Mixed-methods evaluation of targeted leadership development training to support the career progression of the black and minority ethnic NHS workforce
Holly Blake, Keir Scarlett, Sala Kamkosi Khulumula, Niki Chouliara

TL;DR
This study evaluates leadership training programs aimed at helping Black and minority ethnic NHS workers advance their careers, finding that while the programs are beneficial, broader institutional changes are needed to address racial disparities.
Contribution
The study provides empirical evidence on the effectiveness of targeted leadership training for BME NHS workers and highlights the need for institutional reforms.
Findings
Participants reported positive impacts from the leadership programs, including increased self-confidence and career opportunities.
Institutional barriers and structural racism were identified as significant obstacles to career progression for BME workers.
Most participants achieved meaningful career development after completing the programs.
Abstract
Black and minority ethnic (BME) workers within the National Health Service (NHS) experience barriers to attainment of senior leadership roles. The NHS Leadership Academy delivered two Leadership Programmes addressing barriers to progression among the BME workforce, the Stepping Up (middle managers) and Ready Now (senior leaders) programmes. Mixed-methods evaluation involving an online survey (n=39; 20m/19f, identifying with 10 ethnic groups) and qualitative interviews (n=8; 5m/3f) with programme participants investigating barriers and the extent to which targeted leadership programmes impacted their career progression. Analysis included descriptive statistics and thematic analysis of qualitative data. Participants reported institutional barriers to career progression and experiences of structural racism. Evaluation of targeted leadership programmes was consistently positive, providing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
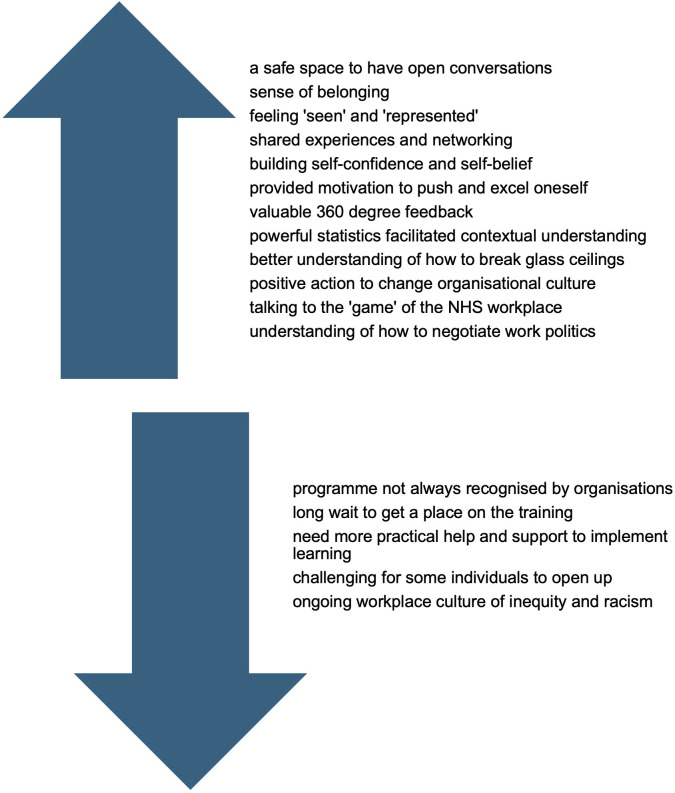 Figure 1
Figure 1| Theme | Illustrative quotes |
|---|---|
| Theme 1: | “Whilst I didn’t greatly benefit within the Trust, I think my boss used it as a flag to bolster their credentials” (Asian British—other, female, 45–54: RN) |
| Theme 2: | “When you go on the programme you have a sponsor within the trust, I think more should be asked of those sponsors… exposing you to opportunities… giving you access to higher level meetings, allowing you to sit and shadow them” (Asian British—other, female, 45–54, RN) |
| Theme 3: | “To understand the impact of such trauma in the landscape and how to push beyond” (Asian British—other, female, 45–54, RN) |
| Theme 4: | “It gave me the confidence to put myself in the shop window, because if I hadn’t, I wouldn’t have had the opportunities I have had” (Black British African/Caribbean, male, 45–54, RN) |
| Theme 5: | “Because of that… I have moved significantly from where I was when I went on the programme… I am now an Interim Chief Allied Health Professional” (Black/Black British—African, male, 45–54, RN) |
- —http://dx.doi.org/10.13039/501100000269Economic and Social Research Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Health Workforce Issues · Medical Education and Admissions · Innovations in Medical Education
Introduction
Over one in five staff working in the National Health Service (NHS) in England are from black and minority ethnic (BME) backgrounds (22.4%1), but only 10.3% of those in senior management roles are BME workers, who are over-represented in less senior roles (34.5% at band 5).2 Many BME staff believe that their employer does not provide equal opportunities to career progression and promotion, compared with their white colleagues, specifically in relation to senior leadership roles.1 Indeed, white applicants are 1.61 times more likely to be shortlisted for job vacancies compared with BME applicants.1 The NHS Race and Health Observatory outlines the need to accelerate action to diversify its senior leadership.3 The NHS Leadership Academy has delivered two Leadership Programmes specifically targeted at BME staff, ‘Stepping Up’ aimed at middle managers, Bands 5–7 and ‘Ready Now’ suitable for senior leadership roles, Bands 