Barriers and Facilitators to Expanding User-Administered Injectable Contraceptives in the United States
Chase Clark, An-Lin Cheng, Laura Creason, Jennifer Karlin

TL;DR
This study explores factors influencing the use of user-administered contraceptive injections among healthcare professionals in the U.S.
Contribution
The study identifies professional, institutional, and policy-level barriers and facilitators to prescribing user-administered subcutaneous DMPA.
Findings
Only 34.8% of healthcare professionals actively prescribed subcutaneous DMPA despite 74.5% awareness.
Awareness and prescribing were influenced by professional specialization, institutional setting, and state policies.
Gender diversity and insurance coverage were significant facilitators for prescribing subcutaneous DMPA.
Abstract
Addressing barriers and implementing facilitators across domains can guide efforts to expand access to subcutaneous depot medroxyprogesterone acetate for user-administration and mitigate disparities in contraceptive provision. To identify facilitators and barriers to prescribing subcutaneous depot medroxyprogesterone acetate (DMPA) for user administration. This mixed-methods study comprised surveys (N=422) and interviews (N=34) with family planning experts, defined as health care professionals who see at least three contraceptive visits a month, regarding their awareness, knowledge, and practice of prescribing subcutaneous DMPA for user administration. We found that 74.5% of professionals reported awareness of subcutaneous DMPA for user administration, but only 34.8% actively prescribed it. Professionals who completed a fellowship in reproductive health, specialized in obstetrics and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
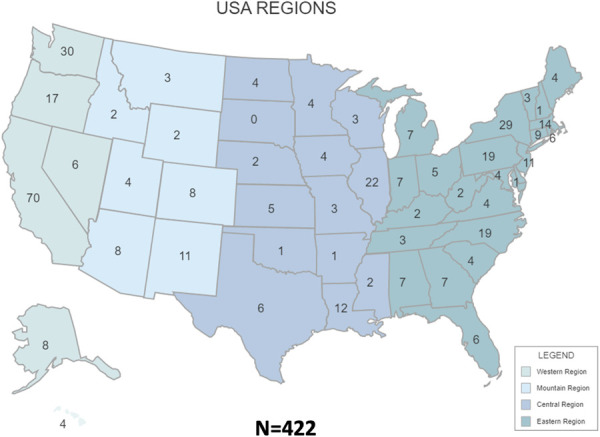 Fig. 1
Fig. 1| Gender | |
| Cisgender female | 355 (84.1) |
| Cisgender male | 44 (10.4) |
| Genderqueer or gender-fluid | 10 (2.4) |
| Transgender male | 5 (1.2) |
| Transgender female | 2 (0.5) |
| None of the above/prefer not to say | 6 (1.4) |
| Age (y) | |
| Under 35 | 114 (27.0) |
| 35–44 | 184 (43.6) |
| 45–54 | 75 (17.8) |
| 55 and older | 49 (11.6) |
| Degree | |
| MD/DO | 233 (55.2) |
| NP/PA/DNP | 107 (25.3) |
| PharmD/BSPharm | 34 (8.1) |
| Masters/PhD | 30 (7.1) |
| RN | 18 (4.3) |
| Practice institution | |
| Academic | 137 (21.5) |
| Primary care clinic | 113 (17.8) |
| Planned Parenthood | 112 (17.6) |
| FQHC | 64 (10.1) |
| Pharmacy | 47 (7.5) |
| Other | 165 (25.5) |
| Title X family planning funding | |
| Yes | 166 (39.3) |
| No | 172 (40.8) |
| Not sure | 84 (19.9) |
| Race and ethnicity | |
| American Indian or Alaska Native | 6 (1.3) |
| Asian | 52 (11.6) |
| Black or African American | 36 (8.0) |
| Hispanic or Latino | 25 (5.6) |
| Native Hawaiian or Pacific Islander | 2 (0.4) |
| None of the above/prefer not to say | 14 (3.1) |
| White | 315 (70.0) |
| Specialty | |
| Family practice/family medicine | 156 (44.6) |
| Obstetrics and gynecology | 89 (25.4) |
| Women's health | 54 (15.4) |
| Adult medicine/internal medicine/ID | 24 (6.9) |
| Other | 16 (4.6) |
| Midwifery | 8 (2.3) |
| Pediatrics | 3 (0.9) |
| Fellowship | |
| No | 157 (67.4) |
| Yes | 76 (32.6) |
| Practice setting | |
| Urban | 294 (49.2) |
| Suburban | 141 (23.6) |
| Telemedicine | 82 (13.8) |
| Rural | 77 (12.9) |
| Frontier | 3 (0.5) |
| Factor | Level | Key | Health Care Professionals Who Were Not Aware | Health Care Professionals Who Were Aware | Total Health Care Professionals |
|
| Health care professional completed a reproductive health fellowship | Professional | None | 43 (29.5) | 103 (70.5) | 146 (100.0) | <.001 |
| 1 y | 2 (12.5) | 14 (87.5) | 16 (100.0) | |||
| 2 y | 1 (1.0) | 70 (99.0) | 71 (100.0) | |||
| Health care professional with obstetrics and gynecology specialty | Professional | Other | 61 (23.4) | 200 (76.6) | 261 (100.0) | .039 |
