Syndromic molecular testing in mechanically ventilated patients with severe pneumonia: a supportive diagnostic approach
Tina Uršič, Kaja Erzar, Katja Seme, Darja Keše, Matjaž Jereb, Franc Strle, Miroslav Petrovec

TL;DR
This study compares traditional and rapid molecular tests for diagnosing pneumonia in ICU patients, finding that conventional methods detect more pathogens and allow for antibiotic testing.
Contribution
The study demonstrates that conventional diagnostics outperform commercial molecular panels in detecting pathogens and enabling antimicrobial susceptibility testing in ICU pneumonia patients.
Findings
Conventional diagnostics detected pathogens in 79.1% of patients versus 63.6% with commercial panels.
Conventional methods identified more bacterial and fungal pathogens and allowed antimicrobial susceptibility testing.
Viral pathogens like influenza A and rhinoviruses were frequently detected, highlighting their role in severe pneumonia.
Abstract
Rapid identification of pathogens is critical in severe pneumonia patients for timely therapy in mechanically ventilated intensive care unit patients. Conventional diagnostics are time-consuming. The Allplex Respiratory Panels 1–4 detect 16 viruses and seven bacteria and provide faster results; however, because this molecular assay does not yield viable organisms, antimicrobial susceptibility testing cannot be performed. We compared conventional diagnostics with commercial panels to evaluate diagnostic performance and clinical utility. In this prospective study, a total of 30 bronchoalveolar lavage fluids and 80 tracheal aspirates were obtained from 110 unique ICU patients with severe pneumonia (January 2014 and April 2016). Conventional diagnostics were performed during illness, whereas testing of these specimens by commercial panels was performed retrospectively. Pathogen detection…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
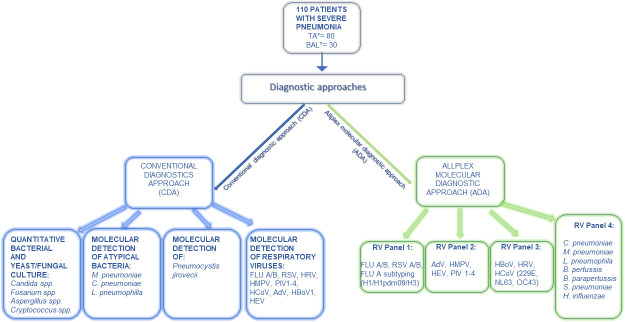 Fig 1
Fig 1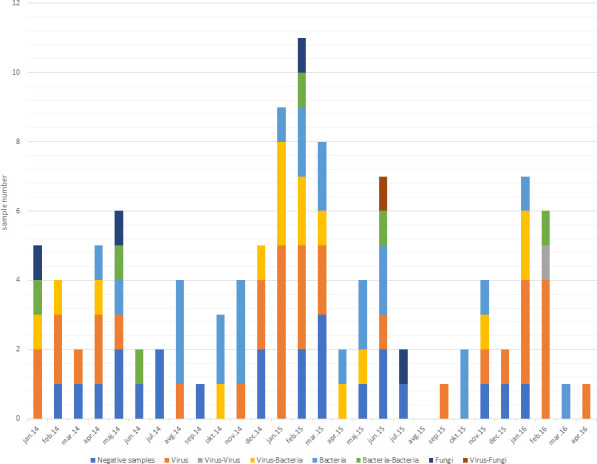 Fig 2
Fig 2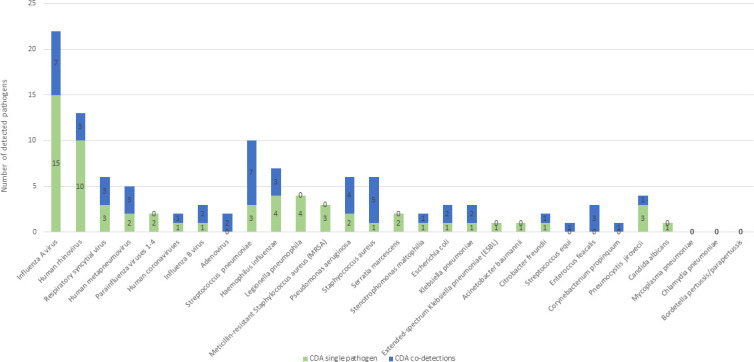 Fig 3
Fig 3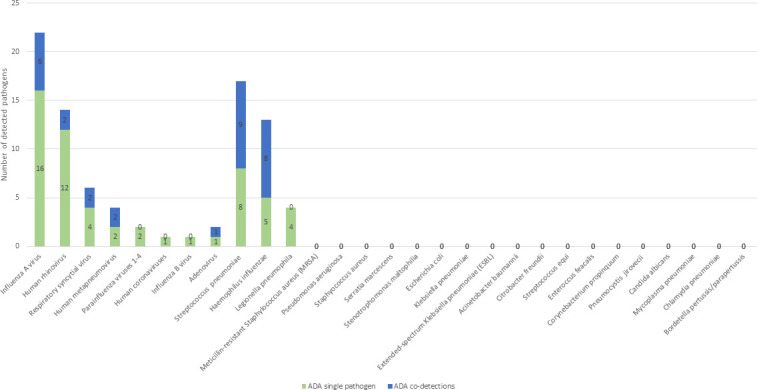 Fig 4
Fig 4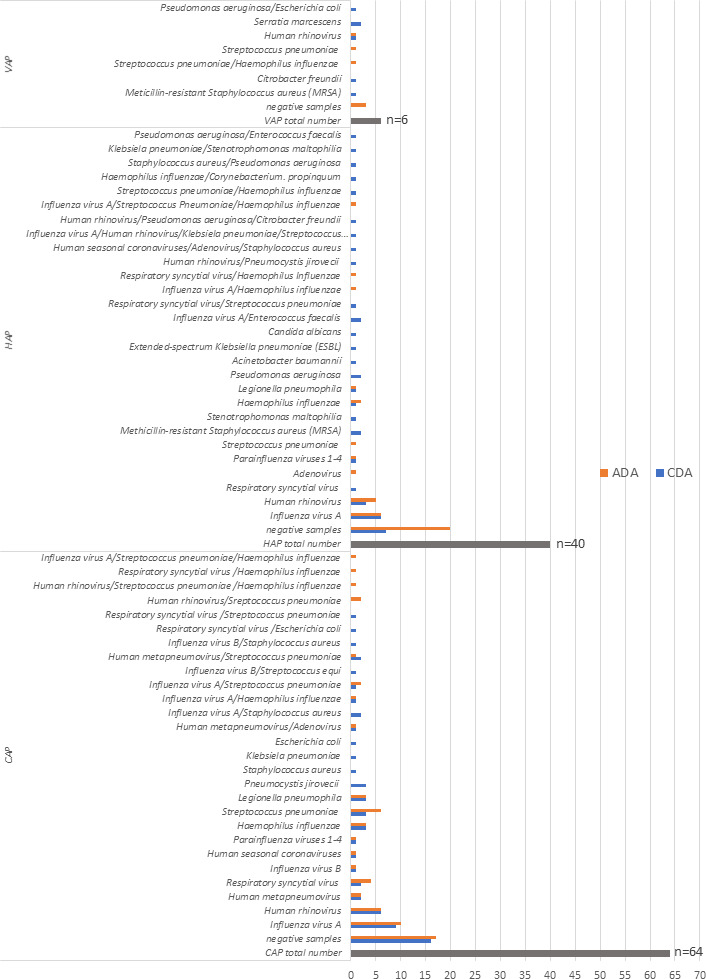 Fig 5
Fig 5| Patient characteristics | Patients, |
|---|---|
| Sex | |
| Women | 31 (29.2) |
| Men | 79 (70.8) |
| Age median (years) | 67 (IQR 57–78) |
| Sample type | |
| Tracheal aspirate | 80 (72.7) |
| BAL | 30 (27.3) |
| Pneumonia type | |
| CAP | 64 (58.2) |
| HAP | 40 (36.4) |
| VAP | 6 (5.4) |
| Characteristics | CDA | ADA |
|---|---|---|
| Patients, | Patients, | |
| Total | 110 (100) | 110 (100) |
| NEGATIVE samples | 23 (20.9) | 40 (36.4) |
| POSITIVE samples | 87 (79.1) | 70 (63.6) |
| Single pathogen detected | 63 (57.3) | 56 (50.9) |
| Single viral pathogens | 34 (31.0) | 39 (35.4) |
| Influenza A virus | 15 (13.6) | 16 (14.5) |
| HRV | 10 (9.1) | 12 (10.9) |
| RSV | 3 (2.7) | 4 (3.6) |
| HMPV | 2 (1.8) | 2 (1.8) |
| PIV 1–4 | 2 (1.8) | 2 (1.8) |
