Development and evaluation of a novel prehospital antidote service providing methylthioninium chloride (methylene blue) for sodium nitrite poisoning
Gregory Davies, Jason Wiles, Alison Walker, Christopher Humphries

TL;DR
A new prehospital antidote service using methylene blue was developed to treat sodium nitrite poisoning, showing potential but needing more evidence for broader use.
Contribution
A novel prehospital methylthioninium chloride service was developed and evaluated for sodium nitrite poisoning.
Findings
Three patients received prehospital methylthioninium chloride, with MetHb levels decreasing and all surviving.
The service had minimal consumable costs and identified areas for improvement.
Only nine cases were observed, suggesting specialist team restriction is proportionate.
Abstract
Sodium nitrite has become established as a method of self-harm and suicide. Toxicity occurs primarily through the formation of methaemoglobin (MetHb). In response to a coroner request, West Midlands Ambulance Service developed a prehospital methylthioninium chloride (methylene blue) capability within the specialist Hazardous Area Response Team (HART) to treat methaemoglobinaemia. A service evaluation was planned to understand the impact. A retrospective observational series of patients, during a planned evaluation period from 1 July 2020 to 1 July 2024. All patients receiving a HART response for suspected sodium nitrite poisoning were included. A Patient Group Direction (PGD) for the treatment of methaemoglobinaemia by paramedics was produced, allowing treatment with intravenous methylthioninium chloride 1–2 mg/kg in specific circumstances. MetHb levels were assessed using handheld…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
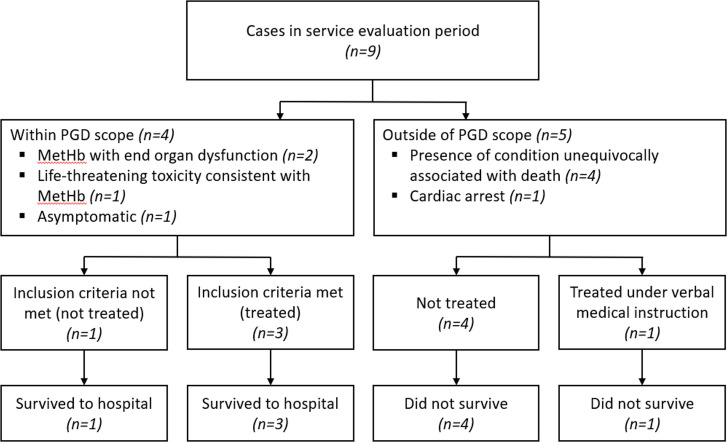 Figure 1
Figure 1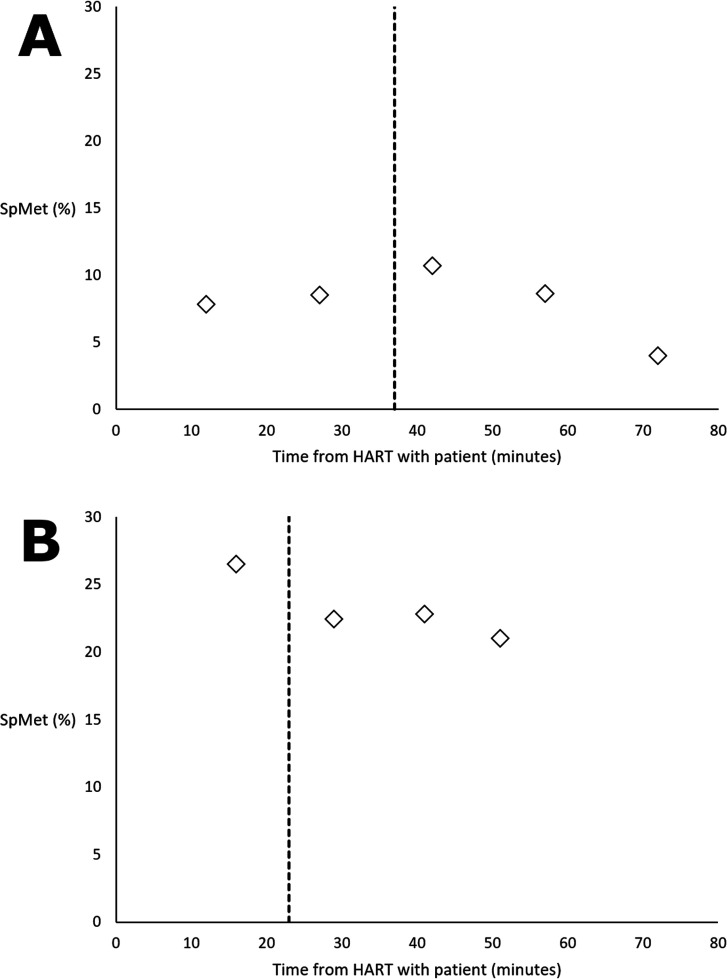 Figure 2
Figure 2| WMAS HART | |
|---|---|
|
Life-threatening cases even if point-of-care MetHb unavailable. MetHb with evidence of end-organ dysfunction (eg, shortness of breath, chest pain, confusion). Consider if MetHb <30% with pre-existing disease increasing susceptibility to tissue hypoxia. | |
|
| 1–2 mg/kg |
|
| Repeat dose at 60 min in cases of persistent or recurrent symptoms, or if MetHb levels remain significantly higher than normal. Maximum 4 mg/kg total. |
|
| 5 mg/mL concentration from ampoule by slow intravenous injection (5 min). |
|
| Not indicated under PGD. |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | |
|---|---|---|---|---|---|
|
| Female | Female | Male | Male | Male |
|
| 30–39 | 30–39 | 30–39 | 50–59 | 10–19 |
| 25 | 30 | 9 | Not reported—substance evident on scene | 50 | |
|
| Respiratory distress, tachycardia, reduced level of alertness, diaphoresis | Respiratory distress, tachycardia, chest discomfort | Respiratory distress, tachycardia, chest discomfort, diaphoresis, confusion | No evidence of end-organ dysfunction | Cardiac arrest |
| 10.7 | 26.5 | Unrecordable | 0 | N/A | |
| 70 | 70 | 90 | N/A | Not recorded | |
| 4.0 | 21.0 | Not available | N/A | N/A | |
| 15 | 43 | 25 | 68 | 16 | |
| 30 | 16 | 7 | 18 | 44 | |
| 37 | 23 | 22 | N/A | 0 | |
| 44 | 30 | 22 | 62 | N/A | |
|
| Survived to hospital | Survived to hospital | Survived to hospital | Survived to hospital | Cardiac arrest |