| Obstetrics and gynecology | 11 (12.4) | 78 (87.6) | 89 (100.0) | |||
| Internal medicine specialty | Professional | Other | 62 (18.8) | 267 (81.2) | 329 (100.0) | .004 |
| Internal medicine | 10 (47.6) | 11 (52.4) | 21 (100.0) | |||
| Contraceptive visits per month, median (IQR) | Professional | 1=10 or less, 2=11–20, 3=21–30, 4=31–40 | 2.4 (1.6) | 3.5 (2.1) | 3.3 (2.0) | <.001 |
| Clinic with Title X funding | Institution | No | 65 (26.1) | 184 (73.9) | 249 (100.0) | .001 |
| Yes | 22 (12.8) | 150 (87.2) | 172 (100.0) | |||
| Clinic in an urban setting | Institution | No | 38 (29.7) | 90 (70.3) | 128 (100.0) | .004 |
| Yes | 49 (16.7) | 245 (83.3) | 294 (100.0) | |||
| Clinic is Planned Parenthood | Institution | No | 80 (25.8) | 230 (74.2) | 310 (100.0) | <.001 |
| Yes | 7 (6.3) | 105 (93.7) | 112 (100.0) | |||
| Clinic is a free-standing reproductive health clinic | Institution | No | 84 (18.1) | 296 (81.9) | 380 (100.0) | .025 |
| Yes | 3 (7.1) | 39 (92.9) | 42 (100.0) | |||
| Pharmacy | Institution | No | 71 (15.9) | 304 (84.1) | 375 (100.0) | .026 |
| Yes | 16 (34.0) | 31 (66.0) | 47 (100.0) | |||
| No. of pregnancy-potential patients, mean±SD | Institution | N/A | 55.8±26.7 | 68.4±26.6 | 65.8±27.0 | <.001 |
| Contraceptive options not offered, mean±SD | Institution | N/A | 4.0±2.3 | 3.1±1.8 | 3.3±1.9 | .001 |
| Factor | Level | Key | Do Not Provide DMPA-SC | Provide DMPA-SC | Total |
|
| Gender, n (%) | Professional | Cisgender female | 164 (61.2) | 104 (38.8) | 268 (100.0) | <.001 |
| Cisgender male | 12 (35.3) | 22 (64.7) | 34 (100.0) | |||
| Nonbinary | 3 (16.67) | 15 (83.3) | 18 (100.0) | |||
| Contraceptive options not offered, mean±SD | Institution | N/A | 3.5±1.8 | 2.4±1.2 | 3.1±1.7 | <.001 |
| Workflow for administering DMPA-SC for user administration available in clinic | Institution | No | 171 (66.5) | 86 (33.5) | 257 (100.0) | <.001 |
| Yes | 8 (12.7) | 55 (87.3) | 63 (100.0) | |||
| Workflow for administering DMPA-SC available but professional responsible for own education, n (%) | Institution | No | 162 (61.4) | 102 (38.6) | 264 (100.0) | <.001 |
| Yes | 17 (30.4) | 39 (69.6) | 56 (100.0) | |||
| Clinic does not have any workflows or has not considered the option, n (%) | Institution | No | 25 (21.0) | 94 (79.0) | 119 (100.0) | <.001 |
| Yes | 154 (76.6) | 47 (23.4) | 201 (100.0) | |||
| DMPA-SC covered by Medicaid | System | No | 140 (71.1) | 57 (28.9) | 197 (100.0) | .039 |
| Yes | 39 (31.7) | 84 (68.3) | 123 (100.0) | |||
| DMPA-SC covered by private insurance | System | No | 158 (69.0) | 71 (31.0) | 229 (100.0) | .004 |
| Yes | 21 (23.3) | 69 (76.7) | 90 (100.0) | |||
| State is considered to have laws protective of reproductive rights according to Guttmacher Institute | System | No | 77 (61.6) | 48 (38.4) | 125 (100.0) | .05 |
| Yes | 91 (50.3) | 90 (49.7) | 181 (100.0) |
| Level | Barrier | Example Quote | Facilitator | Example Quote |
| Patient | Patients may forget to inject DMPA-SC | “I really am puzzled about how we would be able to get people to do their every 3 months” | Medication administration reminders | “A lot of times pharmacies … will text you, ‘Oh, it's ready.’ So, things like that: auto refill systems where people get texts or reminders like, ‘Oh, it's time for your Depo. Come pick it up. And this is the window in which you can inject it and still be in a safe contraceptive period’” |
| Patient | Patients may forget how to inject DMPA-SC | “I would be really hesitant that they remember to do everything” | Reminders how to perform injection | “I like the Reproductive Health Access Project handout for user administration. I like that a lot, because it tells you the basics, and then on the back what you're really in for and how you do this to yourself” |
