Rapid Improvement in Consciousness After Low-Dose Ketamine in a Patient With Acute Confusion: A Case Report
Waleed Khalid Khalafallah Khalid, Hind Abdelazim Mirghani Ibrahim, Ibtisam Ahmed Abdullah Al Hoqani

TL;DR
A patient with acute confusion regained full consciousness quickly after a low dose of ketamine, suggesting potential neurocognitive benefits.
Contribution
Reports a case where ketamine rapidly reversed acute confusion, suggesting new clinical applications beyond sedation.
Findings
A 66-year-old patient regained full consciousness within 45 minutes of receiving 40 mg intravenous ketamine.
No other sedatives or interventions were administered during the observed improvement.
The findings suggest ketamine may have neurocognitive effects that could reverse acute confusion in certain cases.
Abstract
Ketamine, widely used for procedural sedation, may possess underrecognized neuroprotective and cognitive-modulating effects. We report the case of a 66-year-old female patient who presented with acute confusion (Glasgow Coma Scale (GCS) 12/15; E3V4M5), likely secondary to a urinary tract infection. Remarkably, she regained full consciousness (GCS 15/15; E4V5M6) within 45 minutes of receiving 40 mg of intravenous ketamine for nasogastric tube insertion. No other sedatives or interventions were administered during this period. This observation raises the possibility that ketamine may play a role in rapidly reversing acute confusion and enhancing arousal in select clinical scenarios. While anecdotal, such findings align with emerging literature and warrant further exploration of ketamine’s neurocognitive effects beyond its established indications.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
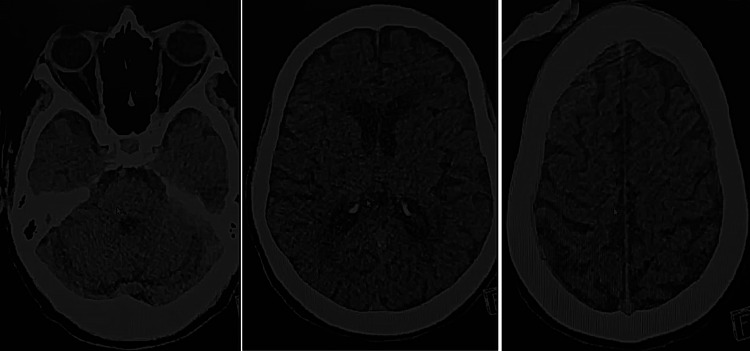 Figure 1
Figure 1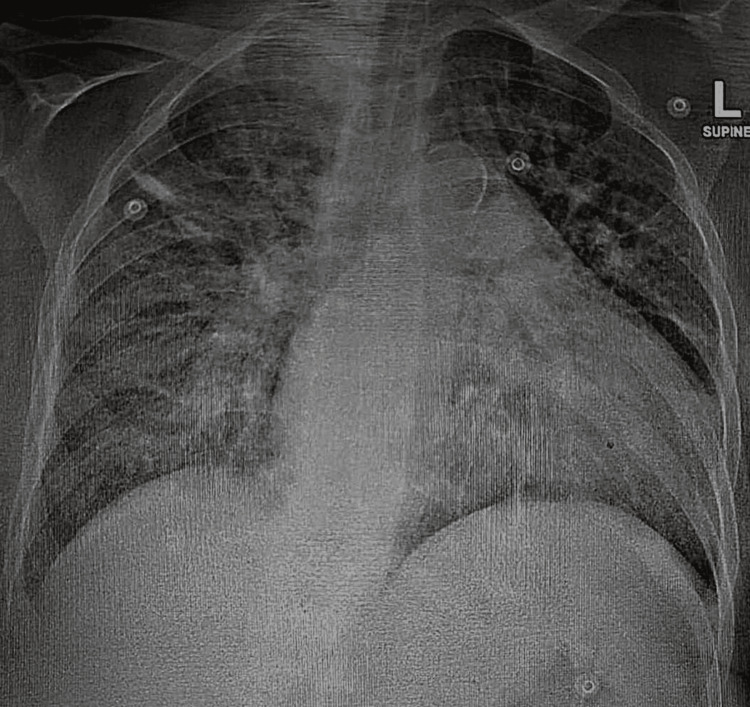 Figure 2
Figure 2| Parameter | Patient Value | Reference Range |
| Haemoglobin in Blood | 11.7 g/dL | 11-14.5 |
| White Blood Cells in Blood | 6.00x103/uL | 2.4 - 9.5 |
| Platelet count in Blood | 140x103/uL | 150 - 450 |
| Red Blood cells | 3.38x106/uL | 4.1 - 5.4 |
| Haematocrit of Blood | 34.5 % | 34 - 43 |
| Mean Cell Volume | 102.1 fL | 78-95 |
| Mean Cell Hemoglobin | 34.6 pg | 26 - 33 |
| RBC distribution width | 13.1 % | 11.5 - 16.5 |
| Neutrophils # in Blood | 3.90x103/uL | 1-4.8 |
| Lymphocytes # in Blood | 1.16x103/uL | 1.2 - 3.8 |
| Eosinophils # in Blood | 0.22x103/uL | 0 -. 5 |
| Monocytes # in Blood | 0.66x103/uL | .1 - 1.3 |
| Basophils # in Blood | 0.06x109/L | 0 - .2 |
| Mean Cell Hb Conc | 33.9 g/dL | 31 - 35 |
| Mean Platelet Volume in Blood | 11.3 fL | 7 - 10.5 |
| Lactate in Serum/Plasma | 1.40 mmol/L | .5 - 2.2 |
| C-Reactive Protein in Serum | 1.30 mg/L | 0 - 5 |
| Aerobic Blood Culture | No bacterial growth | |
| Anaerobic Blood Culture | No bacterial growth | |
| Urine Culture | No bacterial growth | |
| White Cells in Urine | 20 cells/cumm | 0 – 5 cells/μL |
| Red Cells in Urine | 24 cells/cumm | 0 – 3 cells/μL |
| Epithelial cells in Urine | 4 /uL | 0 – 5 cells/μL |
| Casts in Urine | NIL/HPF | None seen |
| Crystals in Urine | NIL | None seen |
| Bacteria in Urine | NIL | None seen |
| Yeast in Urine | NIL | None seen |