| Human coronaviruses | 1 (0.9) | 1 (0.9) |
| Influenza B virus | 1 (0.9) | 1 (0.9) |
| Adenovirus | 0 | 1 (0.9) |
| Single bacterial pathogens | 25 (22.7) | 17 (15.4) |
| | 3 (2.7) | 8 (7.3) |
| | 4 (3.6) | 5 (4.5) |
| | 4 (3.6) | 4 (3.6) |
| MRSA | 3 (2.7) | NA |
| | 2 (1.8) | NA |
| | 1 (0.9) | NA |
| | 2 (1.8) | NA |
| | 1 (0.9) | NA |
| | 1 (0.9) | NA |
| | 1 (0.9) | NA |
| Extended-spectrum | 1 (0.9) | NA |
| | 1 (0.9) | NA |
| | 1 (0.9) | NA |
| | 0 | 0 |
| | 0 | 0 |
| | 0 | 0 |
| Single yeast pathogens | 4 (3.6) | - |
| | 3 (2.7) | NA |
| | 1 (0.9) | NA |
| Co-detections | 24 (21.8) | 14 (12.7) |
| Virus–bacterium | 16 (14.5) | 12 (10.9) |
| Influenza A virus/ | 2 (1.8) | 0 |
| Influenza A virus/ | 1 (0.9) | 2 (1.8) |
| Influenza A virus/ | 1 (0.9) | 2 (1.8) |
| Influenza A virus/ | 2 (1.8) | 0 |
| Influenza A virus/HRV/ | 1 (0.9) | 0 |
| Influenza A virus/ | 0 | 2 (1.8) |
| Influenza B virus/ | 1 (0.9) | 0 |
| Influenza B virus / | 1 (0.9) | 0 |
| RSV/ | 1 (0.9) | 0 |
| RSV/ | 2 (1.8) | 0 |
| RSV/ | 0 | 2 (1.8) |
| HMPV/ | 2 (1.8) | 1 (0.9) |
| Human coronavirus/adenovirus/ | 1 (0.9) | 0 |
| HRV/ | 0 | 2 (1.8) |
| HRV/ | 1 (0.9) | 0 |
| HRV/ | 0 | 1 (0.9) |
| Bacterium–bacterium | 6 (5.5) | 1 (0.9) |
| | 1 (0.9) | 0 |
| | 1 (0.9) | 0 |
| | 1 (0.9) | 1 (0.9) |
| | 1 (0.9) | 0 |
| | 1 (0.9) | 0 |
| | 1 (0.9) | 0 |
| Virus–virus | ||
| HMPV/adenovirus | 1 (0.9) | 1 (0.9) |
| Virus–fungus | ||
| HRV/ | 1 (0.9) | NA |
| Patient characteristics | CAP | HAP | VAP |
|---|---|---|---|
| Total number of patients; | 64 (58.2) | 40 (36.4) | 6 (5.4) |
| Single pathogen detected by CDA | 37/64 (57.8) | 21 (52.5) | 5 (16.7) |
| Virus | 22 (34.4) | 11 (27.5%) | 1 (16.7) |
| Bacterium | 12 (18.7) | 9 (22.5) | 4 (66.7) |
| Fungus | 3 (4.7) | 1 (2.5) | 0 |
| Co-detections detected by CDA | 11 (17.2) | 12 (30.0) | 1 (16.7) |
| Virus–bacterium | 10 (15.6) | 6 (15.0) | 0 |
| Bacterium–bacterium | 0 | 5 (12.5) | 1 (16.7) |
| Virus–virus | 1 (1.6) | 0 | 0 |
| Virus–fungus | 0 | 1 (2.5) | 0 |
| Positive patients by CDA | 48/64 (75.0) | 33/40 (82.5) | 6/6 (100) |
| Single pathogen detected by ADA | 37/64 (57.8) | 17/40 (42.5) | 2/6 (33.3) |
| Virus | 25 (39.1) | 13 (32.5) | 1 (16.7) |
| Bacterium | 12 (18.8) | 4 (10.0) | 1 (16.7) |
| Fungus | NA | NA | NA |
| Co-detections detected by ADA | 10 (15.6) | 3 (7.5) | 1 (16.7) |
| Virus–bacterium | 9 (14.1) | 3 (7.5) | 0 |
| Bacterium–bacterium | 0 | 0 | 1 (16.7) |
| Virus–virus | 1 (1.5) | 0 | 0 |
| Positive patients by ADA | 47/64 (73.4) | 20/40 (50.0) | 3/6 (50.0) |
- —Javna Agencija za Raziskovalno Dejavnost RShttp://dx.doi.org/10.13039/501100004329
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNosocomial Infections in ICU · Antibiotic Use and Resistance · Pneumonia and Respiratory Infections
INTRODUCTION