| Patient | Patients may be unaware of DMPA-SC for user administration as a contraceptive option | “I think that's the biggest [barrier]. I think, like, patients not knowing it's an option” | Advertise directly to consumers | “When we advertise directly to consumer and then they come in asking for it, so that's an option” |
| Patient | Patient may not have transportation to their contraceptive appointments | “[Barriers involve] some of the social determinants of health, like living in a rural area or not having transportation” | Eliminate transportation needs | “I suppose the self-administered would be a way to facilitate that particular barrier: transportation” |
| Patient | Patients may have a fear of needles or self-injecting | “The patients' biggest barriers, I think needle phobia might be one of them” | Aid people to overcome their fear of needles | “I think that in the beginning, they would probably be nervous. Like, am I able to do this? Is this going to hurt? Am I going to mess it up? But I think that, you know, eventually, they can totally, like, build the confidence and do it” |
| Patient | Patients who inject at home may have decreased privacy | “A lot of teenagers like doing things, but if they could do it on their own, too, although … that's something that their parents could find, if they had the needles” | Safely dispose of needles | “I would probably say you can either buy … a sharps container at the pharmacy or, like, order it online, or you can just use like an old laundry detergent container” |
| Professional | Professionals lack awareness of DMPA-SC for user administration as a contraceptive option | “I think even at my institution, the majority of the general gynecologists probably aren't aware that it's an option” | Increase professional awareness | “We all have to get a continuous education somewhere. And so providing that on some big, like, symposiums where they go and target it, I think that would be probably helpful” |
| Professional | Professionals have ideas of who makes an ideal or unideal candidate for self-administered DMPA-SC | “The ideal patient is young due to delay in fertility, those already injecting hormones, those who want depo but don’t want to come to clinic, self-motivated” | Eliminate ideas of patient candidacy | “I don't think there's anyone where I would think, oh, they probably can't do this or wouldn't be interested. I think everyone is probably capable or at least should be given the option” |
| Professional | Professional bias against DMPA | “I think so many people probably undercounsel about depo in general or perceive that patients don't want depo” | ||
| Professional | Professional lacks time to teach proper and safe self-injection technique | “I also think that the time it takes to teach a patient is not insignificant” | Delegate time it takes to teach self-injection to supporting staff | “I have a nurse in my office who then swoops in, does the education” |
| Professional | Professionals may require a pregnancy test before initiation of user-administered DMPA-SC | “I would say you need to do a pregnancy test before you get the second [DMPA injection]” | Do not require a pregnancy test | “I don't think [a pregnancy test is] as important as we previously thought it would be. I think, if patients are educated on why we do it and, again, what the risks are, that this is their life and they're going to be taking charge of their own health, and they can check themselves at home for a pregnancy test” |
| Institution | Institution may lack workflows for prescribing DMPA-SC for user administration | “Gosh, I mean, the provider level, just knowledge that it is an option, knowledge of how to bill effectively, and how to accomplish the prior authorizations effectively” | Implementation of protocols or workflows | “Any leg work … that makes it easier for me to know that, like, if I actually prescribe it, it's going to be, like, available for the patient” |
