A post-implementation evaluation of BioFire FilmArray Meningitis/Encephalitis panel for pathogen detection in cerebrospinal fluid with a special focus on clinical significance of HHV-6
Manoshi Perera, Hemalatha Varadhan, Aileen Oon

TL;DR
This study evaluates a molecular test for detecting pathogens in cerebrospinal fluid and highlights the importance of proper interpretation, especially for HHV-6.
Contribution
The study emphasizes the need for diagnostic stewardship to avoid misinterpretation of HHV-6 detection in CSF using syndromic panels.
Findings
CSF specimens with elevated white cell count had higher NAAT-positive rates.
HHV-6 was detected in 48 CSF specimens, often in immunocompromised individuals.
Syndromic panels without stewardship may detect bystander pathogens like HHV-6.
Abstract
Syndromic molecular testing for the diagnosis of infections has been advantageous given high sensitivity and rapid diagnostics; however, challenges remain with appropriate interpretation. A post-implementation evaluation of the cerebrospinal fluid (CSF) BioMerieux BioFire FilmArray Meningitis/Encephalitis panel in an adult and pediatric population was performed. The aims were to assess the prevalence and epidemiology of all targets and to correlate laboratory parameters with results from human herpesvirus 6 (HHV-6) detection in CSF to identify opportunities to apply diagnostic stewardship. A retrospective observational study was conducted on CSF Nucleic Acid Amplification Test (NAAT) results performed at a referral laboratory in Australia between 19 March 2022 and 31 July 2023. Laboratory data were extracted, with additional clinical data obtained for the HHV-6 positive subcohort. Of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
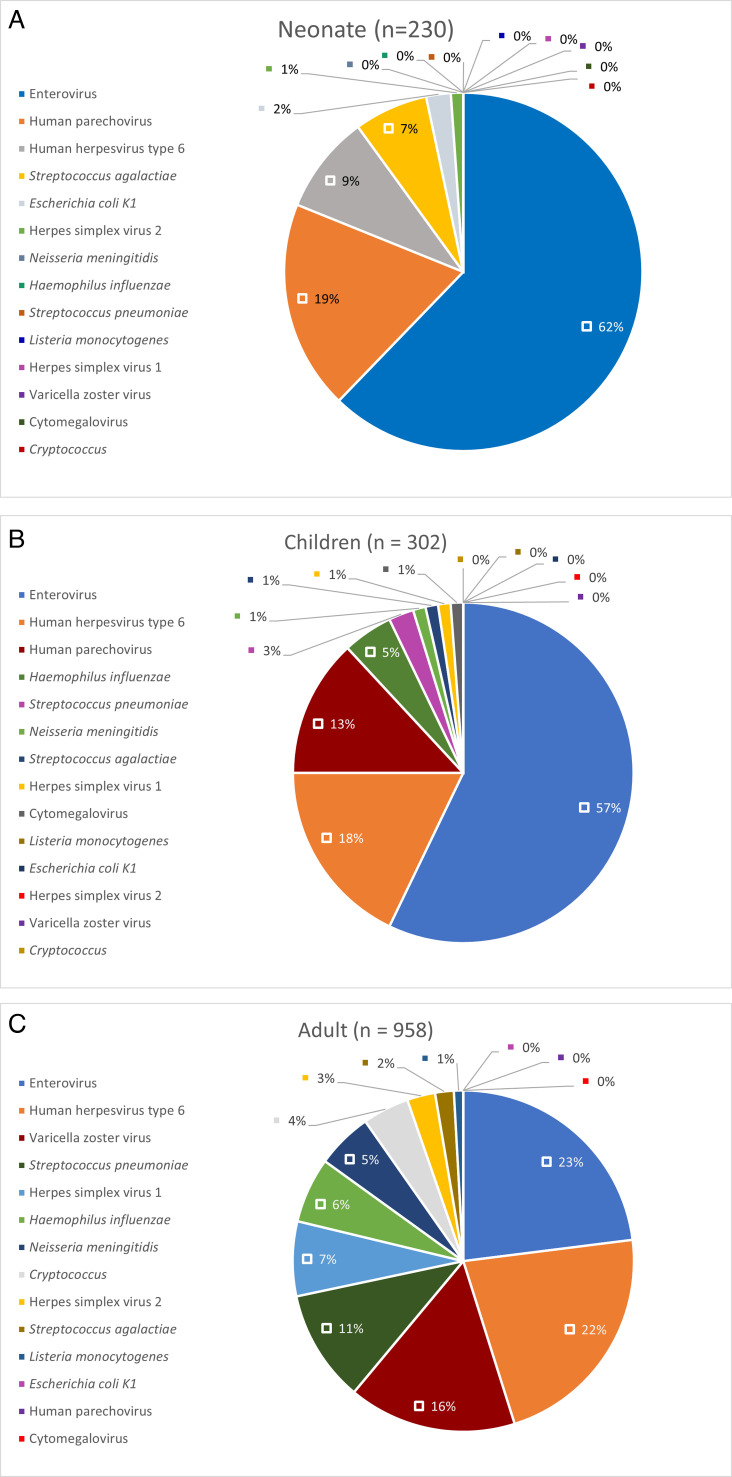 Fig 1
Fig 1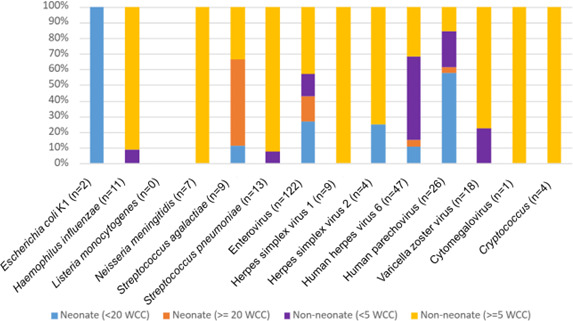 Fig 2
Fig 2| Characteristic | |
|---|---|
| Male | 775 (52) |
| Female | 715 (48) |
| Age at CSF collection, years (median, IQR) | 34.9 (0.3–61.7) |
| Neonate | 230 (15.4) |
| Children | 302 (20.3) |
| Adult | 958 (64.3) |
| Positive CSF NAAT | 287 (19.3) |
| >1 detected | 5 (0.3) |
| Enterovirus RNA detected | 130 (8.7) |
| Human herpesvirus type 6 DNA detected | 48 (3.2) |
| Human parechovirus RNA detected | 28 (1.9) |
| Varicella zoster virus DNA detected | 18 (1.2) |
| 14 (0.9) | |
| 11 (0.7) | |
| Herpes simplex virus type 1 DNA detected | 9 (0.6) |
| 9 (0.6) | |
| 7 (0.5) | |
| 5 (0.3) | |
| Herpes simplex virus type 2 DNA detected | 4 (0.3) |
| 2 (0.1) | |
| Cytomegalovirus DNA detected | 1 (0.1) |
| 1 (0.1) |
| Pathogen | Positive CSF culture | Positive NAAT | % (positive CSF culture/ |
|---|---|---|---|
