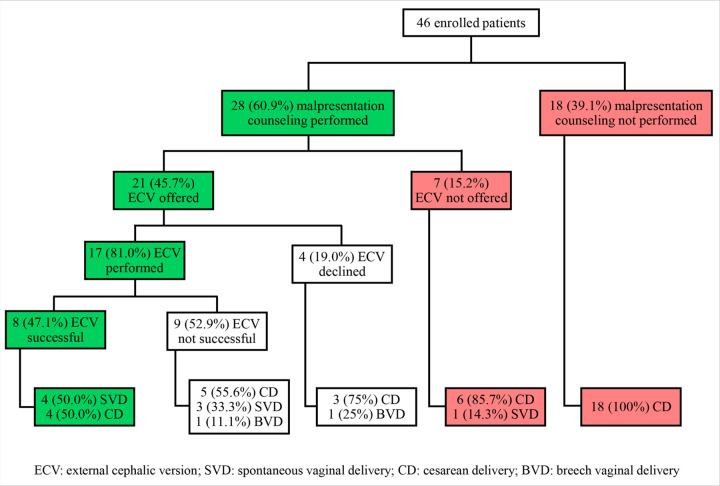 Figure 1
Figure 1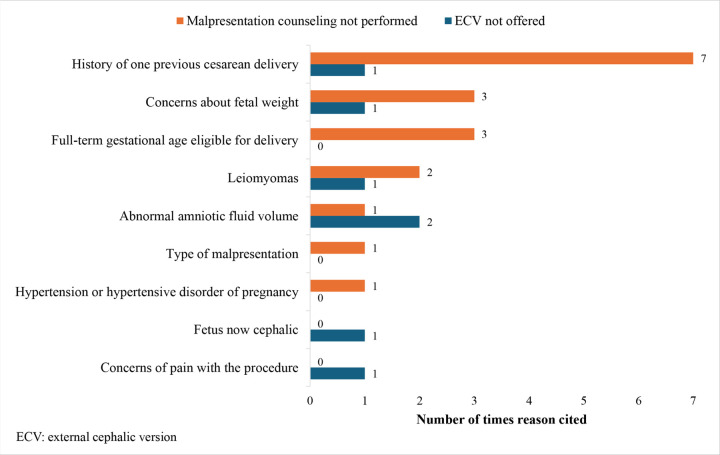 Figure 2
Figure 2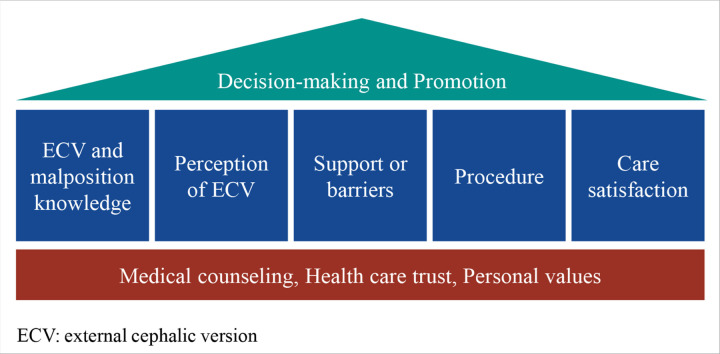 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and Perinatal Health Interventions · Global Maternal and Child Health · Reproductive Health and Contraception
Background
Evidence shows that cesarean delivery (CD) rates above 19% do not decrease maternal morbidity and mortality.^1^ When not medically necessary, CD pose a greater risk to maternal and neonatal health compared to vaginal delivery, especially in low- and middle-income countries (LMICs), where perioperative resources may be limited.^1–3^ In 2020, over 95% of maternal deaths occurred in LMICs, with the majority being preventable. This highlights the urgent need to reassess the current use of CDs in LMICs in reducing maternal morbidity and mortality.^4^ In 2022, the national CD rate in Ghana was 21%,^5^ while 2016 data indicate the CD rate at Korle Bu Teaching Hospital (KBTH), a tertiary referral hospital where the current research was conducted, was 46.9%.^6^
The third most common indication for primary CD is malpresentation, when the fetus is not in a head down position, which affects approximately 4% of term pregnancies.^1,2^ The American College of Obstetricians and Gynecologists and the Royal College of Obstetricians and Gynecologists recommend that external cephalic version (ECV) be attempted for cases of malpresentation to avoid CD and enable a trial of vaginal delivery.^2,3^ ECV is a procedure in which a skilled clinician applies external pressure to the abdomen of a pregnant person with a malpresented fetus to manually rotate the fetus to a cephalic, head-down presentation that facilitates vaginal delivery.^7^
Existing research helps shed light on patient attitudes toward ECV. In one study, patients in the UK report viewing successful ECV as a means to a “natural” birth, framing vaginal delivery as an “achievement” with faster recovery and CD as a last resort for management, specifically for first-time labor.^10^ However, other patients view ECV as an unnatural manipulation of their fetus and have significant concerns about pain levels during the procedure.^10^ One study from Australia reported patient barriers to ECV to include receiving very little or no information from a clinician on the procedure, concerns about fetal safety, and the fact that a vaginal delivery was not guaranteed after successful ECV.^11^ In another study, some patients reported learning more about ECV from family, friends, and the print media than from a clinician, indicating a possible gap in quality information or an overestimation of risks.^12^ They also found that patients generally responded favorably to “de-mything” negative assumptions about ECV, noting the importance of timing, manner, and depth of information given during malpresentation counseling as important predictors of women’s anxieties surrounding ECVs.^12^ From a clinician’s perspective, several barriers to providing quality ECV counseling exist, including lacking confidence in the skills of the clinician performing the ECV, disagreement among clinicians on contraindications, and a perceived inability to convince patients who have previously decided on planned CD to consider alternative options, as identified by research in the Netherlands.^13^
While these studies shed light on malpresentation counseling, decision-making, and ECV practices in high-income countries, there is very little current information regarding ECV practices and decision-making among patients and clinicians in LMICs. While studies suggest an overwhelming desire for vaginal delivery over CD among women in LMICs,^14^ data from 2009 shows that only 21–52% of healthcare professionals in sub-Saharan Africa perform ECVs.^9^