8+. These programmes aimed to create greater levels of sustainable inclusion within the NHS by addressing social, organisational and psychological barriers restricting BME colleagues from progression. Stepping Up4 was delivered over 5 days in total, attended face to face, over 2–3 months. There were approximately six cohorts per year, delivered between 2014 and 2019. Ready Now5 consisted of 12 residential dates spread across 5 modules. There were approximately five cohorts per year, delivered between 2014 and 2019. This study aimed to investigate barriers to career progression, experiences of alumni relating to the leadership programme they attended, and any perceived impacts of the programme on their career progression.
Methods
This mixed-methods study involved an online survey with closed and open-ended questions (phase 1: QUANT+QUAL), and individual qualitative interviews (phase 2: QUAL). Data were integrated to address the study aim. Study reporting was guided by the ‘Good Reporting of A Mixed Methods Study’ framework developed by O’Cathain et al.6 This aims to enhance the quality of reporting through a set of six reporting guidelines.6 Mixed-methods research was selected as it provides the opportunity to represent a greater diversity of views. Using an existing typology of research purposes,7 the study purpose was to ‘add to the knowledge base’ and ‘understand a complex phenomenon’, with study findings having potential to ‘have a personal, social, institutional and/or organisational impact’. Individuals who had taken part in all cohorts of the Stepping Up or Ready Now leadership development programmes between 2014 and 2019 (total n=990) were invited to take part in the study. Stepping Up consisted of two modules, lasting 3 months each. Ready Now was a year-long programme split across five modules. There were 40 individuals per cohort in each programme. The programme content and delivery format remained the same year-to-year. Here, we adopt the terminology used in the programmes, (‘black and minority ethnic: BME’), but this also reflects ‘BAME’, ‘ethnically minoritised communities’ or ‘global majority’. This was a convenience sample. Invitations were sent by email via the NHS Leadership Academy in September 2023 and contained the study information sheet and a link to an anonymous online survey hosted on Microsoft Forms (online supplemental file 1). A single reminder was sent 7 weeks later. Survey completers could consent to take part in an online semistructured qualitative interview (online supplemental file 2) with the study researcher, on Microsoft Teams, to share their views in more depth. The survey included demographic items, views towards BME-targeted programmes, and items relating to the programme attended, perceived benefits of attending, and any career progression since programme completion. Response options included categorical (yes/no) items, free text and 5-point Likert-type scales: ‘extremely useful’, ‘very useful’, ‘somewhat useful’, ‘slightly not useful’ and ‘not at all’. Quantitative survey data were analysed using IBM SPSS Statistics (V.27). Interviews were audio recorded, transcribed and anonymised. Inductive thematic analysis8 was applied to the two qualitative data sets collected from free-text responses in the online survey (phase 1) and interviews (phase 2) to enable the identification and analysis of notable themes or patterns in the data. There were six steps of thematic analysis conducted as part of this process: familiarisation with the data, the creation of a coding system, coding data and identifying key themes, reviewing and defining notable themes, and then analysis of those themes. Qualitative data were analysed using MAXQDA Analytics Pro V.24.4.1, which allows for a ‘high degree of reflexivity’9 in the organisation and coding of data. MAXQDA allowed data from multiple documents to be compiled and coded as individual themes emerged, using functionality such as memos and hyperlinks between multiple documents. Through this process, themes were gradually condensed and organised into a more refined group of thematic categories which demonstrated an emerging narrative to the participant experience.