| Institution | DMPA-SC for user administration may cost the institution | “I feel like some providers may be worried about missed billing opportunities. Like, maybe helping folks understand that admin would probably be on board, because there's not less provider visits, because when they come for their reinjections of IM it's not a provider doing it, it's an MA or a nurse. Which could get could be billed for but frequently isn't” | ||
| Systemic | The FDA has not approved DMPA-SC for user administration | “I mean I feel like one of the things that kind of maybe makes people hesitate or not realize that it's a viable option is the fact that it's approved for provider administration. I know people prescribe and use things off-label all the time. I just feel like, for some reason, contraception seems to be viewed a little bit differently and like, ‘Oh. If the label says this is what it's approved for and how it should be used, that's what we have to do’” | FDA approval of DMPA-SC for user administration | “I truly believe that, in 2004, when the FDA approved it, if they had approved it for user administration and home use, that we would be in a completely different place now” |
| Systemic | Pharmacy stock of DMPA-SC is sparse to nonexistent | “We have an affiliated pharmacy, and I don't know that they keep it in stock” | Increase pharmacy stock | “It would make it easier if pharmacies actually stocked it and you know that, when you show up at the pharmacy to get it, that you don't have to go back and get it another day because they don't have it” |
| Systemic | Insurance coverage | “It's not always covered by insurance and that's a fight” | Insurance coverage of DMPA-SC for user administration | “I'm very lucky, my patients have Medicaid, and Medicaid in [redacted state] pays for it. But I know that it is not on formulary for some of the other insurances” |
- —Society of Family Planning
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Health and Contraception · Global Maternal and Child Health · Reproductive tract infections research
Subcutaneous depot medroxyprogesterone acetate (DMPA) is a progestin-only contraceptive approved for professional administration by the U.S. Food and Drug Administration (FDA) in 2004 for pregnancy prevention. Research demonstrates comparable safety and effectiveness for user administration compared with professional administration,^1–8^ prompting organizations like the Centers for Disease Control and Prevention, Office of Population Affairs, and the World Health Organization to recommend offering the user-administered formulation to individuals of reproductive age.^2,3^ U.S.–based studies highlight interest in user administration, improved continuation rates, and feasibility across diverse populations.^9–18^
Despite its patient-centered benefits and potential to advance equitable health care access, subcutaneous DMPA for user administration remains underutilized in the United States. Limited documentation exists on this gap, with prior studies focusing on health care professional surveys during the coronavirus disease 2019 (COVID-19) pandemic and systematic reviews of implementation strategies.^19–21^ To address this knowledge gap, we conducted a survey and interviews with family planning experts to examine professional awareness, clinical practices, and barriers to offering user-administered subcutaneous DMPA. We hypothesized that barriers to self-administered subcutaneous DMPA span four levels previously identified as categories for care implementation barriers: perceived patient preferences, professional-related factors, clinic-level obstacles, and systemic health care challenges.^22^ This study presents findings and proposes strategies to expand access to this contraceptive option in the United States.