The aim of the current study was to evaluate the current state of malpresentation counseling and decision-making and ECV practices in Ghana from the perspective of clinicians and patients. Optimizing management of malpresentation and by extension, ECV, into common practice in sub-Saharan Africa has the potential to reduce avoidable CD and its associated morbidity and mortality.
Methods
We conducted a multi-modal study at the Korle Bu Teaching Hospital (KBTH), in Accra, Ghana. The quantitative component was a prospective, cohort study of obstetrics patients who were eligible for ECV between July 1 and December 31, 2024. In the qualitative component of the study, we conducted semi-structured interviews of clinicians and postpartum patients. KBTH, located in the capital city of Accra, is the largest referral teaching hospital in Ghana and the third largest in sub-Saharan Africa. The 6-floor maternity unit has 275 inpatient beds and performs approximately 8,000 deliveries annually. While updated data is limited, 9% of CDs at KBTH in 2010–2011 were due to malpresentation.^4^ Patients were included if they were receiving antenatal care at KBTH; able to speak English, Twi, or Ga (the two most popular local dialects in the area); and diagnosed with malpresentation at 36 weeks’ gestation or greater. Patients were excluded if they were younger than age 18, referred from another facility for delivery, or had an absolute clinical contraindication to trial of vaginal delivery (which by hospital policy includes a history of two previous CDs).
Institutional review board approval was obtained from KBTH (KBTH-STC/IRB/00044/2024). The study aims were presented to the Department of Obstetrics and Gynecology during their department meeting. Recruitment was completed by trained research assistants at two key hospital locations: the Fetal Assessment Center, where all obstetric ultrasounds are performed, and the outpatient department, where antepartum patients receive outpatient care. Clinicians and nurses attending to these patients notified the research team of potential participants. The research team assessed eligibility by reviewing the patient’s pregnancy care booklet, which is the medical record completed by the patient’s clinician team. If eligible, the study protocol was thoroughly explained to the patient in the language of their choice (English, Twi, or Ga). If the patient was interested, they provided written informed consent to participate. The research team reviewed hospital records, including the ECV and delivery record books, on a weekly basis to ensure no patients were missed in the recruitment process.
After enrollment, the research team directly observed each patient’s antenatal care visits to collect data on the counseling related to their malpresentation diagnosis and ECV procedure if performed. Delivery information was collected postpartum via the patient’s pregnancy care booklet. Malpresentation counseling was classified as “performed” if the options of ECV and CD were discussed with the patient; vaginal breech delivery discussions were not included. The counseling method and information given was performed by the patients’ clinician per their standard clinical practices; the research team did not intervene. Patients were able to unenroll at any time and the research team did not participate in the patients’ care.
