False-negative CMV PCR results due to viral sequence variation: a diagnostic pitfall with the potential for serious consequences
Huanyu Wang, Monica I. Ardura, Sophonie J. Oyeniran, Amy L. Leber

TL;DR
False-negative CMV PCR results due to viral mutations can delay treatment in immunocompromised patients, highlighting the need for improved diagnostic strategies.
Contribution
This case highlights how viral sequence variation can cause false-negative CMV PCR results, leading to delayed treatment.
Findings
Nucleotide mutations in the probe-binding site caused false-negative CMV PCR results in a patient.
False negatives led to delayed detection of CMV DNAemia and delayed antiviral therapy.
Testing with an alternate PCR assay targeting a different gene is recommended when results conflict with clinical data.
Abstract
Cytomegalovirus (CMV) continues to be a significant cause of morbidity and mortality in immunocompromised patients. Nucleic acid amplification tests (NAATs) are the preferred method for both diagnosing CMV infection and monitoring response to antiviral therapy in these patients. The use of a sensitive and specific CMV NAAT is essential to ensure early and reliable detection. A 4-month-old patient with familial hemophagocytic lymphohistiocytosis received an allogeneic hematopoietic cell transplant (HCT). Weekly CMV monitoring before and after HCT was performed using an in-house quantitative CMV PCR assay that targets the CMV UL54 gene. Review of the amplification curves of PCR runs raised concerns about potential false-negative results. Sequencing of the patient sample identified nucleotide mutations within the probe-binding site, confirming the cause of the assay failure. These…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
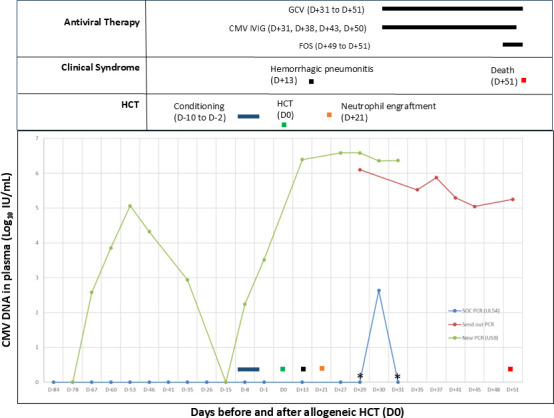 Fig 1
Fig 1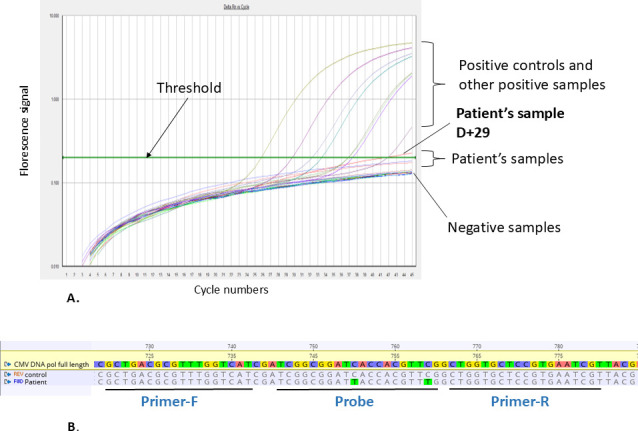 Fig 2
Fig 2| Tests | Manufacturer | Technologies | Specimen type | Target(s) | Selected references |
|---|---|---|---|---|---|
| Abbott RealTime CMV | Abbott Molecular | Quantitative PCR | Plasma | UL34 and UL80.5 genes | ( |
| Alinity M CMV | Abbott Molecular | Quantitative PCR | Plasma and whole blood | UL34 and UL80.5 genes | ( |
| Aptima CMV Quant Assay | Hologic, Inc | Quantitative TMA | Plasma | UL56 gene | ( |
| ARTUS CMV RGQ MDX Kit | Qiagen | Quantitative PCR | Plasma | Major immediate early gene (MIE) | ( |
| COBAS AmpliPrep/COBAS TaqMan CMV Test | Roche Molecular | Quantitative PCR | Plasma | UL54 | ( |
| COBAS CMV test | Roche Molecular | Quantitative PCR | Plasma | UL54 | ( |
| Simplexa Congenital CMV Direct | DiaSorin | Qualitative PCR | Saliva and urine | UL54 | ( |
| Alethia CMV DNA Amplification Assay | Meridian Bioscience | Qualitative LAMP | Saliva | UL33 gene | ( |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Viral Infections and Immunology Research · T-cell and Retrovirus Studies
INTRODUCTION
Cytomegalovirus (CMV), a beta-herpes virus, causes significant morbidity and mortality in immunocompromised patients and is the leading cause of congenital infection and hearing loss in children in industrialized countries (1). Nucleic acid amplification tests (NAATs) are preferred for diagnosis and monitoring response to CMV-directed therapy. Primers and/or probes typically target highly conserved regions of the genome, such as glycoprotein B (UL55), DNA polymerase (UL54), matrix phosphoprotein (UL83), or major immediate-early (MIE) gene (2–4). However, nucleotide variability within UL55 and MIE genes causing false-negative results has been reported (2, 5–7).