| Urine Analysis | ||
| Leukocytes (White Cells) | + | Negative |
| Erythrocytes (Red Cells) | Trace | Negative |
| Glucose in Urine by Test | NIL | Negative |
| Bilirubin in Urine | NIL | Negative |
| pH of Urine | 7.5 | 4.5 – 8.0 |
| Ketones in Urine | Negative | Negative |
| Specific Gravity of Urine | 1.010 | 1.005 – 1.030 |
| Nitrite in Urine | NIL | Negative |
| Protein in Urine | +++ g/L | Negative |
| Urobilinogen in Urine | Negative | Negative |
| Cell count & Differential in Body Fluid (CSF), Panel | ||
| White Blood Cells CSF | 3/uL | 0 – 5 cells/μL |
| Polymorphonuclear cells % CSF | 33 % | 0 – 6% |
| Mononuclear cells % in CSF | 67 % | 94 – 100% |
| Red Blood Cells in CSF | 1x103/UL | 0 – 10 cells/μL |
| Gram-negative Bacilli | Not seen | Not seen |
| Gram-negative Cocci | Not seen | Not seen |
| Gram-positive Cocci | Not seen | Not seen |
| Gram-positive Bacilli | Not seen | Not seen |
| Yeast Cells | Not seen | Not seen |
| Site/Type of Specimen | LP CSF | |
| Appearance of Specimen | Clear | Clear |
| Gram Film | No organisms seen | |
| CSF Culture | No bacterial growth | |
| Protein in CSF | 70.01 mg/dL | 15 - 45 |
| Glucose in CSF | 2.92 mmol/L | 2.22 - 3.89 |
| Ammonia in Plasma | 16.50 umol/L | 11 - 51 |
| Urea in Serum/Plasma | 13.9 mmol/L | 2.7 - 8.07 |
| Creatinine in Serum/Plasma | 587.84 umol/L | 44 - 80 |
| Sodium in Serum/Plasma | 133.37 mmol/L | 136 - 145 |
| Potassium in Serum/Plasma | 4.26 mmol/L | 3.5 - 5.1 |
| Chloride in Serum/Plasma | 95.95 mmol/L | 98 - 107 |
| eGFR.MDRD | 7 mL/minute/1.73 m2 | 90 - 120 |
| Bilirubin Total in Serum | 13.18 umol/L | 3 - 21 |
| Protein Total in Serum/PI | 65.52 g/L | 64 - 80 |
| Alanine Transaminase in serum | 7.09 U/L | 0 - 33 |
| Alkaline Phosphatase in serum | 55.70 U/L | 35 - 104 |
| Albumin in Serum/Plasma | 40.40 g/L | 35 - 52 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTreatment of Major Depression · Intensive Care Unit Cognitive Disorders · Anesthesia and Sedative Agents
Introduction
Ketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist, is widely recognized as a versatile drug in emergency medicine. It is commonly used for sedation, analgesia, asthma exacerbation management, seizure control, rapid sequence intubation (RSI) in hypotensive patients, awake intubation, and cerebroprotection in head trauma. Ketamine’s diverse therapeutic applications have made it a favorite among emergency physicians. Traditionally, ketamine has been widely used in emergency care for procedural sedation, analgesia, reduction of dislocations, burn dressing changes, and as an adjunct in the management of seizures and severe asthma. These diverse effects are mediated through NMDA receptor antagonism. In addition to these established uses, emerging literature highlights its potential in enhancing cognition, reducing delirium, improving levels of consciousness, and treating major depressive disorder resistant to standard therapy [1-5]. Ketamine has also been studied for its potential to reduce postoperative delirium and cognitive decline, especially in elderly surgical patients [6,7]. This case illustrates ketamine’s surprising neuroactivating effect in the context of acute confusion.