In the postpartum period, all enrolled patients were requested to participate in a semi-structured interview using an interview guide developed by the authors based on the Theoretical Framework of Acceptability to understand their perspectives and decision-making around accepting, declining, or not being offered ECV (see Additional files 1 and 2).^5^ The interviews were conducted privately in person in the language of their choice (English, Twi, or Ga). Enrolled patients’ clinicians, including trainees, were also requested to participate in a semi-structured interview using an interview guide developed by the authors based on the Theoretical Framework of Acceptability to understand their perspectives and decision-making around offering or not offering ECV (see Additional file 3).^5^ Clinicians were only invited to interview once, regarding their first patient enrolled in the study; information regarding any additional patients who were enrolled was not addressed. Interviews were conducted privately in person in English. All interviews were audio-recorded. Recordings were translated and back-translated from Twi or Ga to English (if necessary) to ensure consistency across languages and transcribed verbatim. Recordings in English were transcribed verbatim with GoTranscript (Lewes, DE, USA). The final numbers of interviews for both patients and clinicians were determined by thematic saturation of the data and/or completion of the recruitment process.
Quantitative data was collected in Research Electronic Data Capture (REDCap) and analyzed with Stata v18 (College Station, TX, USA). For data analysis, age (in years) was re-coded as 18–34 and 35 or greater; relationship status was re-coded as relationship or single; highest completed education was re-oded as junior high school or less, senior high school, or tertiary; partner highest completed education was re-coded as senior high school or less or tertiary given low sample size; and the differences between the ECV-performing clinician and the counseling clinician were manually compared and coded as yes or no. No patient’s medical history was complicated by gestational diabetes in a previous pregnancy, seizure disorder, respiratory diseases other than asthma, mental illness, heart disease/failure, tuberculosis, or smoking; therefore, these conditions were not included in the analysis. We performed descriptive and inferential statistics including cross-tabulation with Chi-square analysis or Fisher’s exact test for categorical variables and independent samples t-test or analysis of variance for continuous variables. Statistical significance was defined at p < 0.05.
We imported the patients’ qualitative data into Dedoose 10.0.35 (Manhattan Beach, CA, USA) for coding. Two research team members independently reviewed the transcripts to develop parent and child codes and iteratively developed a finalized codebook, which was reviewed by the remaining research team members for completion. Two research team members independently coded each transcript in Dedoose using the finalized codebook. Coding discrepancies were discussed and resolved on a weekly basis to ensure consistency throughout the coding process. We conducted thematic analysis using the thematic networks technique to understand patient decision-making around malpresentation and ECV.^6^ This process was replicated for the clinicians’ qualitative data.
Results
During the study period, 57 patients were identified at 36 weeks’ gestation as eligible for ECV. Six (10.5%) patients declined recruitment. Of the 51 (89.5%) patients who enrolled, five (9.8%) were lost to follow-up: three were no longer interested in being in the study, one patent was no longer interested in pursuing care at KBTH, and one provided an incorrect phone number for follow-up. A total of 46 (80.7%) eligible patients ultimately enrolled and were followed to delivery (Table 1). All patients had national health insurance. Three patients, who had a history of one previous CD, had this first CD due to malpresentation.
Out of the 46 enrolled patients, ECV was discussed with 28 (60.9%) and offered to 21 (45.7%). Four (19.0%) patients who were offered ECV declined. Eight (47.1%) of the 17 ECVs performed were successful and none reverted to malpresentation before delivery (Fig. 1).
Figure 2 demonstrates the various reasons clinicians stated for recommending CD over ECV during the counseling session, as observed by the research team. Upon individual review of the ultrasound findings by the research team, no fetuses were identified as growth restricted or having macrosomia to the extent CD was required. Additionally, there were no cases where fibroids were considered a contraindication to a trial of vaginal delivery.
When comparing reasons for malpresentation counseling not being performed, history of one previous CD was a significant factor (Table 2). Of the 46 enrolled patients, eight (17.4%) had a history of one previous CD; however, only one (12.5%) received malpresentation counseling. Malpresentation-related history and pregnancy complications related to current or previous fetal anatomical abnormality, diabetes mellitus or gestational diabetes, sickle cell disease, HIV, asthma, Rh negative, postpartum hemorrhage in previous pregnancy, and fetal or neonatal demise in previous pregnancy were too small for comparisons.