| | 3 | 3 | 100 |
| | 2 | 2 | 100 |
|
| 4 | 11 | 36.4 |
|
| 5 | 14 | 35.7 |
|
| 2 | 9 | 22.2 |
|
| 0 | 2 | 0 |
|
| 0 | 7 | 0 |
| Characteristic | Neonates, | Children, |
|---|---|---|
| Growth on CSF culture | 7 (3.0) | 9 (3.0) |
| Positive NAAT | 90 (39.1) | 84 (27.8) |
| Enterovirus | 56 (24.3) | 48 (15.9) |
| Parechovirus | 17 (7.4) | 11 (3.6) |
| HHV-6 | 8 (3.4) | 15 (5.0) |
| | 6 (2.6) | 1 (0.3) |
| | 0 (0) | 4 (1.3) |
| | 0 (0) | 0 (0) |
| | 2 (0.9) | 0 (0) |
| | 0 (0) | 2 (0.7) |
| | 0 (0) | 1 (0.3) |
| CMV | 0 (0) | 1 (0.3) |
| HSV 1 | 0 (0) | 1 (0.3) |
| HSV 2 | 1 (0.4) | 0 (0) |
| VZV | 0 (0) | 0 (0) |
| | 0 (0) | 0 (0) |
| Characteristic | |
|---|---|
| Male | 28 (58.3) |
| Age at CSF collection, years (median, IQR) | 24.3 (0.5–58.7) |
| CSF WCC, ×106 cells/L (median, IQR) | 2 (0.5–11.5) |
| CSF WCC differential (median, IQR) | |
| PMN % | 3.5 (0–23.75) |
| Mononuclear % | 82 (36.3–99.5) |
| Not performed | 30 (62.5) |
| CSF RBC ≥ 5, ×106 cells/L | 20 (41.7) |
| Neonate | 5 (25.0) |
| Children | 3 (15.0) |
| Adult | 12 (60.0) |
| CSF biochemistry | |
| Glucose (<LLN) | 7 (14.6) |
| Protein (>ULN) | 12 (25.0) |
| Lactate (>ULN) | 2 (4.2) |
| Not recorded | 16 (33.3) |
| Immunocompetent; peripheral WCC, ×109 cells/L (median, IQR) | 9.6 (7.4–13.6) |
| Lymphocyte % | 27 (16–48) |
| Neutrophil % | 62 (34–74) |
| Immunocompromised; peripheral WCC, ×109 cells/L (median, IQR) | 7.6 (4.4–9.7) |
| Lymphocyte % | 12 (9–15) |
| Neutrophil % | 75 (71–88) |
| Not recorded | 6 (12.5) |
| Serum HHV-6 quantitative NAAT | 6 (12.5) |
| Copies/mL (median, IQR) | 2,809 (1,924.3–3,915) |
| HHV-6 serology | 6 (12.5) |
| Recorded clinical diagnosis | |
| HHV-6 meningoencephalitis or myelitis | 11 (22.9) |
| Non-meningoencephalitis | 30 (62.5) |
| Not recorded | 7 (14.6) |
| Directed anti-viral therapy | 7 (14.6) |
| Not recorded | 7 (14.6) |
| Immunocompromised status | 10 (20.8) |
| Malignancy | 5 (50) |
| Autoimmune disease on immunosuppressants | 4 (40) |
| Transplant recipient | 1 (10) |
| Not recorded | 4 (8.3) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Polyomavirus and related diseases · Infectious Encephalopathies and Encephalitis
INTRODUCTION
The introduction of syndromic molecular testing methods for the diagnosis of central nervous system (CNS) infections has been advantageous, given high sensitivity and subsequent implications of rapid diagnostics leading to prompt antimicrobial rationalization, optimal clinical outcomes, and an impact upon financial burden (1).