It has been estimated that at least 200 million pneumonia cases occur in the world every year (1). In Slovenia, with a population of 2.1 million, each year between 20,000 and 30,000, patients are treated for pneumonia as outpatients, and 5,000 to 7,000 patients are hospitalized due to a severe course of the disease (2). The proportion of hospitalized patients is the highest in preschool children, in patients with underlying chronic diseases, and the proportion is particularly high among those over 80 years of age (1, 3). The fatality rate of patients with community-acquired pneumonia (CAP) requiring hospital treatment is approximately 10% and is much higher (20%–50%) in patients who need intensive care treatment (3). The fatality rate increases with the age of the patients and is especially high in those >80 years old. The occurrence of pneumonia patients fluctuates seasonally and is strongly related to the frequency of influenza (4).
According to the infection source, pneumonia can be divided into CAP, hospital-acquired pneumonia (HAP), and ventilator-associated pneumonia (VAP). The etiology of these entities differs: the most common causative agents for CAP are Streptococcus pneumoniae, respiratory viruses, Haemophilus influenzae, and atypical bacteria such as Mycoplasma pneumoniae and Legionella pneumophila (4); the most frequent causes of HAP are Staphylococcus aureus, Klebsiella pneumoniae, and Pseudomonas aeruginosa (5); and the most frequent causative agents of VAP are P. aeruginosa, S. aureus, Acinetobacter spp., and Stenotrophomonas spp. (5, 6).
Analysis of the etiology of 3,854 adult European patients treated for CAP from 2003 to 2014 showed that 7% of the causes were respiratory viruses, 24% were bacteria, 6% were polymicrobial infections, and 3% were other causes. In contrast, in 60% of patients, no pathogen was detected (1, 3). However, in the last decade, studies using advanced diagnostic methods have confirmed a large proportion of pneumonia associated with viral infections and substantially increased the understanding of the role of viruses as the causative agents of pneumonia (4, 7–9). There is much more information on the etiology of pneumonia for outpatients and hospitalized patients treated at usual departments than for critically ill patients treated in intensive care units (ICUs) (4, 7).
Despite advances in microbiological testing, establishing the etiology of severe pneumonia in mechanically ventilated ICU patients remains challenging. Conventional culture-based diagnostics are time-consuming and frequently yield negative results, particularly after prior antibiotic exposure. Syndromic multiplex PCR panels offer faster pathogen identification, but their performance and clinical utility have mostly been studied in less critically ill populations (10, 11). Real-world data on their application in ICU-acquired or VAP are limited (12). This study addresses this gap by directly comparing a commercially available multiplex PCR panel with comprehensive conventional diagnostic methods in a cohort of critically ill mechanically ventilated patients.