Case presentation
A 66-year-old female patient with end-stage renal disease on regular haemodialysis, breast cancer on hormonal therapy, long-standing hypertension, and a history of recurrent urinary tract infections (UTIs) presented to the Emergency Department (ED) with acute confusion characterised by fluctuating attention, severe disorientation to time, place, and person, impaired comprehension, and marked agitation. Her symptoms had been gradually progressive over approximately 26 hours. The confusion had progressed gradually. On arrival, her Glasgow Coma Scale (GCS) was 12/15 (E3V4M5).
Vital signs showed a blood pressure (BP) of 195/85 mmHg, heart rate (HR) 81 beats per minute, respiratory rate (RR) 18 breaths per minute, temperature 38.1°C, and oxygen saturation (SpO₂) of 96% on room air. Neurological examination showed marked agitation and disorientation to time, place, and person. Cranial nerves were grossly intact. Muscle tone was normal, but power could not be reliably assessed due to poor cooperation. Deep tendon reflexes were normal, and there were no signs of meningeal irritation or focal neurological deficits. Chest auscultation was clear, and heart sounds were normal.
Urinalysis revealed leukocytes (+), and urine microscopy showed 20 WBCs per cumm, consistent with an acute UTI, and her fever (38.1°C) supported this impression [8]. Cerebrospinal fluid (CSF) analysis was clear, with normal glucose and no organisms on Gram stain. A non-contrast CT of the head showed no acute intracranial pathology (Figure 1). The CT findings support that the patient’s confusion was not due to an acute structural brain lesion.
Non-contrast CT Head (Axial Slices)Three axial non-contrast CT images demonstrating no acute intracranial pathology.
The official radiology report for the CT scan (Figure 1) indicated no acute intracranial pathology. Although the study was mildly degraded by motion artefact, the radiologist noted only age-related atrophic changes, chronic small-vessel disease, and a chronic right basal ganglia lacunar infarct. No hemorrhage, mass effect, midline shift, or herniation was present. A small right intraventricular isodense lesion was described without associated hydrocephalus or ventriculomegaly. Overall, there was no CT evidence of an acute intracranial insult.
Initial laboratory investigations included complete blood count, renal function tests, liver panel, electrolytes, C-reactive protein (CRP), and ammonia. These are detailed in Table 1. Findings were consistent with her baseline chronic renal impairment, with no significant new derangements. A diagnosis of acute confusion secondary to UTI was considered.
Due to significant agitation, poor cooperation, and inability to take oral medications for over 24 hours, intravenous ketamine, 40 mg (0.5 mg/kg based on an estimated body weight of 80 kg), was administered for procedural sedation to facilitate nasogastric tube (NGT) insertion. Over the next 45 minutes, three NGT insertion attempts were made. During this period, the patient became calm enough to allow the NGT attempts. A chest X-ray was subsequently performed to confirm NGT placement and showed no acute pulmonary abnormalities (Figure 2). This was clinically relevant as it excluded pulmonary infection, aspiration, or respiratory pathology as contributors to her altered mental status. No other medications were administered during this period.
Chest X-rayConfirming nasogastric tube position with no acute pulmonary findings.
Remarkably, 45 minutes after ketamine administration, the patient regained full consciousness (GCS 15/15; E4V5M6). She became fully oriented, cooperative, and interacted appropriately. Post-recovery vital signs were BP 197/90 mmHg, HR 82 bpm, RR 18 breaths/min, and SpO₂ >95% on room air.
The patient was subsequently started on intravenous ceftriaxone and resumed oral antihypertensive medications (hydralazine and nifedipine), which gradually controlled her blood pressure. She was later transferred to another facility, where she completed a four-day course of intravenous piperacillin/tazobactam and was discharged fully recovered. No recurrence of confusion was noted during follow-up.