The Clinical Microbiology Laboratories at Nationwide Children’s Hospital has offered a laboratory-developed quantitative real-time PCR assay targeting a 61 bp fragment of the UL54 gene from plasma as the standard-of-care molecular assay since 2003 (SOC-PCR) (3). Here, we describe a pediatric hematopoietic cell transplant (HCT) patient in whom this assay produced false negatives due to mutations in UL54, delaying initiation of CMV therapy.
CASE PRESENTATION
A 4-month-old patient with familial hemophagocytic lymphohistiocytosis (homozygous PRF1 mutation) received myeloablative conditioning and a 10/10 matched unrelated allogeneic HCT from a CMV-seropositive donor (recipient was CMV seropositive). Pre-HCT CMV NAAT testing was negative. The infant was considered at high risk of CMV reactivation, and per institutional protocol, preemptive prophylaxis management with twice-weekly CMV monitoring by SOC-PCR on plasma was performed post-transplant and was not detected.
Thirteen days post-HCT (D + 13), the patient developed respiratory failure requiring intubation and progressive bilateral multifocal ground-glass opacities on imaging, consistent with alveolar hemorrhage and potential CMV pneumonitis. Infectious disease evaluation was negative, including blood cultures and adenovirus, herpes simplex virus, human herpes virus 6 PCRs and CMV-SOC PCR, respiratory tract secretions for bacterial cultures, adenovirus, HSV, Pneumocystis jirovecii PCRs and CMV-SOC PCR and multiplex respiratory panel (BioFire Respiratory Panel 2.0), as well as Aspergillus galactomannan (Platelia Aspergillus Ag). The evaluation was further expanded to include Legionella PCR, Aspergillus and Mucorales PCR on lower respiratory tract secretions with reflex to universal broad-range fungal PCR and Legionella urine antigen; all were negative. The patient achieved neutrophil engraftment on D + 21, and weekly CMV SOC-PCR monitoring remained negative (Fig. 1).
*Plasma CMV viral loads by assay type and patient’s clinical course. Viral loads were reported as indeterminate. CMV, cytomegalovirus; FOS, foscarnet; GCV, ganciclovir; HCT, hematopoietic cell transplantation; IVIG, intravenous immunoglobulin.
On D + 29, the patient’s plasma exhibited an unusual amplification curve on the CMV SOC-PCR. The signal did cross the detection threshold and increased in amplitude slightly; it did not display logarithmic growth. Review of prior runs, although not crossing the threshold, showed similar atypical curves in samples previously reported as negative (Fig. 2A). These findings raised concern for false-negative results; therefore, the D + 29 sample was reported as indeterminate. The treating team was notified of this unusual result, and D + 29 plasma was sent to a reference laboratory using a PCR targeting the CMV US9 gene. On the following day (D + 30), the plasma again demonstrated the same unusual amplification curve and was reported as positive after review. On D + 31, the reference laboratory reported a viral load of 1,260,000 IU/mL (6.1 log_10_ IU/mL) for the D + 29 sample, confirming our suspicion. Ganciclovir (5 mg/kg/dose every 12 hours) was started for CMV DNAemia (D + 31), and intravenous CMV immunoglobulin was given for possible CMV pneumonitis. Foscarnet (60 mg/kg/dose every 8 hours) was added to the treatment regimen. Weekly CMV monitoring was subsequently performed at the reference laboratory. Despite treatment, downtrending CMV PCR, and no evidence of hepatitis or retinitis, the patient remained critically ill. Plasma collected on D + 37 and D + 51 was sent to a reference laboratory to detect mutations within UL97 and UL54 genes by Sanger sequencing, and no mutations associated with ganciclovir or foscarnet resistance were found. On D + 51, the patient acutely developed refractory hypoxemia and asystolic cardiac arrest not responsive to resuscitation efforts.