METHODS
This University of California, Davis IRB–approved mixed-methods study recruited family planning experts by means of convenience sampling and snowball recruitment through email listservs through organizations and individuals who had contacts likely to be experts in sexual and reproductive health. A mixed-method survey (Appendix 1, available online at http://links.lww.com/AOG/E482) with multiple choice, Likert-scale, and free-text questions assessed professional awareness, provision, implementation practices, perceptions of patient suitability, and readiness to prescribe subcutaneous DMPA for user administration. Some survey questions had been validated previously, and the entire survey was piloted with 20 people. Eligible participants included nurses, pharmacists, or physicians (with MD and DO degrees) who self-reported at least three contraceptive visits in the previous month. Surveys were distributed online, excluding professionals not meeting inclusion criteria. Respondents were incentivized to complete the survey through raffle entry for a gift card of $250.
The survey opened in May 2022 for 6 months, yielding 344 complete responses. We reviewed demographics and kept the survey open for another month, with targeted recruitment again through listservs from states with limited responses to ensure geographic diversity, resulting in an additional 78 complete surveys. Surveys with less than 75.0% completion (n=146) were excluded.
Among the respondents, 70.1% (n=296 of 422) expressed interest in follow-up surveys and interviews. Participants who had viewed the Clinical Training Center for Sexual and Reproductive Health subcutaneous DMPA toolkit (n=153) were excluded from the follow-up cohort because the study design aimed to expose participants to the toolkit and to reassess readiness for provision (results forthcoming). Sensitivity analyses compared demographics between the 153 excluded and the remaining 143 respondents. Forty participants were selected at random with a number generator. Thirty-four secondary surveys and interviews were completed. We stopped reaching out to participants when theoretical saturation was reached with the interviews. Sensitivity analysis of the 34 participants who were selected for random follow-up compared with the participants not selected for follow-up interview and survey was conducted to show that those who agreed to follow-up did not differ from the overall cohort and did not differ from the group who accepted interviews and had not viewed the toolkit previously. Follow-up surveys and 1-hour interviews (Appendix 2 and 3, respectively, http://links.lww.com/AOG/E482) were conducted between September 20, 2022, and April 19, 2023, and interviewees were compensated for their time with a $100 gift card. Theoretical saturation was approximated after 34 interviews.^23^
Researchers used inductive–deductive framework to analyze the transcripts individually, noted what stood out to them, and then compared the transcripts until common themes were found among researchers and transcripts across patient, professional, institutional, and systemic domains, in line with previous studies on health care implementation barriers.^22^ Discrepancies in coding were adjudicated by consensus (less than 5.0%).^23^ Barriers and facilitators were categorized across domains (patient, professional, institution, and system), in line with previous studies that outline barriers for health care implementation.^22^
Statistical analyses were performed with R 4.2.1, with χ^2^ tests for categorical variables and independent-sample t tests for continuous variables. A value of P<.05 was considered statistically significant. Descriptive statistics summarized respondent characteristics and practice settings. Categorical variables are presented as frequencies and percentages, and continuous variables are summarized as mean±SD. Significant factors associated with awareness and lack of awareness of subcutaneous DMPA for user administration were identified through bivariate analyses. Factors of interest included professional sex, age, degree, specialty, fellowship training, years practicing, contraceptive visit quantity per month, percent of patient population with pregnancy capacity, institution of practice, Title X funding status, commonness of DMPA among patient population, geographic location, and insurance coverage. We used χ^2^ tests for categorical variables, Fisher exact tests when cell count was less than five, and independent-sample t tests for continuous variables. If normality assumption failed for t tests, nonparametric tests were applied. Percentages or averages reflect the proportion or means of respondents within each category.