Of the 46 enrolled patients, 35 (76.1%) completed an interview regarding their malpresentation and ECV counseling, ECV procedure if performed, and postpartum experience; of these, 16 (45.7%) were never offered ECV and proceeded to deliver by CD. The other 19 patients (54.3%) were offered ECV: 15 (78.9%) elected to pursue ECV, resulting in eight (53.3%) spontaneous vaginal deliveries and seven (46.7%) CDs; and four (21.1%) decided against pursuing ECV, resulting in one (25.0%) vaginal breech delivery and three (75.0%) CDs. Twenty of these patients’ clinicians completed an interview regarding their malpresentation and ECV counseling and ECV procedure if performed: 10 (50.0%) offered ECV and 10 (50.0%) did not offer ECV to these patients (Table 3).
Regarding decision-making around whether to offer and/or pursue ECV, patients refrained from pursuing ECV if they had gaps in understanding the procedure and its complications but were more likely to pursue it when supported by partners, friends, and clinicians. Although, clinicians demonstrated appropriate knowledge to counsel patients regarding the procedure and its complications. Both patients and clinicians were motivated by their desire to avoid the financial cost, long recovery time, and future complications of undergoing a CD. Overall, patients and clinicians had a positive perception of ECV and would endorse it regardless of whether the procedure resulted in a vaginal delivery or not (Table 4).
Despite clinicians valuing ECV, they highlighted barriers preventing them from offering ECV to more patients, including patients with a history of one prior CD, hospital resource barriers to performing ECV, and limited training opportunities to learn ECV procedural skills (Table 5).
Clinicians and patients were comfortable with midwives performing ECV if they were appropriately trained to do so.
Overall, medical counseling, trust in the health care system and professional, and personal values were fundamental motivators to patients as they began to make their decision on whether to have ECV or not.
Knowledge of ECV and malpresentation, perception of ECV, support or barriers experienced, experience of the ECV procedure, and care satisfaction played influential roles in a patient’s final decision to pursue and promote ECV to others (Fig. 3).
Discussion
Among 46 enrolled patients who were eligible for ECV, only 21 (45.7%) patients were offered the procedure. Though a patient having a history of one previous CD was a significant factor in clinicians not offering ECV, evidence demonstrates that this does not increase the risk of ECV complications, nor does it decrease the success rate of an ECV. It is generally recommended to offer ECV to patients who are otherwise eligible for trial of labor after cesarean.^2,3,8,9^ Though other concerns cited by clinicians such as fetal weight, gestational age, leiomyomas, abnormal amniotic fluid volume, and type of malpresentation may factor into the success of ECV, there is conflicting data regarding the predictive value of these factors; therefore, decisions to not offer ECV should not be based solely on these factors.^2,3,10–17^ While caution must be used with hypertensive patients to ensure stability can be achieved while awaiting a vaginal delivery, hypertension itself has not been noted as a contraindication to ECV.^2,3^ Additionally, although ECV can be a painful procedure—information that should be included in patient counseling—most patients can tolerate this procedure and can be offered ECV.^2,18^ Finally, while limited resources in the hospital for fetal monitoring was cited as a factor for not offering ECV, and although the non-stress test is the gold standard for monitoring, alternatives such as ultrasound may be used to continue to offer this overall low-resource procedure.^2,3^
The biggest contributing factor identified by patients for being concerned and/or not pursuing ECV was a gap in understanding the procedure and its potential complications. This is aligned with other studies conducted in Australia, England, and the United States.^19–21^ Similar to our finding that patients are more likely to make their decision about pursuing ECV with family, friends, and clinicians, studies among patients in Nigeria, England, and Australia have demonstrated the same.^19,20,22^ Conversely, another study in Austria demonstrated that family and friends were a reason patients decided against pursuing ECV.^23^ Interestingly, in our study, some patients felt comfortable
and motivated to make their own decision without partner support and/or input, which does not align with other studies performed in Ghana which highlighted the strong partners role in health care decision-making.^24,25^ In studies completed in the United States and England, knowledge of the success rate of the ECV procedure played a large role in patient decision-making, which we did not find in our study.^20,21^
In our study, patients and clinicians valued ECV as a way to prevent CD, which aligns with patients and clinicians in England, the United States, and other studies among Ghanaians.^20,21,26^ While patients in our study desired to promote ECV to others even if it was not successful and resulted in a CD, this is unique compared to studies of patients in Austria and Australia.^19,23^
There are opportunities to improve clinician knowledge on evidence-based indications for offering ECV to encourage more patients who can benet from this procedure, as well as to implement training on counseling practices to discuss the risks, benefits, and alternatives to ECV that resonate with patients and aid in their decision-making. There may be a bene t to encourage the involvement of patients’ families and other support persons throughout the counseling and decision-making process. Revising hospital guidelines for evidence-supported fetal monitoring during and after the procedure may reduce the burden on hospital resources that currently limit ECV from being offered. Additionally, these findings demonstrate an opportunity to train clinicians, such as in a simulation-based curriculum, to improve the knowledge, confidence, and sustainability of ECV practices.^27^ Importantly, ECV training for midwives may be beneficial to ensure patients have greater access to ECV services.