Global epidemiology studies have identified a comparatively low rate of CNS infection in Australia, with an incidence of encephalitis of 2.08 per 100,000 person-years in 2019 (2), and an incidence of meningitis in 2016 of 0.5 per 100,000 persons (3). A large prospective cohort study identified enteroviruses, human parechovirus, herpes simplex virus (HSV), and Streptococcus species as the highest causes of meningoencephalitis among Australian children (4). Similarly, in a study over an 18-year period, HSV and varicella zoster virus (VZV) were identified as the most common causes of hospitalization due to encephalitis among adults. The etiology of CNS infections has likely also been impacted by the implementation of nationwide targeted immunization schedules for Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis (5).
Human herpesvirus 6 (HHV-6) is a ubiquitous herpesvirus with a wide spectrum of disease from benign, self-limiting illness in children to encephalitis within an immunocompromised host (6). The seroprevalence of HHV-6 in the adult population globally is estimated to be >90%, with the majority of primary infections occurring in childhood (7). HHV-6 has a unique ability among other members of the family Herpesviridae to integrate into the subtelomeric regions of human chromosomes in every host cell (6). Described as chromosomally integrated HHV-6 (ciHHV-6), it has an estimated prevalence of 1% in humans (8). Hence, detection of HHV-6 nucleic acid in cerebrospinal fluid (CSF) may represent primary infection, latency, secondary reactivation, or ciHHV-6 present with host cells within CSF (1). Subsequently, challenges arise in the interpretation of results from a highly sensitive assay like the BioMerieux BioFire FilmArray Meningitis/Encephalitis (FAME) assay and necessitate appropriate correlation with clinical findings (9).
No standardized treatment guidelines are available for the management of HHV-6; however, literature has reported positive outcomes with the use of ganciclovir, foscarnet, and less frequently, cidofovir (10, 11). These antiviral therapies are associated with significant adverse effects, including anemia, electrolyte disturbance, and nephrotoxicity, and hence require close monitoring during use (10). Subsequently, the implications of reporting and interpretation of results need to be carefully considered by laboratories that perform diagnostic testing.
In March 2022, our laboratory implemented the BioMerieux BioFire FAME assay as part of CSF multiplex Nucleic Acid Amplification Test (NAAT) testing in order to facilitate more rapid diagnostics for a large, heterogeneous adult and pediatric patient population. Prior to the implementation of the assay in March 2022, CSF specimens were referred for testing of targeted pathogens as specifically requested by the clinician.