Discussion
The unexpected improvement in this patient's GCS following ketamine administration aligns with emerging literature describing ketamine’s potential neuroactivating effects. This phenomenon has been documented in comparative studies evaluating ketamine versus other sedatives in terms of cognitive outcomes [9], as well as in experimental models of psychiatric and neurological illness [10].
One of the most clinically relevant examples of ketamine’s neurocognitive influence comes from its use in treatment-resistant major depressive disorder (MDD) [11]. Multiple randomized trials and systematic reviews have demonstrated that subanesthetic doses of ketamine can produce rapid and significant antidepressant effects-often within hours-suggesting a direct action on brain circuits involved in mood regulation, cognition, and consciousness [12]. This well-established role in MDD provides a biological and clinical rationale to explore ketamine’s influence on cortical arousal and recovery of consciousness in non-psychiatric contexts.
These findings challenge the traditional view of ketamine solely as a sedative or analgesic and support the hypothesis that ketamine may modulate thalamocortical connectivity, glutamatergic transmission, and cortical responsiveness. Further research is warranted to understand better ketamine’s role in patients presenting with acute confusion, delayed awakening, or impaired consciousness. Its use in critical care settings could potentially extend beyond sedation, facilitating ventilator weaning, early neurocognitive recovery, and even cerebral protection; however, these implications are speculative and based on emerging experimental evidence rather than established guideline recommendations.
This case is not merely an anecdote; it invites clinicians and researchers to explore ketamine's untapped therapeutic roles. It raises important clinical questions and may contribute to the development of future protocols targeting altered mental status and cognitive dysfunction. Ketamine continues to surprise, and its full potential is still being uncovered.
Conclusions
This case describes a striking temporal association between low-dose ketamine and rapid resolution of acute confusion in an elderly patient. Although causality cannot be definitively established from a single report, the timing of neurological improvement following ketamine administration is striking. Emergency physicians should be aware of this possible neuroactivating phenomenon. Further targeted research is warranted to explore ketamine’s broader neurological benefits in emergency and critical care contexts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Impact of ketamine versus propofol for anesthetic induction on cognitive dysfunction, delirium, and acute kidney injury following cardiac surgery in elderly, high-risk patients Ann Card Anaesth Wittwer ED Cerhan JH Schroeder DR Schaff HV Mauermann WJ 2742802620233747052510.4103/aca.aca_106_22PMC 10451121 · doi ↗ · pubmed ↗
- 2Intraoperative ketamine administration to prevent delirium or postoperative cognitive dysfunction: a systematic review and meta-analysis Acta Anaesthesiol Scand Hovaguimian F Tschopp C Beck-Schimmer B Puhan M 118211936220182994709110.1111/aas.13168 · doi ↗ · pubmed ↗
- 3Impact of ketamine and propofol on cognitive function in elderly patients: a systematic review Cureus Van de Vel G Mun S Zia SU Chalasani R Shukla PS Malasevskaia I 017202510.7759/cureus.79091 PMC 1191745840104485 · doi ↗ · pubmed ↗
- 4Effects of subanaesthetic S-ketamine on postoperative delirium and cognitive function in elderly patients undergoing non-cardiac thoracic surgery: a protocol for a randomised, double-blinded, placebo-controlled and positive-controlled, non-inferiority trial (SKED trial)BMJ Open Wei W Zhang A Liu L 012202210.1136/bmjopen-2022-061535 PMC 934503335914911 · doi ↗ · pubmed ↗
- 5Ketamine vs. haloperidol for prevention of cognitive dysfunction and postoperative delirium: a phase IV multicentre randomised placebo-controlled double-blind clinical trial J Clin Anesth Hollinger A Rüst CA Riegger H 1100996820213312030210.1016/j.jclinane.2020.110099 · doi ↗ · pubmed ↗
- 6Intraoperative ketamine for prevention of postoperative delirium or pain after major surgery in older adults: an international, multicentre, double-blind, randomised clinical trial Lancet Avidan MS Maybrier HR Abdallah AB 26727539020172857628510.1016/S 0140-6736(17)31467-8PMC 5644286 · doi ↗ · pubmed ↗
- 7The influence of low-dose s-ketamine on postoperative delirium and cognitive function in older adults undergoing thoracic surgery J Cardiothorac Surg Wang Y Ma B Wang C Wang Y Liu A Hang L 3241920243884985910.1186/s 13019-024-02811-x PMC 11157807 · doi ↗ · pubmed ↗
- 8Delirium risk associated with esketamine, sevoflurane, propofol, and dexmedetomidine: a real-world study based on the FDA adverse event reporting system Eur J Pharmacol Shuai Y Liu Y Yang X Wan Q Zhao J Wang X 177723100020254034831910.1016/j.ejphar.2025.177723 · doi ↗ · pubmed ↗