(A) CMV SOC-PCR amplification curves from the patient’s samples, assay controls, and other positive samples. Assay controls and other positive samples display typical sigmoidal shape with flat baseline, exponential rise, and plateau phase, while the patient’s samples displayed unusual amplification curves. (B) Alignment of the partial UL54 gene: amplification region for the CMV SOC-PCR, from reference strain (NC_006273), assay control, and the patient’s sample. The location of the primers and probe is illustrated. The mutations within the probe-binding site found in the patient’s sample are highlighted in green.
The patient was CMV seropositive prior to the transplant; however, this was considered likely reflective of passive maternal antibody, and all CMV NAAT results pre-HCT were negative. To investigate further, we developed another CMV PCR targeting the US9 gene (US9-PCR) testing all available remnant specimens (Fig. 1). We detected CMV DNAemia pretransplant and rising DNAemia post-HCT, demonstrating that the SOC-PCR had repeatedly produced false-negative results. This led to delayed detection of CMV DNAemia and delayed initiation of CMV preemptive therapy by 16 days.
One of the patient’s samples was sequenced in the region targeted by SOC-PCR, which revealed two C-T substitutions within the probe-binding site (Fig. 2B), confirming the false-negative results were due to sequence variation. Searches of publicly available databases (NCBI, accessed 8 June 2025) revealed three reports of these mutations: Belgium (GenBank KP745705, submitted 2015), Germany (GenBank JX512203, 2016), and Czech Republic (KY490065, 2017).
DISCUSSION
HCT recipients at risk of CMV disease (all CMV-seropositive recipients and CMV-seronegative recipients with a CMV-seropositive donor) are monitored closely for CMV. The preemptive therapy strategy, involving monitoring for CMV DNAemia during at-risk periods and initiating antivirals when the CMV load reaches a certain threshold, has been proven highly effective in preventing CMV end-organ disease (8, 9). Furthermore, pretransplant CMV DNAemia is a strong risk factor for post-HCT CMV reactivation and associated complications (10, 11). Antiviral therapy to clear CMV DNAemia pre-HCT reduces the risk of reactivation post-HCT (10). With the US9-PCR, we detected CMV DNAemia in pretransplant samples and rising in DNAemia post-HCT, demonstrating that the SOC-PCR had repeatedly produced false negatives.
NAATs are inherently susceptible to false-negative results due to sequence diversity in the target genome. Extensive variability in the CMV genome and demonstration of multiple variants coexisting in an individual make assay design challenging (12, 13). In one prior report, it was found that samples from a leukemia patient undergoing antiviral therapy tested falsely negative on the COBAS assay (UL54 target) for a period of 2 months. Retrospective testing with a dual target PCR assay (UL54 and UL55) revealed high viral loads. These false-negative results delayed appropriate antiviral treatment. Although sequencing was not performed, the authors suggested that mutations within the primer/probe-binding regions were the probable cause (7). Additionally, a mismatch in the primer/probe region can lead to falsely low viral load. In the aforementioned study, viral loads for other samples tested were considerably lower for the UL55 assay than for the UL54 assay. Subsequent sequencing revealed a mismatch within the primer/probe for the UL55 assay (7).
Given the serious consequences of a false-negative CMV results, we implemented a surveillance program to screen SOC-PCR negative samples with the US9-PCR assay. Among >3,000 samples testing negative on the SOC-PCR that have been screened to date, four additional samples from four unique patients tested positive by US9-PCR assay. We sequenced one of these samples, revealing the same mutations as described in this case. This suggests that the primer/probe used in the SOC-PCR remains broadly inclusive and that strains carrying mutations compromising detection are relatively rare. Nevertheless, it is important for clinical laboratories and assay manufacturers to evaluate the inclusivity of their assays periodically. A 2009 study evaluating published CMV primers/probes identified a primer/probe set targeting UL54, which is the one used in our SOC-PCR, as one of the three most sensitive sets for CMV detection. In silico analysis revealed only one mismatch within the Towne strain (14). Our recent analysis of 462 published CMV sequences (NCBI, accessed 8 June 2025) identified 47 with at least one mismatch in the SOC-PCR binding region, although most involved a single mismatch unlikely to affect assay performance. This highlights the importance of ongoing evaluation of NAATs against newly submitted sequences. As mandated by the College of American Pathologists, clinical laboratories are required to evaluate laboratory-developed NAATs for compatibility with currently circulating microbial strains, thus ensuring continued diagnostic accuracy.