- —http://dx.doi.org/10.13039/100014589Chief Scientist Office, Scottish Government Health and Social Care Directorate
- —http://dx.doi.org/10.13039/501100000265Medical Research Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoisoning and overdose treatments · Neonatal Health and Biochemistry · Methemoglobinemia and Tumor Lysis Syndrome
Introduction
Sodium nitrite is an inorganic compound, historically best known to clinical toxicologists as an antidote with a role in the treatment of cyanide toxicity.1 2 While it is still licensed for this purpose, and has legitimate public uses, including as a meat preservative and as a corrosion inhibitor, data have emerged in recent years suggesting that it has become an increasingly well-known method of deliberate self-harm ingestion and suicide.3 Discussion of the use of sodium nitrite as a method of suicide on online forums has increased, and though the UK lacks robust data on self-harm poisonings, it appears that use of sodium nitrite as a method of suicide may be growing.4 5
The mechanism of sodium nitrite toxicity is through the conversion of haemoglobin to methaemoglobin (MetHb), by indirect oxidation of ferrous iron to ferric iron which cannot bind oxygen, leading to tissue hypoxia and oxidative stress.6 Nitrite-induced vasodilation may also occur, contributing to hypotension. The typical antidote provided in hospitals is methylthioninium chloride (methylene blue), which acts as an electron donor to reduce MetHb.7 While recommendations regarding antidote stocking for emergency departments exist, the only antidotes routinely available in the UK prehospital setting are activated charcoal, atropine and naloxone.8 9 Given the time-critical nature of these presentations, and the potential for the peak effect of methylthioninium chloride to be delayed for up to 30 min after administration, there have been calls to introduce methylthioninium chloride to the prehospital environment.10
UK coroners may issue a Regulation 28 Prevention of Future Deaths Report to specific individuals or organisations, when they believe that action should be taken to prevent future deaths. West Midlands Ambulance Service (WMAS) received such a report in January 2020, requesting an examination of ways to improve patient outcomes following sodium nitrite ingestion, and specifically examining the role of methylthioninium chloride.
A pilot programme was developed to allow the WMAS Hazardous Area Response Teams (HART) to provide methylthioninium chloride for the treatment of methaemoglobinaemia under a Patient Group Direction (PGD).11 PGDs allow a legal framework for the supply and administration (by healthcare professionals) of specified medicines to predefined patient groups in prespecified circumstances. This allows the provision of treatments without the case-by-case input of a prescriber. A service evaluation was planned to understand the impact of the change on clinical effectiveness and prehospital clinical outcomes (in all patients assessed for the potential administration of methylthioninium chloride) and resource utilisation (at a service level). The results of the evaluation and case series of patients treated are presented here.