International guidelines for the management of CAP (13) and HAP/VAP (14) primarily recommend culture-based diagnostics and do not yet endorse routine use of multiplex PCR panels in ICU pneumonia. Recent expert reviews suggest that such panels may be considered as adjunctive tools, particularly for early viral detection and antimicrobial stewardship, but emphasize the lack of robust evidence from critically ill populations. By evaluating both diagnostic approaches in severe ICU pneumonia, our study provides novel evidence to inform this debate and clarify the potential and limitations of syndromic panels in this high-risk patient group.
This prospective study assesses the detection of pathogens in lower respiratory tract specimens obtained from critically ill patients with severe pneumonia using the conventional diagnostic approach (CDA) combining bacterial culture and molecular diagnostics of respiratory viruses and atypical bacteria. Furthermore, we aimed to evaluate whether a molecular approach, the Allplex molecular diagnostic approach (ADA; Allplex Respiratory Panel (RP) assays 1–4; Seegene Inc., Korea), is suitable for detecting potential pathogens of pneumonia in critically ill mechanically ventilated patients and to highlight the potential advantages and limitations of the ADA in comparison to the current CDA.
MATERIALS AND METHODS
Study population, inclusion criteria, definitions
The study population consisted of consecutive mechanically ventilated adult patients treated at the ICU of the Department of Infectious Diseases, Ljubljana University Medical Center, between January 2014 and April 2016 for severe CAP, HAP, or VAP.
Pneumonia cases were classified as CAP, HAP, or VAP based on established international guidelines by the Infectious Diseases Society of America, American Society of Microbiology, and American Thoracic Society (13–16). Diagnostic criteria for CAP are clinical presentation, including cough, fever, and radiologically detected lung infiltrate at the beginning of the illness in a community setting.
Diagnostic criteria for HAP are radiologically confirmed lung infiltrate that appeared >48 hours after admission to the hospital in a patient who simultaneously had at least two of the following indicators: body temperature>38.0°C, presence of leukocytosis or leukopenia, or purulent tracheobronchial discharge. Patients with HAP were either transferred to the ICU from other departments due to severe HAP or developed HAP during treatment in the ICU.
Diagnostic criteria for VAP are the formation of a new lung infiltrate or the spread of already known lung infiltrates in a patient that had been mechanically ventilated for >48 hours and had at least two of the following three symptoms: body temperature >38.0°C, presence of leukocytosis or leukopenia, or purulent tracheobronchial discharge.
Microbiological analyses
In this study, mechanically ventilated ICU patients with pneumonia often had more than one lower respiratory tract sample (tracheal aspirate or bronchoalveolar lavage [BAL]) collected during their disease course. For consistency and to avoid repeated measures, we analyzed only the first available lower respiratory tract sample, collected at the time of pneumonia suspicion/diagnosis, using both the CDA and the ADA. The CDA testing was performed in real time while patients were experiencing ongoing clinical symptoms (2014–2016), and the same combination of CDA assays was applied to all patient samples. The ADA testing was performed retrospectively in 2018 using the same raw tracheal aspirate and BAL specimens, which had been stored at −80°C. For ADA testing, nucleic acids were re-extracted from these stored samples before analysis. The diagnostic workflow is depicted in Fig. 1.
Schematic presentation of two diagnostic workflows for mechanically ventilated patients with severe pneumonia. Legend: TA, first tracheal aspirate; BAL*, first bronchoalveolar lavage; FluA/B, influenza A/B virus; RSV, respiratory syncytial virus; HRV, human rhinovirus; HMPV, human metapneumovirus; PIV1−4, parainfluenza viruses 1–4; HCoV, seasonal coronaviruses; AdV, Adenovirus; HBoV1, human bocavirus 1; HEV, human enterovirus; M. pneumoniae, Mycoplasma pneumoniae; C. pneumoniae, Chlamydia pneumoniae; L. pneumophila, Legionella pneumophila; B. pertussis, Bordetella pertussis; B. parapertussis, Bordetella parapertussis; S. pneumoniae, Streptococcus pneumoniae; H. influenzae, Haemophilus influenzae. The left side presents methods and pathogens detected using a CDA, and the right side shows detection using the syndromic ADA.*
Conventional diagnostic approach
Microbiologic diagnostics according to the conventional approach included quantitative bacterial culture. The quality and adequacy of respiratory specimens were assessed by microscopic examination at 100× magnification following Gram staining. Samples were considered acceptable if they contained >25 leukocytes and <10 epithelial cells per field. Samples not meeting these criteria were rejected for diagnostic processing, in line with clinical practice. Established quantitative culture thresholds to distinguish colonization/contamination from true infection were followed. For BAL specimens, ≥10⁴ CFU/mL was considered significant, and for endotracheal aspirates ≥10⁵ CFU/mL, as described previously (17–19). Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (Bruker Daltonics, Bremen, Germany) was used for microbial identification of recovered isolates. Moreover, selective mycology media including Sabouraud dextrose agar and CHROMagar Candida were used for the isolation and identification of Candida species, as well as other clinically important fungi, such as Fusarium spp., Aspergillus spp., and Cryptococcus spp. Additionally, direct Gram staining and India ink staining were performed for the presumptive identification of Cryptococcus spp., whereas direct microscopy with calcofluor white staining was used for the detection of Aspergillus and Fusarium spp. The detection of respiratory viruses—including influenza A and B (flu A/B), respiratory syncytial viruses (RSVs), adenoviruses (AdV), human bocavirus 1 (HBoV1), seasonal coronaviruses (HCoV), human metapneumoviruses (HMPV), parainfluenza viruses 1–4 (PIV 1-4), human rhinoviruses (HRV), and enteroviruses (EV)—was carried out using in-house real-time RT-PCR as described previously (20). M. pneumoniae, L. pneumophila, and C. pneumoniae were detected using the Chla/Myco pneumo and Legio pneumo/Cc R-GENE Kit according to the manufacturer’s instructions (Argene by Biomerieux, France) and Pneumocystis jirovecii using in-house real-time PCR using the primers and probe described previously (21).