Strengths and limitations
To our knowledge this is the first study to explore and evaluate ECV practices in Ghana. However, this study was limited to KBTH, which as the largest teaching hospital is more likely to be performing evidence-based practices than other hospitals. Additionally, the Department of Obstetrics and Gynecology was informed of this study and research assistants were present at every counseling visit or ECV procedure, which may have biased counseling patterns and/or interview responses for patients whose pregnancies were complicated by malpresentation given that it was known we were evaluating malpresentation practices. Patients who declined to participate or were lost to follow-up may have had other experiences.
Conclusions
With increasing CD rates in sub-Saharan Africa, preventing CDs is paramount to reducing maternal and neonatal morbidity and mortality, aligned with the United Nations’ Sustainable Development Goal three.^4,28,29^ ECV is a proven, low-risk, low-resource, and cost-effective procedure, when performed by a skilled clinician, to reduce CD rates for malpresented fetuses.^2,30–32^ This study demonstrates that there is an opportunity to improve counseling and utilize evidence-based indications to offer ECV to patients whose pregnancies are complicated by fetal malpresentation. There is also an important opportunity to ensure clinicians, and potentially midwives, are trained to perform ECV. Addressing these opportunities successfully could improve the numbers of health care professionals who practice safe and effective ECV in sub-Saharan Africa and potentially decrease rates of avoidable CD and their associated morbidity and mortality.^2,3^
Supplementary Material
This is a list of supplementary fi les associated with this preprint. Click to download.
• Additionalfile1.docx
• Additionalfile2.docx
• Additionalfile3.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American College of Obstetricians and Gynecologists (College), Society for Maternal-Fetal Medicine, Caughey AB, Cahill AG, Guise JM, Rouse DJ. Safe prevention of the primary cesarean delivery. Am J Obstet Gynecol. 2014;210(3):179–193. 10.1016/j.ajog.2014.01.02624565430 · doi ↗ · pubmed ↗
- 2External Cephalic Version and Reducing the Incidence of Term Breech Presentation. Green-top Guideline No. 20a. BJOG Int J Obstet Gynaecol. 2017;124(7):e 178–92. 10.1111/1471-0528.14466. · doi ↗
- 3External Cephalic Version. ACOG Practice Bulletin, Number 221. Obstet Gynecol. 2020;135(5):e 203–12. 10.1097/AOG.0000000000003837.32332415 · doi ↗ · pubmed ↗
- 4Gulati D, Hjelde GI. Indications for Cesarean Sections at Korle Bu Teaching Hospital, Ghana. Master thesis. 2012. Accessed September 18, 2023. https://www.duo.uio.no/handle/10852/29016
- 5Sekhon M, Cartwright M, Francis JJ. Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Serv Res. 2017;17(1):88. 10.1186/s 12913-017-2031-8.28126032 PMC 5267473 · doi ↗ · pubmed ↗
- 6Attride-Stirling J. Thematic networks: an analytic tool for qualitative research. Qual Res. 2001;1(3):385–405. 10.1177/146879410100100307. · doi ↗
- 7Rosman AN, Guijt A, Vlemmix F, Rijnders M, Mol BWJ, Kok M. Contraindications for external cephalic version in breech position at term: a systematic review. Acta Obstet Gynecol Scand. 2013;92(2):137–42. 10.1111/aogs.12011.22994660 · doi ↗ · pubmed ↗
- 8Sánchez-Romero J, Gallego-Pozuelo RM, Dahmouni-Dahmouni H, External cephalic version following prior cesarean delivery: A comparative cohort analysis. Int J Gynecol Obstet. 2024;167(3):1066–74. 10.1002/ijgo.15738. · doi ↗