Aim
Evaluation of the diagnostic performance of the BioMerieux BioFire FAME panel (from this point forward referred to as CSF NAAT), on CSF in a population of adult and pediatric patients was undertaken with two main aims. The first is to assess the prevalence and epidemiology of all NAAT targets, and the second is to correlate laboratory parameters with results from HHV-6 detection on CSF to identify opportunities for the laboratory to apply diagnostic stewardship.
MATERIALS AND METHODS
A retrospective observational study was conducted of CSF NAAT results, performed at a single referral laboratory in Newcastle (New South Wales), Australia between 19 March 2022 and 31 July 2023. The laboratory service performs testing for regional and rural health facilities in the region and is co-located with an adult and a specialist children’s hospital, which includes transplant, hematology, and oncology clinical services. Inclusion criteria included pediatric and adult CSF specimens obtained from lumbar puncture, at least 200 µL volume collected, and referred specimens from Hunter New England and Mid-North Coast Local Health Districts. Exclusion criteria included forensic specimens, repeat specimens collected from the same patient during the same admission period, and specimens collected external to the pre-defined local health districts.
Laboratory procedures
CSF multiplex NAAT testing is ordered at clinician discretion, and the BioMerieux BioFire FAME assay is performed as per the manufacturer’s instructions for use. The CSF NAAT is an automated, real-time assay from BioMerieux BioFire Diagnostics which enables the isolation, amplification, and detection of nucleic acid from seven viral targets—HSV 1 and 2, VZV, HHV-6, human parechovirus, enterovirus, and cytomegalovirus (CMV)—as well as Cryptococcus neoformans/gattii and six bacterial targets—Listeria monocytogenes, Neisseria meningitidis, Streptococcus pneumoniae, Streptococcus agalactiae, Escherichia coli K1, and Haemophilus influenzae. Analysis occurs simultaneously from a single 200 µL CSF specimen, producing a qualitative result within approximately 1 h. Detection of a pathogen is considered a critical result and is verbally notified to the treating clinician.
CSF microscopy and bacterial culture are performed onsite as per local laboratory standard procedures. Microscopy, including cell count and Gram stain, is performed manually, and culture plates are incubated for a minimum of 5 days. Organism identification is performed using MALDI-ToF (Bruker Biotyper).
HHV-6 serum quantitative NAAT and serology were referred to an external reference laboratory. No other targeted NAAT testing was performed on CSF specimens.
Data collection
Laboratory data were extracted from the laboratory information system (AUSLAB). This included results of CSF NAAT, CSF culture, and CSF microscopy (white cell count, WCC), in addition to patient demographics of age and gender. Additional laboratory data were obtained for the CSF HHV-6 positive subcohort, including CSF microscopy (red blood cell, RBC; WCC differential), CSF biochemistry (glucose, lactate, and protein), peripheral WCC and differential, serum HHV-6 viral load, and HHV-6 serology. Additional clinical details, including immunocompromised status, documented clinical diagnosis, and antiviral therapy received, were obtained for the CSF HHV-6 positive subcohort.
Normal CSF WCC in adults and children (aged between 1 month and 18 years) was defined as <5 × 10^6^ cells/L and RBC as <5 × 10^6^ cells/L (12, 13). Normal CSF WCC in neonates (≤1 month) was defined as <20 × 10^6^ cells/L (14, 15). Normal ranges for CSF biochemistry were defined as follows: glucose 2.8–4.5 mmol/L with lower limit of normal (LLN) < 2.8 mmol/L, protein 0.2–0.7g/L with upper limit of normal (ULN) > 0.7 g/L, and lactate < 2.8 mmol/L with ULN ≥ 2.8 mmol/L (13). Normal CSF biochemistry in neonates included glucose ≥ 2.0 mmol/L and protein < 1.0 g/L (12).
Statistical analysis
Standard descriptive statistics were used to analyze participant demographics, microbiological data, and clinical data. Qualitative/categorical variables were described as counts and proportions and compared with the chi-square test. Statistical significance was accepted as P < 0.05. Microsoft Excel version 16.0 and IBM SPSS version 29.0 were used for statistical analysis.
RESULTS
Total cohort
Overview
During the study period, 1,490 CSF specimens were identified from 1,457 different patients. Thirty-three patients had more than one CSF NAAT performed in the study period during different admission episodes, with the median number of days between collection being 25 (interquartile range [IQR]: 17.0–65.0). There was a male preponderance of 52% with the median age at CSF collection of 34.9 years (range 0.3–61.7 years). The cohort comprised 958 (64.3%) specimens from adults, 302 (20.3%) from children, and 230 (15.4%) from neonates.