To enhance inclusivity, some CMV NAATs incorporate two distinct genomic targets as the likelihood of concurrent mutations in two conserved regions is low. Among eight FDA-approved CMV NAATs (Table 1), two utilize both UL34 and UL80.5 as targets. In one multicenter evaluation of the Alinity mCMV assay, only 8 of 336 positives were missed, and one discordant sample showed a higher load by Alinity than by a single-target reference PCR, suggesting target-region mismatch in the reference assay (15). Another study also demonstrated high agreement between the Alinity mCMV and a reference method (16). Single-target commercial assays have also shown high sensitivity and specificity (17–24) (Table 1), though rare false negatives do occur. A study of ARTUS CMV PCR demonstrated false lowering of viral loads with mismatches in the MIE target implicated as the cause (25). Notably, three FDA-approved assays use UL54 alone, but their proprietary primer/probe sequences preclude in silico inclusivity checks by users.
Although not clinically available at the time, metagenomic next-generation sequencing (mNGS) could have allowed for broad pathogen detection in blood and pulmonary fluid samples in this case (30) as mNGS is not susceptible to sequence diversity and can detect mutated pathogens as efficiently as the wild-type strains.
To the best of our knowledge, CMV UL54 mutations causing diagnostic failure have not been previously reported. Our case underscores the importance of rigorous and routine evaluation of CMV NAATs, even with well-characterized primer/probe sets. Laboratories should be aware of the limitations of NAATs and implement mitigation strategies, such as reviewing amplification curves for unusual patterns, periodic in silico analysis, thorough literature review, close communication with clinicians to identify potential false-negative cases, and considering use of multitarget assays. When laboratory findings conflict with clinical data, clinicians should critically assess a negative NAAT result and consider testing using an alternative gene target or mNGS for broader pathogen coverage.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leber AL. 2024. Maternal and congenital human cytomegalovirus infection: laboratory testing for detection and diagnosis. J Clin Microbiol 62:e 0031323. doi:10.1128/jcm.00313-2338391188 PMC 11005381 · doi ↗ · pubmed ↗
- 2Novak Z, Chowdhury N, Ross SA, Pati SK, Fowler K, Boppana SB. 2011. Diagnostic consequences of cytomegalovirus glycoprotein B polymorphisms. J Clin Microbiol 49:3033–3035. doi:10.1128/JCM.01039-1121653769 PMC 3147759 · doi ↗ · pubmed ↗
- 3Sanchez JL, Storch GA. 2002. Multiplex, quantitative, real-time PCR assay for cytomegalovirus and human DNA. J Clin Microbiol 40:2381–2386. doi:10.1128/JCM.40.7.2381-2386.200212089251 PMC 120584 · doi ↗ · pubmed ↗
- 4Boppana SB, Ross SA, Novak Z, Shimamura M, Tolan RW Jr, Palmer AL, Ahmed A, Michaels MG, Sánchez PJ, Bernstein DI, Britt WJ, Fowler KB, National Institute on Deafness and Other Communication Disorders CMV and Hearing Multicenter Screening (CHIMES) Study. 2010. Dried blood spot real-time polymerase chain reaction assays to screen newborns for congenital cytomegalovirus infection. JAMA 303:1375–1382. doi:10.1001/jama.2010.42320388893 PMC 2997517 · doi ↗ · pubmed ↗
- 5Lengerova M, Racil Z, Volfova P, Lochmanova J, Berkovcova J, Dvorakova D, Vorlicek J, Mayer J. 2007. Real-time PCR diagnostics failure caused by nucleotide variability within exon 4 of the human cytomegalovirus major immediate-early gene. J Clin Microbiol 45:1042–1044. doi:10.1128/JCM.01109-0617229861 PMC 1829136 · doi ↗ · pubmed ↗
- 6Nye MB, Leman AR, Meyer ME, Menegus MA, Rothberg PG. 2005. Sequence diversity in the glycoprotein B gene complicates real-time PCR assays for detection and quantification of cytomegalovirus. J Clin Microbiol 43:4968–4971. doi:10.1128/JCM.43.10.4968-4971.200516207949 PMC 1248473 · doi ↗ · pubmed ↗
- 7Herrmann B, Larsson VC, Rubin C-J, Sund F, Eriksson B-M, Arvidson J, Yun Z, Bondeson K, Blomberg J. 2004. Comparison of a duplex quantitative real-time PCR assay and the COBAS Amplicor CMV Monitor test for detection of cytomegalovirus. J Clin Microbiol 42:1909–1914. doi:10.1128/JCM.42.5.1909-1914.200415131148 PMC 404600 · doi ↗ · pubmed ↗
- 8Boeckh M, Ljungman P. 2009. How we treat cytomegalovirus in hematopoietic cell transplant recipients. Blood 113:5711–5719. doi:10.1182/blood-2008-10-14356019299333 PMC 2700312 · doi ↗ · pubmed ↗