Detection of bacteria and viruses using ADA
From BAL and TA samples, nucleic acids were retrospectively re-extracted and tested using Allplex RPs 1, 2, 3, and 4 by Seegene (Seegene Inc., Korea). RP1 was used for detecting FluA/B and RSV; RP2 for AdV, HMPV, PIV1–4, and EV; RP3 for HBoV 1–4, HRV, and seasonal HCoV; and RP4 for bacterial pathogens: Chlamydia pneumoniae, M. pneumoniae, L. pneumophila, Bordetella pertussis, Bordetella parapertussis, S. pneumoniae, and H. influenzae (Fig. 1). Extraction of nucleic acids was performed using the STARMag 96 × 4 Universal Cartridge Kit (Seegene Inc., Korea) using a Microlab NIMBUS instrument, and real-time RT-PCR was performed using the CFX96 real-time PCR system (Bio-Rad, USA). If there was an insufficient patient sample for nucleic acid extraction and subsequent ADA testing, the patient was excluded from the study. During conventional diagnostic analysis, there were no failed sample extractions and no invalid results. In the ADA testing, three samples initially yielded invalid results; these were successfully re-extracted, and ADA was subsequently completed successfully. Syndromic molecular/PCR testing was performed and interpreted blinded to CDA, with data compared only after all analyses were completed to minimize interpretation bias.
Statistics
Continuous variables were summarized using medians and (interquartile) ranges. Student’s t-test was used for continuous variable calculation of the statistical significance (mean Ct values), and categorical variables were presented as frequencies with percentages. Fisher’s exact test was used for calculating the statistical significance of categorical variables.
RESULTS
Basic characteristics of patients with severe pneumonia are presented in Table 1.
A comparison of the CDA and ADA approaches in terms of pathogen detection rates, including co-detections, is presented in Table 2. The CDA showed a higher percentage of respiratory pathogens detected (87/110, 79.1% vs 70/110, 63.6%; P = 0.016). The difference arises from the limited number of bacterial and fungal targets in ADA.
Seasonal pattern of viral pneumonia
Because respiratory viruses tend to follow seasonal patterns, a higher incidence of viral pneumonia was observed in the winter months. This was observed for each season during the study period, from January 2014 to April 2016 (Fig. 2).
Seasonality pattern of severe pneumonia cases. Legend: samples of severe pneumonia patients during the study period are colored depending on the type of pathogen detected, single or co-detections.
Single infections and co-detections in mechanically ventilated patients with severe pneumonia
Combined results, using both the CDA and the ADA, showed that most frequently detected viruses were Flu A and HRV, and the most frequently detected bacteria were H. influenzae, L. pneumophila, and S. pneumoniae. H. influenzae and S. pneumoniae were also most frequently seen in co-detections ([Fig. 3 and 4](#F3 F4)).
Number of pathogens detected using the CDA, including numbers of single and co-detections. Legend: The figure shows pathogen detection (single or co-detections) using the conventional approach.
Number of pathogens detected using Allplex Seegene RPs 1–4, including numbers of single and co-detection by pathogen. Legend: The figure presents pathogens detected (single or co-detections) using the Allplex Seegene molecular diagnostic approach.
Comparison of the two approaches revealed that the ADA missed 14 (12.7%) bacterial single infections and four (3.6%) fungal infections (three P. jirovecii [Ct values: 23.2, 25.4, 29.4]) and one Candida albicans (>10^5^ CFU/mL), as well as 12 (10.9%) co-detections detected using the CDA. However, additional viral single infections were detected by ADA in five (4.5%) in comparison to the current CDA (Table 2 and Fig. 5). Regarding bacteria, using the CDA, S. pneumoniae was detected in 10 patients, whereas using ADA, it was detected in 17 patients ([Fig. 3 and 4](#F3 F4)). The mean Ct value for S. pneumoniae detected by ADA was significantly lower in samples that were positive by both CDA and ADA compared to those positive only by ADA (22.81 vs 28.89; P = 0.001). A similar pattern was seen for H. influenzae detection. It was detected in seven patients using the CDA and in 13 patients using ADA. The mean Ct value for H. influenzae detected by ADA was significantly lower in samples that were positive by both CDA and ADA, compared to those positive only by ADA (21.97 vs 30.53; P < 0.001). Five of seven pneumonia patients who were negative by CDA but positive for S. pneumoniae by ADA and all six patients who were negative by CDA but positive for H. influenzae by ADA had already received antibiotic treatment before sample collection.