CSF NAAT
A positive CSF NAAT was identified in 287 specimens (19.3%), with five specimens (0.3%) having more than one organism detected. This included one specimen with VZV and Streptococcus pneumoniae detected, two specimens with HHV-6 and enterovirus, one specimen with HHV-6 and Streptococcus agalactiae, and one specimen with HHV-6 and VZV (Table 1). Enterovirus was detected in 130 specimens (8.7%), and HHV-6 was detected in 48 specimens (3.2%). There was a variable distribution of pathogens detected between the neonate, children, and adult subcohorts (Fig. 1).
(A) Proportion of positive CSF NAAT panel targets for the subcohort of neonates (≤1 month). (B) Proportion of positive CSF NAAT panel targets for the subcohort of children (between 1 month and 18 years). (C) Proportion of positive CSF NAAT panel targets for the subcohort of adults (≥18 years).
CSF culture
There was no growth from culture in 1,421 (95.4%) specimens, and culture was not performed for 15 (1.0%) specimens. Of samples which isolated an organism from culture, 38 (70.4%) were not target pathogens within the CSF NAAT panel—these included coagulase-negative staphylococci (20, 37%), Candida dubliniensis (1, 1.9%), Staphylococcus aureus (1, 1.9%), other Gram-positive organisms (13, 24.1%), and other Gram-negative organisms (3, 5.6%). Concordance of bacterial and fungal NAAT targets and culture results was seen in 16 (33.3%) specimens, with concordance seen in all Cryptococcus cases (Table 2). Four CSF specimens with a virus detected on NAAT isolated bacteria on CSF culture, including coagulase-negative staphylococci and other Gram-positive organisms.
CSF microscopy
The median WCC on CSF microscopy was 3 × 10^6^ cells/L (IQR: 1–16.8), with 61 specimens without documented WCC. A WCC within normal range (<5 × 10^6^ cells/L) was identified in 844 (844/1,260, 67.0%) specimens among non-neonates and 165 (165/230, 71.7%) specimens with normal WCC (<20 × 10^6^ cells/L) in the neonate subcohort. Among all age groups, there were 24 (2.4%) positive CSF cultures with WCC within normal range. The organisms isolated included coagulase-negative staphylococci and other Gram-positive and Gram-negative organisms. A positive CSF NAAT result was obtained in 7.5% of specimens in this cohort with WCC within normal range, with enterovirus most frequently detected (Fig. 2). In contrast, there were 347 CSF specimens from non-neonates with elevated WCC (≥5 × 10^6^ cells/L) and negative CSF culture, of which 115 (33.1%) had a positive NAAT. Overall, non-neonate CSF specimens with a WCC above normal range had a higher proportion of NAAT-positive rates (35.3%) compared to those with a WCC < 5 × 10^6^ cells/L (6.5%) (P < 0.001).
Comparison of positive NAAT targets in patients with elevated CSF WCC (non-neonates ≥ 5 × 106 cells/L, neonates ≥ 20 × 106 cells/L) to patients with a WCC within normal range (non-neonates < 5 × 106 cells/L, neonates < 20 × 106 cells/L). WCC was not recorded for 13 specimens.
Age-based subcohorts
There were 958 (64.3%) adult CSF specimens and 532 obtained from pediatrics patients, comprising 230 (15.4%) neonates and 302 (20.3%) children, respectively. Of the latter cohort, 16 had growth on respective CSF cultures, including one specimen with Haemophilus influenzae, three specimens with Streptococcus, one specimen with Candida, and the others either coagulase-negative staphylococci or other Gram-positive organisms (Table 3). A positive NAAT result was detected in 90 (39.1%) specimens in neonates and 84 (27.8%) specimens in children, with proportionally viral targets more frequently detected including enterovirus and parechovirus. While enterovirus (23%) and HHV-6 (22%) were the most commonly detected targets among NAAT-positive specimens in adults, there were also more frequent bacterial/fungal detections compared to the pediatric cohort. This was supported by 38 positive CSF cultures, including five Cryptococcus isolates, five Streptococcus pneumoniae, and three Haemophilus influenzae.