Methods
Design and participants
The study design was a retrospective observational series of all patients receiving a HART response for suspected sodium nitrite poisoning from 1 July 2020 to 1 July 2024.
Setting
WMAS is an ambulance service provider (emergency medical service—EMS—provider) to a population of 5.6 million, over an area of 5000 square miles. UK ambulance services all have HART units tasked with providing the response in the presence of potentially hazardous materials or environments, and the provision of specialist skills, equipment and medications not provided by standard emergency ambulances.
Incidents featuring suspicious substances (eg, an unidentified white powder, later found to be sodium nitrite) automatically trigger a WMAS HART response. If the presence of sodium nitrite only became apparent after the initial call (eg, on standard crew attendance), a HART response would then become indicated. Interrogation by the Incident Command Desk was a parallel process to standard EMS dispatch, and HART dispatch therefore did not delay routine clinical care if attendance by a non-specialist crew was appropriate based on initial information.
Of note, if initial call information suggests an unwell patient in the context of a suspicious substance, it is standard care that a routine EMS crew would not commence clinical care due to the potential risk to care providers and would instead await the arrival of HART. However, if clinical care has already commenced, and ingestion of sodium nitrite subsequently becomes apparent, routine EMS crews may transport the patient to hospital without awaiting HART. In these cases, HART would typically attempt to intercept the patient in transit to assist in providing clinical care. In cases of suspected sodium nitrite ingestion where the victim has unequivocal signs of death, HART will be called but will not treat. These calls may have slower response times given the lack of urgency in these situations.
Methylthioninium chloride was stocked as 50 mg/10 mL ampoules for injection. MetHb percentage values were obtained using Masimo Rad-57 Handheld Pulse CO-Oximeters with Masimo Rainbow SET Technology. PGD-specific training to WMAS HART paramedics was provided as part of standard training cycles. All patients in whom there was a clinical suspicion of methaemoglobinaemia had CO-Oximetry performed.
The indications for treatment of methaemoglobinaemia were based on the WMAS interpretation of TOXBASE advice, applied to the prehospital setting at the time when the PGD was authorised. TOXBASE is the clinical toxicology database of the UK National Poisons Information Service (NPIS), accessible by health professionals as an additional support tool for medical decision-making.6 Adaptation was primarily aimed at delivering a pragmatic treatment guideline for use in the prehospital setting to reduce risk for patients who were likely to be at the greatest risk of poor outcomes. Indications for treatment of methaemoglobinaemia under the PGD are provided in table 1.
Data collection and analysis
Patient data collected were limited to data contained within electronic patient record forms. All domains for which data were collected are reported in the results without omission. Data collection was undertaken retrospectively by all evaluators (GD, JW, AW, CH) and consensus on any areas of data abstraction disagreement was reached through group discussion. In-hospital data (eg, venous blood gas results) were not available.
Costs assessed were those additional costs directly attributable to the acquisition of consumables for the HART capability to provide methylthioninium chloride antidote therapy, rather than the entire cost attributable to responding to the patient. Costings were provided directly by WMAS HART and are provided as British Pound Sterling (GBP), excluding Value Added Tax (VAT), rounded to the nearest whole number.
Patient and public involvement
Patient and public involvement was not sought for this service evaluation. Introduction of the service was as a result of a coroner’s request requesting that WMAS examine the role of methylthioninium chloride in treating sodium nitrite ingestion.
Results
Nine cases received a HART response for sodium nitrite ingestion. Four patients had conditions unequivocally associated with death and were not treated (figure 1). Three patients received methylthioninium chloride under PGD eligibility criteria. One additional patient reported sodium nitrite ingestion but had no clinical findings suggestive of toxicity and a normal MetHb percentage on CO-Oximetry and therefore did not receive methylthioninium chloride. A further patient was in cardiac arrest and thus ineligible under the PGD (identified as the patient in cardiac arrest in figure 1); this patient received treatment with methylthioninium chloride for clinically suspected sodium nitrite ingestion from HART under the explicit direction of medical staff on arrival at hospital as an adjunct to cardiopulmonary resuscitation and did not survive (dose not recorded).
Service evaluation flow chart. Conditions unequivocally associated with death are: massive cranial and cerebral destruction, hemicorporectomy or similar massive injury, decomposition/putrefaction, incineration, hypostasis, rigour mortis. MetHb, methaemoglobin; PGD, Patient Group Direction.
Patients 1 and 2 had clearly reported times of ingestion and methylthioninium chloride dosing, as well as serial MetHb readings documented during treatment and these are therefore included for interest (figure 2). Patient 3 had clinical findings consistent with sodium nitrite toxicity, but poor peripheral perfusion precluding CO-Oximetry.