Patients with severe pneumonia and pathogens detected by pneumonia type. Legend: CAP, community-acquired pneumonia; HAP, hospital-acquired pneumonia; VAP, ventilator-associated pneumonia. Blue bars represent pathogens detected using the classical diagnostic approach, and orange bars pathogens detected using the ADA.
Using the existing CDA, five multi-resistant bacteria, four S. aureus (MRSA), and one case of K. pneumoniae (extended-spectrum beta-lactamase [ESBL]) were detected; all were missed using the ADA due to a lack of associated targets for these organisms.
Detected pathogens by pneumonia type
Of 110 patients, 64 had severe CAP. Using the CDA, a single virus was detected in 22 patients (34.4%) with Flu A (n = 9) and HRV (n = 6), accounting for 15/22 (23.4%) of these single virus infections. Single bacterial infections were detected in 12 (18.7%) patients, with S. pneumoniae (n = 3), H. influenzae (n = 3), and L. pneumophila (n = 3) accounting for the majority of single bacterial infections (Table 3). Three patients (4.7%) with CAP, with three single fungal infections caused by P. jirovecii, were detected (Fig. 5). Of the 11 cases in which several pathogens were detected together, a virus and a bacterium occurred together in 10 cases, with more than half of these cases containing combinations of Flu A/B virus, HMPV, or RSV with S. pneumoniae, H. influenzae, or S. aureus (Fig. 5).
Using the ADA, single virus infections were found in 25 (39.0%) patients with Flu A (n = 10) and HRV (n = 6), corresponding to 16 (25.0%) of the single viral infections. Single bacterial infections were again identified in 12 (18.8%) patients, with S. pneumoniae (n = 6), H. influenzae (n = 3), and L. pneumophila (n = 3) accounting for all 12 single bacterial infections. In contrast, more than one pathogen was detected in 10 patients (15.6%), with nine cases involving a combination of viruses and bacteria. Flu A and HRV were most frequently detected together with S. pneumoniae and H. influenzae. Overall, the two approaches were comparable in identifying the potential cause of CAP (48/64, 75% vs 47/64, 73.4% for the CDA and the ADA, respectively).
In 40 patients with severe HAP, the CDA identified single viral infections in 11 patients (27.5%), with Flu A (n = 6) and HRV (n = 3) accounting for 9 (22.5%) of these cases (Table 3). Single bacterial infections were detected in nine patients (22.5%), most frequently methicillin-resistant S. aureus (MRSA) (n = 2) and P. aeruginosa (n = 2), which together accounted for 4 (10 %) single bacterial infections. A single fungal infection with C. albicans was detected in one patient (2.5%; Fig. 5). Twelve patients (30.0%) had multiple pathogens, including six virus–bacterium combinations and five bacterium–bacterium combinations. The most common virus–bacterium combinations were Flu A or HRV with S. pneumoniae or Enterococcus faecalis. Bacterium–bacterium combinations included H. influenzae, P. aeruginosa, S. aureus, K. pneumoniae, Stenotrophomonas maltophilia, Citrobacter freundii, and Corynebacterium propinquum. In addition, virus–fungus co-detection (HRV and P. jirovecii) was observed.
Using the ADA, single viral infections were detected in 13 patients (32.5%), with Flu A (n = 6) and HRV (n = 5) accounting for 11 (27.5%) of these cases. Single bacterial infections were detected in four patients (10.0%), including H. influenzae (n = 2), S. pneumoniae (n = 1), and L. pneumophila (n = 1; Table 3). Virus–bacterium combinations were detected in three patients (7.5%), with H. influenzae present in all cases and Flu A in two cases.
Overall, Flu A and HRV were the most frequently detected viruses in both approaches. In CDA, the most common bacteria were MRSA and P. aeruginosa, whereas H. influenzae was predominant in the ADA. The etiology of HAP was more commonly identified with CDA than with the ADA (33/40, 82.5% vs 20/40, 50.0%; P = 0.004) (Table 3 and Fig. 5). Six patients had severe VAP (Fig. 5). The CDA detected a single viral infection (HRV) in one patient, single bacterial infections in four patients (Serratia marcescens n = 2, C. freundii n = 1, and MRSA n = 1), and a bacterium–bacterium combination (P. aeruginosa and E. coli) in one patient. The etiological pathogen was thus identified in all six patients (100%). With the ADA, pathogens were only detected in three patients (50%): in one with HRV, in one with S. pneumoniae, and in one with a joint detection of S. pneumoniae and H. influenzae (Fig. 5; P = 0.1818).
DISCUSSION
Although modern diagnostic methods have considerably improved the etiological detection of microbial infections, pneumonia diagnosis remains challenging due to the wide range of potential pathogens and difficulties in obtaining high-quality samples. Combining classical bacteriology, serology, antigenic, and molecular testing allows pathogen identification in 38%–76% of pneumonia cases (8, 9, 22–24), which is not optimal. Furthermore, such an approach is labor-intensive and time-consuming, often requiring days for definitive results. While new diagnostic approaches are needed, they should be critically assessed against conventional methods (25).
Several commercial multiplex molecular RPs are now available for detecting respiratory pathogens (25–28).
This study evaluated the Allplex Seegene RP 1–4 kits (ADA) and compared the results with our CDA in severely ill mechanically ventilated ICU patients with pneumonia. To our knowledge, the ADA, which detects 16 viral and seven bacterial pathogens, has not been evaluated in such a patient group.