RESULTS
Data were collected from a geographically diverse sample of contraceptive experts across the United States and its territories, with responses from all states except South Dakota. Professional demographics and practice characteristics are detailed in Table 1 and Figure 1. Responses to the surveys included 388 that were fully completed and 34 that were 76.0–90.0% completed. Excluded surveys consisted of 16 with 33.0–68.0% completion and 130 with less than 17.0% completion. The response rate was 74.3% conservatively (422 of 568) or 77.1% less conservatively (438 of 568). Sensitivity analysis of survey completion status performed with χ^2^ tests determined no differences in completion rates across age (less than 45 years vs 45 years or more, P=.1634), sex (female vs nonfemale, P=.2478), or race (White vs non-White, P=.5411). This implies survey completion was consistent across demographic groups, supporting the robustness of the results and reducing bias in participation. Similarly, no differences emerged with sensitivity analyses regarding the participants chosen for follow-up compared with the initial cohort.
Geographic diversity of participants. Responses were collected from every state in the United States except South Dakota. Only one response was received from Arkansas, Northern Mariana Islands, Delaware, Marshall Islands, New Hampshire, and Oklahoma. The largest number of responses came from California, Washington, New York, Illinois, Pennsylvania, North Carolina, Oregon, Massachusetts, Louisiana, New Jersey, and New Mexico.
A total of 79.4% of respondents were aware of subcutaneous DMPA for user administration, with 52.0% learning about it during the COVID-19 pandemic (2020–2022). Despite awareness, only 34.8% prescribed subcutaneous DMPA for user administration, and 76.9% of these professionals began prescribing after 2019. This highlights barriers between awareness and provision.
Professional awareness was significantly associated with completing a reproductive health fellowship, obstetrics and gynecology specialization, higher contraceptive visit volumes, urban practice settings, Title X funding, working at Planned Parenthood or freestanding reproductive health clinics, and higher proportions of pregnancy-capable patients. Awareness was inversely associated with internal medicine specialization, pharmacy practice, and having more contraceptive options available (Table 2).
Provision of subcutaneous DMPA for user administration was significantly associated with sex and state political environments. Male and gender-diverse professionals were more likely to prescribe, whereas cisgender female professionals were more likely to be aware but not prescribe (P<.001). Professionals in abortion-hostile or middle-ground states, according to Guttmacher Institute's characterization of policy landscapes,^24,25^ were less likely to prescribe if aware of the option (P=.05). Institutional workflows and Medicaid/private insurance coverage for subcutaneous DMPA were significant facilitators of prescribing (P<.001) (Table 3).
Professionals aware of subcutaneous DMPA for user administration identified the top barriers to prescribing: lack of patient awareness, limited access to professional education material, and electronic medical record limitations. Professionals prescribing subcutaneous DMPA noted financial barriers and lack of staff support/time for counseling. Professionals predicted 17.3% (CI, 95.0%) of patients not on contraception and 43.7% (CI, 95.0%) of those using intramuscular DMPA would be interested in user administration.
Follow-up interviews revealed perceived patient barriers, including injection schedules and needle fears; professional barriers such as lack of awareness and limited time for injection education; institutional barriers, including lack of standardized workflows; and systemic barriers such as FDA approval status, pharmacy stock issues, and insurance gaps. Facilitators included telehealth visits, mail-order systems, and reminder systems. Illustrative professional quotes regarding barriers and facilitators are listed in Table 4. The most prevalent perceived barriers were at the perceived patient level (n=7) followed by professional level (n=5) with fewer but important institutional (n=2) and systemic (n=3) barriers.