SpMet (%), as measured by a handheld pulse CO-Oximetry, in (A) patient 1 and (B) patient 2, before and after methylthioninium chloride administration (indicated by the vertical dashed line). HART, Hazardous Area Response Team; SpMet, methaemoglobin saturation.
Table 2 describes the five patients assessed for prehospital administration of methylthioninium chloride (four under PGD indications, one under verbal instruction). The data demonstrate variation within each time-stamped aspect of the patient journey, though the time from HART arrival to antidote use became shorter with increasing HART experience. Improvements were seen in SpMet readings in patients 1 and 2 following treatment, while readings could not be obtained in the other treated patients (3 and 5).
Consumables costs associated with the introduction of methylthioninium chloride were minimal. Two of the CO-Oximeters used were already stocked on each HART vehicle to meet other service capability requirements. If a novel service required purchasing these devices, provision of a single device would cost approximately £5825. Supplying all three HART vehicles with methylthioninium chloride had an initial cost of £193 per vehicle (three vehicles) and a per-dose consumables cost of approximately £80 for a 1 mg/kg adult dosing.
Discussion
Feasibility
This service evaluation demonstrates that the pathway was not only technically deliverable by specialist paramedics, but also workable as a wider service. The findings support the feasibility of the overall service model from clinical, governance and logistical perspectives.
A key finding is the successful implementation and use of the PGD. This demonstrates governance feasibility, providing a robust legal and clinical framework for a complex, high-risk and infrequent intervention in the prehospital environment. Feasibility was also evident in the paramedics’ clinical decision-making; three eligible patients were identified, while treatment was appropriately withheld from a patient with no objective evidence of toxicity, clearly demonstrating professional capacity for nuanced clinical judgement, not just task completion.
Furthermore, the data support the proportionality and sustainability of the model. The low number of cases confirms that restricting this specialist capability to HART is an appropriate and efficient use of resources. This targeted approach is made economically feasible by leveraging existing HART infrastructure, such as the pre-existing stock of CO-oximeters and the integration of new competencies into routine training cycles. In contrast, a service expansion to all routine ambulances would likely be prohibitively expensive and face significant logistical barriers related to medicine storage and governance, reinforcing that this specialist team model is a pragmatic and workable solution.
Time to HART activation, treatment and transport
The duration between initial call and HART activation can be significant. This suggests that there may be work to be done on appropriate flags to expedite the identification of potential cases to HART dispatch systems, but this would require amendments by National Health Service Pathways and Medical Priority Dispatch call-taking systems. Callers may not use the chemical name for sodium nitrite, but may use colloquialisms describing types of salt, such as ‘curing salt’.10 Inevitably, in some cases, evidence of sodium nitrite ingestion will only become apparent after the initial call—either due to evidence on scene or clinical interrogation of the caller.
Time from HART activation to arrival is a feature of geography and may be seen as introducing unnecessary delay. However, the authors would emphasise that in some contexts (eg, when it is known from call information that there is an acutely unwell patient in the context of an unknown substance), HART is considered the only appropriate dispatch response due to the potential risk to care providers and their attendance does not delay a standard ambulance attendance, as this would not be provided. Additionally, in cases where clinical care had already commenced prior to sodium nitrite ingestion being identified, no standard EMS crew were prevented from transporting their patient to hospital if they felt able to do so (as seen with patient 5, where HART attempted to intercept the patient in transit, but were unable to do so, and therefore met the patient on arrival at hospital).
Time from HART arrival to treatment was longest with patient 1. The HART members involved acknowledged a steep learning curve requiring senior clinical advice, and improvements were seen in time to treatment in subsequent cases. While this may appear to be a delay which would not occur in hospital, the most recent available UK audit data suggests that only 84.3% of hospitals have methylthioninium chloride available immediately.12 This was borne out in HART’s clinical experience; the patient not treated under the PGD as they were in cardiac arrest in fact had methylthioninium chloride administered by HART within a hospital resuscitation room on a doctor’s verbal instruction, as the receiving hospital was unable to locate their own antidote stock.
Time from treatment to arrival at hospital is not considered to represent an additional delay versus non-HART care.
Patient outcomes
To our knowledge, all patients who survived to hospital arrival subsequently survived to discharge, as there have been no coroner’s inquests relating to these cases. The authors acknowledge the small patient numbers in this observational series limit claims regarding treatment benefits and that there is the potential for unidentified consequences. Nevertheless, the centralisation of care to a specialised resource does not appear to have negatively impacted any clinical outcomes in the prehospital phase of patient care, though the study lacks a control group.