Our CDA identified a potential etiologic pathogen in 79.1% of cases, supporting the value of combining molecular and conventional methods, which may improve detection by 20%–50% (29, 30). Testing the same specimens, the ADA identified the causative agent(s) in 63.6% of cases within 6 hours. Despite the faster turnaround, 15.5% of cases diagnosed by the CDA remained undetected using the ADA due to its limited bacterial range. Specifically, the ADA does not include several common HAP/VAP pathogens such as S. aureus, K. pneumoniae, other Enterobacteriaceae, and P. aeruginosa, nor does it include fungal pathogens (1, 8, 9, 22, 29). As a result, several bacterial infections (including five multidrug-resistant bacteria) and four fungal infections, detected using the currently used CDA, were missed by the ADA. Etiological diagnosis is important for appropriate treatment in general and may be critical in the management of patients with severe pneumonia in the ICU (31, 32).
Using the CDA combined with molecular testing, we identified viral pathogens in 47.3% of cases, with single-virus infections in 31.0%. As expected, seasonal occurrence of viral pneumonia was observed (Fig. 2) (7, 22–24, 29, 33). Influenza A virus was the most common viral cause, accounting for 20% of pneumonia cases. Bacteria were found in 42.7% of cases, with single bacterial infections in 22.7%. S. pneumoniae and H. influenzae were detected most frequently (9.1% and 6.4%, respectively), consistent with previous reports (3, 32, 34, 35). In CAP, bacteria usually account for more than half of the agents identified, although prevalence varies widely (11%–77%) (22–24, 29, 36).
We identified four (3.6%) L. pneumophila cases, all confirmed by urine antigen. We also confirmed three cases of pneumocystis pneumonia in immunocompromised patients with a high fungal burden in a clinical context (two patients after kidney transplantation and one patient with non-Hodgkin’s lymphoma). No atypical bacteria, such as C. pneumoniae and M. pneumoniae, were detected, although they are reported in 3%–15% of CAP (22–24, 29, 33); however, these bacteria are uncommon causes of severe pneumonia. Furthermore, their absence in this study may also be due to our older ICU cohort (median age 67 years). A 10-year Slovenian study reported cyclic M. pneumoniae epidemics every 3–7 years, primarily affecting children and younger adults, with lower prevalence in those over 40 (37–39).
Acute lower respiratory tract infections are often (in 10%–56% of patients) associated with the presence of more than one agent (22–24, 29, 33, 40). In our study, co-detections were found in 21.8% of patients, with virus–bacterium combinations most commonly detected (14.5%). The main viral players in co-infections were influenza A, rhinoviruses, and RSV, whereas S. pneumoniae and H. influenzae were the most common among bacteria, which is in line with a previous report (29). An elegant explanation for virus–bacteria combinations is that having previous viral lower respiratory infections increases susceptibility to bacterial superinfections (7, 40, 41).
The results of this study indicate that the ADA is most suitable for the diagnostics of CAP because by using this approach, we were able to detect etiology in all but one out of 64 cases in which the etiology was demonstrated using the CDA. However, the system is less well designed for HAP. Due to the limited range of pathogens that can be detected using the ADA, the etiologic cause was confirmed significantly less often in comparison to our CDA (20/40, 50% vs 33/40, 82.5%; P = 0.008). A similar trend was also valid for VAP (3/6, 50% vs 6/6, 100%; P = 0.182). On the other hand, molecular tests detected the presence of bacteria more often than bacterial culture. In our study, bacterial culture was positive in only 58.8% of S. pneumoniae cases and 53.8% of H. influenzae cases with a positive Allplex molecular result, respectively. This discrepancy probably reflects the limited sensitivity of the culture, but previous antibiotic treatment may also have reduced the viability of the bacteria and thus the yield of the culture. Detection of bacteria by conventional culture in ICU patients is particularly difficult due to the low bacterial load and frequent prior antibiotic exposure. Antibiotics were administered to 5/7 patients (71.4%) that were positive for S. pneumoniae by the ADA but negative by the CDA and to all six patients (100%) that were positive for H. influenzae by the ADA but negative by the CDA, respectively. Similarly, 11/17 (64.7%) and 10/13 (76.9%) patients positive for S. pneumoniae and H. influenzae by the ADA, respectively, had received antibiotics before sampling. These data suggest that prior antibiotic exposure may have disproportionately reduced the sensitivity of the cultures, biasing the comparison in favor of the ADA. Nevertheless, conventional culture remains essential because it allows for isolate recovery essential for antimicrobial susceptibility testing performance, currently irreplaceable by molecular assays. (15).
Two Conformité Européenne-marked PCR-based tests are Food and Drug Administration-approved for pneumonia diagnosis: the BioFire FilmArray Pneumonia Panel (Biomereux, France), which detects 18 bacteria (including three atypical ones), seven resistance genes, and eight viruses in 90 minutes (27, 42), and the Unyvero Pneumonia Panel (Curetis, Germany), which detects 21 bacteria and one fungal pathogen semi-quantitatively and identifies 15 resistance genes in approximately 5 hours. Both have been evaluated in various settings (42–45) but were unavailable during our study.