Professionals identified several perceived patient-level barriers to user administration of subcutaneous DMPA. Although 85.8% of professionals believed subcutaneous DMPA for user administration was suitable for their patients, fewer than half prescribed it. Interviews highlighted professional assumptions about patient suitability such as patient fear of needles, with biases influencing counseling practices. Facilitators addressing memory challenges included reminder systems, although only 31.5% of prescribing professionals used them. Professionals suggested educational resources detailing safe injection techniques and schedules such as online materials or pamphlets to improve patient confidence.
All interviewees noted lack of awareness among general health care professionals as a significant barrier to expanding the prescribing of subcutaneous DMPA for user administration. Professionals emphasized the need for education through workshops, continuing education courses, publications, newsletters, and patient outreach. Only 39.7% of prescribing professionals discussed subcutaneous DMPA at every contraceptive visit, and 34.2% limited discussions to patients already using DMPA or seeking progestin-only methods. Professional biases further restricted counseling about this option.
Institutional barriers included the absence of standardized workflows for prescribing subcutaneous DMPA for user administration. Structured workflows emerged as a significant facilitator. Professionals also highlighted the time needed to teach self-injection techniques and suggested delegating injection education to nurses or support staff. Pregnancy testing requirements varied, with 55.0% of professionals allowing patients to self-report test results, 15.2% preferring to personally verify a negative pregnancy test, and 18.7% requiring institutional verification.
Telehealth visits were identified as key facilitators, with 81.8% of professionals offering them to address patient barriers. However, only 19.0% of prescribing professionals conducted synchronous telehealth visits, and 24.6% offered asynchronous visits for injection counseling. Most professionals preferred in-person visits for the first injection, with 33.7% observing the patient's first injection and 22.7% administering it directly. Professionals also noted mail-order systems as facilitators, although only 8.4% of Title X clinics and 4.3% of non–Title X clinics offered this option.
State- and government-level barriers included the FDA not approving subcutaneous DMPA for user administration but only for professional administration, pharmacy stock limitations, and economic barriers, including lack of insurance coverage. Professionals expressed greater readiness to prescribe when insurance covered the cost. Systemic facilitators included expanded insurance coverage, which increased professional confidence in counseling patients.
DISCUSSION
This national study of contraceptive experts highlights a significant gap between awareness and provision of subcutaneous DMPA for user administration. Although 79.4% of contraceptive experts are aware of this option, fewer than half actively prescribe it, consistent with findings from prior studies.^18^ General practitioner awareness is likely even lower, emphasizing the importance of targeted education for nonspecialists.
Expanding access to subcutaneous DMPA requires addressing barriers between awareness and provision. Sex differences in provision may reflect the limited number of male and gender-diverse contraceptive experts in the field and the likelihood that they are more inclined to seek out and advocate for alternative contraceptive options that support patient autonomy than the majority of professionals. State political environments also influence provision, underscoring the importance of policy supporting contraceptive access, particularly in abortion-hostile states.^26–29^
Professional-perceived patient-level barriers such as self-injection fears often stem from professional biases rather than actual patient limitations; previous studies indicate that needle fears are contextual and decrease over duration of use.^10,13^ Needle fears can be mitigated through guided instruction during the first injection and educational materials.^10,21^ Professional bias in assessing patient suitability influences counseling practices and perpetuates limited patient awareness of this option because professionals are a key conduit to information about contraceptive options.^30,31^ Expanding access to subcutaneous DMPA is particularly important for minoritized populations, who often prefer autonomous contraceptive methods; overcoming professional misconceptions is critical for equitable access.^18,32,33^ A prior study found only 1 in 488 professionals used DMPA themselves compared with 41.7% who used long-acting reversible contraception, suggesting that low personal use of DMPA among health care professionals may contribute to its underutilization.^34^ Concerns about pregnancy testing before initiation can be addressed by recommending self-monitoring for pregnancy symptoms or home testing.