Results
39 individuals (20 male, 19 female) who had attended the Stepping Up (n=20) or Ready Now (n=19) programmes between 2014 and 2019 completed the survey. All were heterosexual, seven had a disability. They were aged 35–44 (n=14, 36%), 45–54 (n=19, 49%) and 55–64 years (n=6, 15%) and identified with 10 different ethnicities: Asian/Asian British–Indian (n=13, 33%), Black/Black British–African (n=7, 18%), Black/Black British–Caribbean (n=7, 18%), Asian/Asian British–Pakistani (n=5, 13%), Mixed–White and Black African (n=1, 2.5%), Asian/Asian British–Chinese (n=1, 2.5%), Mixed–White and Black Caribbean (n=1, 2.5%), White other–Slovakian (n=1, 2.5%), Japanese/Korean/Chinese (n=1, 2.5%), Asian British–Other (n=1, 2.5%). All except one found the programme useful (‘transformational’, ‘empowering’, ‘a self-discovery journey’, ‘life-changing experience’, ‘the best training and development experience of my whole professional career’, ‘can’t rate highly enough’) and reporting having put their learning into practice (n=38, 97%). Most participants believed a targeted programme was better than generic programmes (n=34, 81%), would recommend targeted leadership programmes to colleagues (n=36, 92%) and had shared their learning with BME colleagues (n=36, 92%). Reported benefits of the programme included: it being a ‘safe space’ (n=14, 36%), with tailored content to BME experiences (n=9, 23%), networking opportunities (n=8, 20.5%), exposure to other opportunities (n=5, 13%) and the wide recognition of these NHS leadership programmes among employers (n=2, 5%). Views towards the programme are shown in figure 1.
Views towards the benefits and challenges of the programme. NHS, National Health Service.
Mixed-methods analysis identified five themes relating to the influencers of career progression and outcomes of the programme(s) (table 1).
Theme 1: institutional barriers to career progression
There were accounts of institutional racism, challenges associated with getting time off work to attend training or access senior level programmes compared with white colleagues, perceptions of being passed over for promotion or ‘sidelined’ into lower level or equality, diversity and inclusion roles.
Theme 2: role of line managers in career progression
There were mixed experiences of line manager support, some participants felt dismissed or recipients of ‘lip service’ where progression opportunities were concerned. Participants advocated targeted approaches led by line managers, such as shadowing, mentoring and talent spotting at Bands 6 and 7.
Theme 3: creating psychological safety
Some participants had experienced ‘gaslighting’ leading to self-doubt in their capability. The programmes created a ‘safe space’ for sharing experiences and strategies to support career development and progression.
Theme 4: instilling confidence in oneself
Most participants reported increased self-confidence after attending the programme, and subsequently, were more motivated to take actions relating to personal development and career progression.
Theme 5: tangible career progression.
Of survey respondents, 34 (87%) believed that attending the programme positively impacted their career progression. Participants reported that following the programme they ‘progressed in their career’ (n=24/39, 62%), changed career/job role with a ‘sideways step’ (n=5/39, 13%), remained in their role (n=6/39, 15%) or had another outcome (eg, retirement) (n=4/39, 10%). This was reflected in the interview data, where many participants reported having transitioned into senior job roles.