HHV-6 positive subcohort
Forty-eight (48/1,490) CSF specimens had HHV-6 detected via NAAT, with a male preponderance (58.3%) and a median age of 24.3 years (IQR: 0.5–58.7) at CSF collection. An elevated CSF RBC above the normal range was noted in 41.7% of specimens (Table 4). An immunocompromised status was documented with 10 CSF specimens, of which two underwent HHV-6 quantitative NAAT and serology.
DISCUSSION
This study outlines the epidemiology of CSF NAAT positivity in a heterogeneous adult and pediatric population. Furthermore, it highlights parameters for the application of diagnostic stewardship, as exemplified by the frequency of detection of HHV-6.
The advantages of utilizing a CSF multiplex NAAT are often recognized in cases of aseptic meningitis—CSF specimens with elevated WCC and negative culture (16). Our study had positive identification in 33.1% of these specimens via NAAT, including bacterial pathogens. Enterovirus was the most commonly detected pathogen on NAAT in our study, and this was similarly reported in a recent study as the most common cause of aseptic meningitis in a cohort of pediatric and adult patients (16). The overall concordance between culture and bacterial/fungal targets was lower in our study (33.3%) than previously described by Myint et al., though comparable H. influenzae and N. meningitidis targets (17). Interestingly, our study had 100% concordance between CSF NAAT and culture results for Cryptococcus gattii and Cryptococcus neoformans. This contrasts with previous studies which have highlighted a high false-negative rate for the CSF NAAT, particularly among patients on anti-fungal therapy and/or who have a low disease burden (18). Other instances of false negatives have been described in association with HSV 1/2 (19). Hence, recommendations made by our laboratory to repeat CSF collection if clinical suspicion for HSV infection remains. Instances of NAAT bacteria detection with sterile CSF culture were noted; however, an attributable cause was not directly assessed—a limitation of our study. Previously ascribed causes include antimicrobial treatment prior to specimen collection in hospital or community, fastidiousness of organism, and organism concentration at assay limit of detection (16, 20). The majority (80.7%) of CSF specimens in our study had a negative NAAT panel, which is similar to rates reported by Precit et al., who had a comparable patient cohort and size (20). This raises concerns about overutilization of the assay (20), emphasizing the need to rationalize testing algorithms and employ diagnostic stewardship practices (21). A lenient testing criterion can be detrimental in placing an added burden on clinicians with regard to the interpretation of results. Restriction criteria previously explored include CSF WCC within the normal range; however, studies have described that the absence of leukocytosis is not always reliable (10, 22). Important exceptions to consider include specimens from neonates and detection of parechovirus, which is commonly associated with the absence of reactive pleocytosis (15, 23). This was similarly seen in our study with detection of bacterial pathogens, including S. agalactiae and E. coli K1 target via NAAT in neonates with CSF WCC within normal range. Within our cohort, there was a statistically significant difference in NAAT positivity between non-neonate specimens with normal and elevated CSF WCC. There was only 6.5% NAAT positivity among non-neonates with CSF WCC within normal range, with a minority of targets requiring directed therapy and positive cultures with growth of what were deemed likely contaminants. Most pathogens detected in this subcohort included viruses associated with reactivation but not clinical CNS disease, such as HHV-6 and VZV (1). Of the two positive NAAT bacterial detection, S. pneumoniae was deemed clinically unlikely and a possible false positive due to contamination, which has previously been reported by Leber et al. (16). While, detection of H. influenzae on NAAT with a sterile culture, may be attributable to antimicrobial treatment prior to specimen collection (17). Thereby supporting the use of this WCC criterion among non-neonate specimens as a prompt for clinician discussion prior to proceeding with CSF NAAT.