Institutional barriers such as the absence of standardized workflows complicate implementation. Toolkits addressing workflows, billing, advocacy, patient education, and counseling can help overcome these barriers. A toolkit designed to assist professionals with workflows, billing, advocacy, patient education, and counseling was identified to address these institutional barriers.^35^
Finally, FDA approval for subcutaneous DMPA for self-administration is a key policy and system-level barrier. Approval would increase professional confidence and expand insurance coverage, reducing economic barriers. Increased demand through expanded prescribing could also improve pharmacy stock availability, further enhancing access.
This is the only national survey of professional awareness and provision of subcutaneous DMPA for user administration in the United States. Strengths of this study include assessment of populations both aware and unaware and both actively prescribing and not prescribing subcutaneous DMPA for user administration, allowing assessment of barriers between awareness and provision. Because experts in contraception were targeted, this large sample of professionals who are aware of subcutaneous DMPA option could assess for trends in knowledge, provision, and practices, as well as barriers and facilitators to provision. Generalizability, however, is limited given its inclusion of only contraception experts, and although the geographic representation in this study was widespread, limitations with missing data from certain U.S. states and territories remained.
Expanding access to subcutaneous DMPA for user administration requires reducing professional biases through education initiatives, developing standardized workflows, and increasing insurance coverage. Further research demonstrating improved continuation rates and long-term viability may support FDA approval, opening additional opportunities for access. Addressing barriers across all levels will empower patients with greater control over their reproductive health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nguyen AT Curtis KM Tepper NK Kortsmit K Brittain AW Snyder EM U.S. medical eligibility criteria for contraceptive use. MMWR Recomm Rep 2024;73:1–126. doi: 10.15585/mmwr.rr 7304 a 1PMC 1131537239106314 · doi ↗ · pubmed ↗
- 2Gavin L Pazol K Ahrens K. Update: providing quality family planning services—recommendations from CDC and the U.S. office of population affairs. MMWR Morb Mortal Wkly Rep 2017;66:1383–5. doi: 10.15585/mmwr.mm 6650 a 429267259 PMC 5751580 · doi ↗ · pubmed ↗
- 3WHO consolidated guideline on self-care interventions for health: sexual and reproductive health and rights. World Health Organization; 2019. Accessed November 1, 2025. https://ncbi.nlm.nih.gov/books/NBK 544164/31334932 · pubmed ↗
- 4Curtis KM Nguyen A Reeves JA Clark EA Folger SG Whiteman MK. Update to U.S. selected practice recommendations for contraceptive use: self-administration of subcutaneous depot medroxyprogesterone acetate. MMWR Morb Mortal Wkly Rep 2021;70:739–43. doi: 10.15585/mmwr.mm 7020 a 234014910 PMC 8136426 · doi ↗ · pubmed ↗
- 5Burke HM Ridgeway K Murray K Mickler A Thomas R Williams K. Reproductive empowerment and contraceptive self-care: a systematic review. Sex Reprod Health Matters 2021;29:2090057. doi: 10.1080/26410397.2022.209005735892261 PMC 9336472 · doi ↗ · pubmed ↗
- 6Kennedy CE Yeh PT Gaffield ML Brady M Narasimhan M. User-administration of injectable contraception: a systematic review and meta-analysis. BMJ Glob Health 2019;4:1–13. doi: 10.1136/bmjgh-2018-001350 PMC 652876831179026 · doi ↗ · pubmed ↗
- 7Beasley A White KO Cremers S Westhoff C. Randomized clinical trial of self versus clinical administration of subcutaneous depot medroxyprogesterone acetate. Contraception 2014;89:352–6. doi: 10.1016/j.contraception.2014.01.02624656555 PMC 4086940 · doi ↗ · pubmed ↗
- 8Burke HM Mueller MP Perry B Packer C Bufumbo L Mbengue D Observational study of the acceptability of Sayana® press among intramuscular DMPA users in Uganda and Senegal. Contraception 2014;89:361–7. doi: 10.1016/j.contraception.2014.01.02224631328 · doi ↗ · pubmed ↗