Discussion
These targeted leadership programmes delivered by the NHS Leadership Academy4 5 were perceived to be highly successful in providing personal development and progressing the careers of NHS staff from BME backgrounds. Many participants had changed job roles, moved to other institutions or into roles that offered more flexibility and autonomy and/or progressed into more senior positions. All participants reported positive impacts on their career, including those who had remained in the same job role. There were many benefits of attendance, but the creation of a safe space in which BME individuals could share experiences, speak freely and feel recognised was the most prominent. For some, safe spaces were sustained postprogramme via WhatsApp groups, creating ongoing opportunities for community building and networking.
Mixed-methods analysis allowed greater insights and perspectives than one method alone, which is valuable given the lack of prior research on this topic. There are several study limitations. Responses were gathered from a small pool of programme attendees due to the time and resource impacts of data integration in a sequential mixed methods study. The views of those who could not be successfully contacted (eg, non-functioning email address), or chose not to respond, are not known. Asian/Asian British Indian participants were over-represented in the sample. Due to the small sample size, we were unable to explore participants’ experience in the context of sex, disability or sexual orientation or the influence of intersectionality of participant identities on their perceptions and views.
Nonetheless, attendance on the programmes increased participants’ confidence and motivation for personal development, which are ‘important determinants of success’ in career progression.10 11 Those with high levels of confidence are often more motivated to overcome obstacles and take beneficial risks12 which may increase the likelihood of career progression.
However, there is widespread concern for the institutional barriers that remain and hinder progression for BME individuals. Some participants reported a sense of ‘career plateauing’, a lack of managerial support for development opportunities, fear of the impact of an institutionally racist healthcare system on patients and intentions to leave the NHS. The ‘glass ceiling’ of institutional racism on career progression is well documented1 13 and manifests in the devaluation and disregard for the experience, qualifications and potential of individuals from a BME background. These findings align with prior research suggesting that ‘organisations create a segregated and racialised career experience’ for those from minoritised ethnic groups, which holds back careers.14
Due to financial limitations, these programmes have ceased, and many Trusts offer generic in-house training instead, although quality and access can be variable. This may hinder the development of future BME leaders. Our mixed-methods evaluation of Stepping Up and Ready Now was consistently positive. The programmes were highly valued by attendees with unique benefits extending beyond generic leadership training. The ethos of targeted leadership programmes clearly aligns with the recommendation for embedding race across development opportunities and diversifying senior leadership.3 15 However, the broader impact of such leadership programmes remains limited without addressing wider institutional barriers to progression and tackling racialised workplace inequities.
Supplementary material
10.1136/leader-2024-001175online supplemental file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NHS Workforce Race Equality Standard 2021 (NHS WRES)Availablehttps://www.england.nhs.uk/publication/nhs-workforce-race-equality-standard-2022/
- 2Ishaq M Hussain AM BAME employees’ work experience in the UK public sector: an empirical study of academic and research libraries IJPSM 2022353344810.1108/IJPSM-03-2021-0069 · doi ↗
- 3Robertson R Williams E Buck D et al Ethnic health inequalities and the nhs: driving progress in a changing system The Kings Fund & NHS Race and Health Observatory 2021 Availablehttps://www.nhsrho.org/wp-content/uploads/2023/05/Ethnic-Health-Inequalities-Kings-Fund-Report.pdf
- 4NHS Leadership Academy Stepping Up programme: Line manager guide Availablehttps://www.leadershipacademy.nhs.uk/wp-content/uploads/dlm_uploads/2018/10/Stepping-Up-programme-Line-Manager-guide.pdf
- 5NHS Leadership Academy Ready Now programme: Line manager guide Availablehttps://www.leadershipacademy.nhs.uk/wp-content/uploads/dlm_uploads/2019/01/NHS-Leadership_Ready-Now-Management-Guide-19-20-1.pdf
- 6O’cathain A Murphy E Nicholl J The Quality of Mixed Methods Studies in Health Services Research J Health Serv Res Policy 20081392810.1258/jhsrp.2007.00707418416914 · doi ↗ · pubmed ↗
- 7Newman I Ridenour CS Newman C et al A Typology of Research Purposes and Its Relationship to Mixed Methods Thousand Oaks, CA Sage 200316788
- 8Braun V Clarke V Using thematic analysis in psychology Qual Res Psychol 200637710110.1191/1478088706 qp 063oa · doi ↗