Another consideration with the use of multiplex NAAT testing methods is the identification of targets which may not correlate with clinical pathogenicity. This is particularly important with viruses given the possibility of subclinical reactivation, latency, and genomic integration (1). The incidence of reported HHV-6 associated meningoencephalitis or transverse myelitis in the HHV-6 positive cohort (22.9%) was similar to that reported by Pandey et al. (24). However, compared to Pandey et al., which was only of pediatric patients, our study cohort had a median age of 24.3 years, with only 35.7% of CSF specimens from patients aged <18 years (24). This is an important consideration, given HHV-6 meningoencephalitis among immunocompetent adults is reportedly rare, and our study cohort included a majority (79.2%) without an immunocompromised status documented (25). Furthermore, the predominant peripheral neutrophilia among the immunocompetent patients may suggest a non-viral etiology. In contrast, HHV-6 associated with severe clinical outcomes has been described among immunocompromised individuals, with manifestations of encephalitis, hemophagocytic lymphohistiocytosis, long-term neurological sequelae, and mortality (26). Although HHV-6 reactivation can occur in up to two-thirds of hematopoietic stem cell transplant recipients, the prevalence of encephalitis among this cohort remains small, as low as 1.4% (27). Further to the low prevalence of HHV-6 meningoencephalitis, the clinical symptoms remain nonspecific, including headache, delirium, and seizures (28), further impacting upon clinician confidence in diagnosing infection. This may have contributed to the diagnosis of two immunocompetent patients within the study cohort with HHV-6 CNS infection who received targeted anti-viral therapy with ganciclovir. Other factors which can further complicate interpretation are in CSF specimens with elevated RBC, suggestive of a traumatic lumbar puncture and possible blood contamination. Thereby, the presence may represent serum levels, rather than be representative of CNS infections (25). This may have contributed to CSF detection in 41.7% of specimens in the HHV-6 cohort in our study, which had CSF RBC levels above the ULN.
Supplementary diagnostic aids which can be utilized for HHV-6 meningoencephalitis include the presence of lymphocytic pleocytosis and elevated protein in CSF (27), although not consistently seen (25), as was similar to our study cohort with a median mononuclear cell count of 82% and elevated protein in only 25% (12/48) of specimens. Incorporation of serology into HHV-6 infection diagnostics has been infrequently reported in the literature, due to limited utility in distinguishing acute infection or reactivation from previous exposure (19). Our study had 12.5% of the HHV-6 subcohort undergo serological testing, although the diagnostic utility of one neonatal specimen is questionable unless compared to maternal serology. Furthermore, two patients with serology consistent with past infection received targeted antiviral therapy, although this may reflect the prolonged turnaround time in receiving serology results.
Serum HHV-6 quantitation can assist in differentiating active infection or reactivation; however, a high level does not consistently occur with CNS infection and can be isolated from otherwise healthy individuals (28). In contrast, digital droplet NAAT enables absolute quantitation of ciHHV-6 by fragmenting the specimen and performing multiple parallel amplification reactions concurrently (14). Although this was not performed in our study, an approximation can be made via quantitative viral load of whole blood or serum. There is a consensus in the literature that a whole blood viral load >5.5log_10_ copies/mL or serum viral load >3.5log_10_ copies/mL is suggestive of chromosomal integration (14, 24, 29, 30). However, pre-analytic factors also need to be considered prior to interpretation of viral load, including WCC count, which can significantly elevate levels (9). Of note, 50% (3/6) of patients who had serum HHV-6 quantitative NAAT performed had a viral load of >3.5log_10_ copies/mL suggestive of ciHHV-6. Overall, our study had underutilization of these supplementary tests, particularly among the subcohort of immunocompromised patients with HHV-6 detected; only two patients proceeded to have further testing, including HHV-6 quantitative NAAT. This renders interpretation challenging, given the likelihood of subclinical reactivation among immunocompromised patients and in those with severe acute illness due to another etiology (19). Hence, this emphasizes the importance of clinicians having a high pre-test probability, with concordant clinical presentation and risk factors. Pursuing supplementary testing such as quantitative HHV-6 NAAT on CSF and serum can further help clarify this, although it was not accessible in our laboratory testing network (31). This may be further prompted by the inclusion of an interpretative comment alongside HHV-6 results, suggesting detection may represent primary infection, latency, or secondary reactivation and for consideration of quantitative NAAT testing if clinically indicated.
Antiviral therapy such as ganciclovir, which targets HHV-6 DNA polymerase to inhibit viral DNA synthesis, is utilized in HHV-6 management; however, it can be associated with adverse effects such as renal impairment and bone marrow suppression (24). Other considerations including the significant financial burden of antiviral therapy and potential increased length of stay for administration of intravenous therapy. The efficacy is also poorly understood in immunocompetent pediatric populations (31), which can likely be extrapolated to immunocompetent adult patients. These concerns are similarly raised in our study, where among the 14.6% (7/48) of patients who received anti-viral therapy, three were immunocompetent hosts, including one case in a pediatric patient.
Strength of the study was the inclusion of a heterogeneous patient population, suggesting generalizability of study findings. This included analysis of CSF specimens from both pediatric and adult patients, immunocompromised patients, and inclusion of multiple regional and rural institutions. Limitations of this study include the retrospective nature and reduced sample size in some subcohorts; therefore, no power calculations were performed. Furthermore, full clinical and laboratory data were not available on all patients, in addition to lack of data regarding the prevalence of ciHHV-6 and supportive evidence such as radiological imaging to support diagnoses of HHV-6 encephalitis.