In conclusion, in our study on mechanically ventilated patients treated for severe pneumonia in the ICU, our CDA identified a potential pathogen in 79.1% of cases, whereas testing the same specimens using the ADA detected the causative agent(s) in 63.6% of cases. This commercial molecular diagnostic approach proved to be very good in the detection of etiologic pathogens in the subgroup of patients with CAP, but it was less useful in the detection of etiologic pathogens in patients with HAP or VAP due to the limited range of bacterial targets*.* Consequently, in mechanically ventilated patients treated for severe pneumonia in the ICU, the ADA may be best utilized for patients with CAP or due to a short turnaround time (6 hours) as a rapid screening method, which can provide basic information on the same day. The ADA platform was selected as the test comparator in our study because it was the most cost-effective molecular RP available in our hospital. Alternative platforms, such as the Unyvero Pneumonia panel, were prohibitively expensive for evaluation, and the BioFire FilmArray Pneumonia panel was only introduced to the market at the end of 2018. Despite its limited pathogen coverage, the ADA allowed timely results to guide clinical decision-making regarding antibiotic therapy, which was a key priority in our study.
Future studies should explore the clinical interpretation of Ct values in molecular testing, their correlation with culture standards, and how molecular diagnostics could integrate with traditional microbiology to optimize treatment strategies (46). Expanding the range of detectable pathogens in commercial molecular panels, incorporating resistance gene detection, and further shortening turnaround times could strengthen the role of molecular diagnostics and therefore further improve pneumonia management as well as guide antimicrobial therapy more precisely (42).
Recently, metagenomic next-generation sequencing has emerged as a promising tool for pneumonia diagnostics. Its high-throughput capacity and sensitivity allow for improved pathogen identification, particularly in severe pneumonia cases for which conventional methods may be limited (46).
The findings of this study exposed the complementary nature of molecular and CDAs. Molecular methods provide rapid and broad pathogen detection, but conventional techniques remain essential for bacterial culturing and antimicrobial resistance testing. In our hospital setting, a hybrid diagnostic model is implemented by performing the ADA on respiratory specimens at the time of collection, in parallel with conventional quantitative bacterial cultures. Molecular results provide early identification of viral, atypical, and common bacterial pathogens to guide timely antimicrobial therapy, and conventional cultures allow confirmation of bacterial etiology and full susceptibility testing, which is particularly important for critically ill patients. Integration of both results through the laboratory/hospital information system enables ICU clinicians to make informed therapeutic decisions, combining speed and precision in the management of severe pneumonia.
This study has several limitations. First, it was conducted at a single tertiary care center with a regional ICU cohort, which may limit the generalizability of the findings to other settings or patient populations. Second, ADA testing was performed retrospectively and was not available to guide clinical management in real time, which may have influenced both diagnostic yield and interpretation. Third, the study lacked randomization and prospective enrollment, introducing potential selection bias. Fourth, due to its observational design, detailed patient-level outcomes—such as the impact of diagnostic findings on antimicrobial therapy adjustments, length of stay, or mortality—could not be systematically assessed. Finally, although the ADA and CDA approaches were compared using standardized workflows, variability in sample quality, timing of collection, and prior antimicrobial exposure could have affected detection rates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Torres A, Cilloniz C, Niederman MS, Menéndez R, Chalmers JD, Wunderink RG, van der Poll T. 2021. Pneumonia. Nat Rev Dis Primers 7:25. doi:10.1038/s 41572-021-00259-033833230 · doi ↗ · pubmed ↗
- 2Lejko-Zupanc T, Pokorn M. 2015. Pljučnica. In Tomažič J, Strle F (ed), Tiskarna Povše: Združenje za Infektologijo, Slovensko zdravniško društvo, 1th ed
- 3Prina E, Ranzani OT, Torres A. 2015. Community-acquired pneumonia. Lancet 386:1097–1108. doi:10.1016/S 0140-6736(15)60733-426277247 PMC 7173092 · doi ↗ · pubmed ↗
- 4Alimi Y, Lim WS, Lansbury L, Leonardi-Bee J, Nguyen-Van-Tam JS. 2017. Systematic review of respiratory viral pathogens identified in adults with community-acquired pneumonia in Europe. J Clin Virol 95:26–35. doi:10.1016/j.jcv.2017.07.01928837859 PMC 7185624 · doi ↗ · pubmed ↗
- 5Jones RN. 2010. Microbial etiologies of hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia. Clin Infect Dis 51 Suppl 1:S 81–S 87. doi:10.1086/65305320597676 · doi ↗ · pubmed ↗
- 6Huang Y, Jiao Y, Zhang J, Xu J, Cheng Q, Li Y, Liang S, Li H, Gong J, Zhu Y, Song L, Rong Z, Liu B, Jie Z, Sun S, Li P, Wang G, Qu J, Infection Assembly of Shanghai Respiratory Society. 2018. Microbial etiology and prognostic factors of ventilator-associated pneumonia: a multicenter retrospective study in Shanghai. Clin Infect Dis 67:S 146–S 152. doi:10.1093/cid/ciy 68630423049 · doi ↗ · pubmed ↗
- 7Ruuskanen O, Lahti E, Jennings LC, Murdoch DR. 2011. Viral pneumonia. Lancet 377:1264–1275. doi:10.1016/S 0140-6736(10)61459-621435708 PMC 7138033 · doi ↗ · pubmed ↗
- 8Johansson N, Kalin M, Tiveljung-Lindell A, Giske CG, Hedlund J. 2010. Etiology of community-acquired pneumonia: increased microbiological yield with new diagnostic methods. Clin Infect Dis 50:202–209. doi:10.1086/64867820014950 PMC 7107844 · doi ↗ · pubmed ↗