Quality of data
Due to the non-standard nature of sodium nitrite cases triggering call transfer to the dedicated incident command desk, and direct feedback to the WMAS Medical Director of all coroner cases, we do not believe we have missed any potentially eligible cases. However, it is possible that patients with methaemoglobinaemia from other causes, with potential to benefit from treatment with methylthioninium chloride, were not identified due to the nature of prehospital medicine precluding gold-standard diagnosis of raised MetHb levels. Additionally, we do not report patient data confirming the diagnosis of methaemoglobinaemia using blood sampling, as WMAS lack suitable data sharing agreements with the multiple receiving hospitals within the geographical area.
Potential PGD changes
The current PGD may warrant revision. A PGD provides the legal framework for administration by non-prescribers; however, this requires strict adherence to the written protocol and legally precludes case-by-case clinical direction from external sources like the NPIS. Within this legal constraint, the dosing range could be aligned more closely with TOXBASE advice, as concerns regarding serotonin toxicity are rare at doses under 7 mg/kg and the principle of direct collaboration with NPIS on national treatment guidelines is well-established.6 13 A key consideration remains the reliance on non-invasive CO-Oximetry, as its accuracy for the high readings that guide treatment is uncertain.1416 The PGD also excludes use in cardiac arrest, which is consistent with TOXBASE but differs from American Heart Association guidelines, which mention the drug for life-threatening toxicity but note a lack of evidence to guide its specific use during cardiac arrest.17 18
The need for further research
Given that several UK ambulance services are now considering similar models, a national rollout is a realistic prospect. However, there is a risk that enthusiasm for this novel treatment could outpace the evidence, leading to premature adoption. Treatment guidelines require a firm foundation in clinical evidence, with an onus on guideline authors to acknowledge when existing evidence is insufficient.19 20
Therefore, before widespread implementation, a formal study is essential to build this evidence base. We suggest that an appropriate evaluation could take the form of a stepped wedge cluster randomised trial. Designing and delivering such a study would require significant expertise encompassing emergency medicine, clinical toxicology and clinical trials methodology.2123 Proceeding with an unevaluated national roll-out risks not only the inefficient allocation of significant resources but also potential patient harm from an intervention that has not yet been proven safe and effective in the prehospital setting.
Conclusion
This evaluation demonstrated that it is feasible to deliver prehospital methylthioninium chloride for probable sodium nitrite-induced methaemoglobinaemia in the UK using specialised paramedics, and that this enables the prehospital treatment of methaemoglobinaemia at relatively low cost.
Findings from this evaluation can inform decisions regarding adoption of methylthioninium chloride in ambulance trusts across the UK. The use of prehospital methylthioninium chloride for the treatment of methaemoglobinaemia currently lacks sufficient evidence to support adoption without further evaluation. A stepped wedge cluster randomised trial would allow for the real-world impact to be clearly understood.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thanacoody HKR Cyanide Bateman DN Jefferson RD Thomas SHL et al Oxford Desk Reference: Toxicology New York (NY)Oxford University Press 201422931
- 2Howland MA Antidotes in depth: nitrites (amyl and sodium) and sodium thiosulphate Nelson LS Howland MA Lewin NA Goldfrank’s toxicologic emergencies New York (NY)Mc Graw-Hill Education 20191698702
- 3Hikin LJ Ho J Morley SR et al Sodium nitrite poisoning: A series of 20 fatalities in which post-mortem blood nitrite and nitrate concentrations are reported Forensic Sci Int 202334511161010.1016/j.forsciint.2023.11161036848754 · doi ↗ · pubmed ↗
- 4Mack KA Kaczkowski W Sumner S et al Special Report from the CDC: Suicide rates, sodium nitrite-related suicides, and online content, United States J Safety Res 202489361810.1016/j.jsr.2024.03.00238858061 PMC 11262023 · doi ↗ · pubmed ↗
- 5Schölin L Humphries C Eddleston M et al De-siloing substance misuse and self-harm research through integrated public health and emergency medicine Lancet Public Health 202510 e 7162110.1016/S 2468-2667(25)00096-940383135 · doi ↗ · pubmed ↗
- 6Bradberry A EAPCCT fellows’ webinar: methemoglobinaemia: diagnosis and treatment 2023 Availablehttps://eapcct.org/fellows/
- 7TOXBASE Sodium nitrite 2022 Availablehttps://www.toxbase.org/poisons-index-a-z/s-products/sodium-nitrite/
- 8Humphries C Eddleston M Dear J The emergency treatment of poisoning Medicine (Baltimore)202352566110.1016/j.mpmed.2023.10.004 · doi ↗