Subsequent review of these study findings provided confidence in implementing a diagnostic stewardship algorithm within our laboratory service. This involved initiating a medical microbiologist review if a non-neonate specimen had CSF WCC within normal range to determine if CSF NAAT should be performed. This included review of medical records and discussion with requesting clinician to determine the indication and underlying risk factors, e.g., immunocompromised host. Future studies worth exploring include a prospective trial following implementation of restrictive criteria for performing CSF NAAT testing on the basis of WCC and the implications on frequency of HHV-6 detection, alongside other pathogens, as well as laboratory factors, including turnaround time and cost. Development of an algorithm or tool to aid clinicians with interpretation and further investigation of HHV-6 detection on CSF specimens specific to local epidemiology, laboratory workflow practices, and available resources may also be beneficial.
Conclusions
This study highlights the caution required when utilizing high-sensitivity, rapid diagnostic assays for the detection of CSF pathogens without laboratory stewardship. Syndromic testing is not without its challenges, and this study has highlighted that HHV-6 detection in CSF, in particular, can be prone to misinterpretation. Utilization of CSF WCC as a trigger for further review of non-neonate samples may be a useful criterion to minimize this.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Waldrop G, Zucker J, Boubour A, Radmard S, Green DA, Thakur KT. 2022. Clinical significance of positive results of the Bio Fire cerebrospinal Fluid Film Array meningitis/encephalitis panel at a tertiary medical center in the United States. Arch Pathol Lab Med 146:194–200. doi:10.5858/arpa.2020-0380-OA 34086848 · doi ↗ · pubmed ↗
- 2Wang H, Zhao S, Wang S, Zheng Y, Wang S, Chen H, Pang J, Ma J, Yang X, Chen Y. 2022. Global magnitude of encephalitis burden and its evolving pattern over the past 30 years. Journal of Infection 84:777–787. doi:10.1016/j.jinf.2022.04.02635452715 · doi ↗ · pubmed ↗
- 3Zunt JR, Kassebaum NJ, Blake N, Glennie L, Wright C, Nichols E, Abd-Allah F, Abdela J, Abdelalim A, Adamu AA, et al.. 2018. Global, regional, and national burden of meningitis, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 17:1061–1082. doi:10.1016/S 1474-4422(18)30387-930507391 PMC 6234314 · doi ↗ · pubmed ↗
- 4Britton PN, Dale RC, Blyth CC, Clark JE, Crawford N, Marshall H, Elliott EJ, Macartney K, Booy R, Jones CA. 2020. Causes and clinical features of childhood encephalitis: a multicenter, prospective cohort study. Clin Infect Dis 70:2517–2526. doi:10.1093/cid/ciz 68531549170 · doi ↗ · pubmed ↗
- 5Gora H, Smith S, Wilson I, Preston-Thomas A, Ramsamy N, Hanson J. 2022. The epidemiology and outcomes of central nervous system infections in Far North Queensland, tropical Australia; 2000-2019. P Lo S One 17:e 0265410. doi:10.1371/journal.pone.026541035312713 PMC 8936475 · doi ↗ · pubmed ↗
- 6Greninger AL, Naccache SN, Pannaraj P, Jerome KR, Dien Bard J, Ruderman JW. 2019. The brief case: inherited chromosomally integrated human herpesvirus 6 (HHV-6) in the age of multiplex HHV-6 testing. J Clin Microbiol 57:e 02016-18. doi:10.1128/JCM.02016-1831551347 PMC 6760953 · doi ↗ · pubmed ↗
- 7Aimola G, Beythien G, Aswad A, Kaufer B. 2020. Current understanding of human herpesvirus 6 (HHV-6) chromosomal integration. Antiviral Res doi:10.1016/j.antiviral.2020.10472032044155 · doi ↗ · pubmed ↗
- 8Leong HN, Tuke PW, Tedder RS, Khanom AB, Eglin RP, Atkinson CE, Ward KN, Griffiths PD, Clark DA. 2007. The prevalence of chromosomally integrated human herpesvirus 6 genomes in the blood of UK blood donors. J Med Virol 79:45–51. doi:10.1002/jmv.2076017133548 · doi ↗ · pubmed ↗