Phasing out India ink: the case for the CrAg LFA in modern practice
Sejal Morjaria, Derick Iturralde, Brenden Clarck, N. Esther Babady

TL;DR
This paper argues for replacing the outdated India ink test with the more accurate CrAg LFA for diagnosing cryptococcal meningitis.
Contribution
The study provides evidence supporting the replacement of India ink with CrAg LFA for improved diagnostic accuracy.
Findings
India ink had 42.9% sensitivity compared to 100% for CrAg LFA and multiplex PCR.
CrAg LFA and PCR offer superior sensitivity, ease of use, and reproducibility.
Replacing India ink can improve detection and patient outcomes in immunocompromised individuals.
Abstract
Cryptococcal meningitis remains a life-threatening infection, particularly in immunocompromised patients, and timely, accurate diagnosis is essential. In a retrospective review of 489 cerebrospinal fluid samples at a tertiary cancer center, the India ink stain demonstrated low sensitivity (42.9%) compared to lateral flow antigen (100%) and multiplex PCR (100%) methods. These findings support replacing the outdated, labor-intensive India ink test with more accurate, rapid diagnostics to improve detection and patient outcomes. The India ink test has historically been a cornerstone of cryptococcal diagnosis, but its low sensitivity and reliance on subjective interpretation make it increasingly obsolete in modern practice. Continued reliance on India ink risks delayed or missed diagnoses, particularly in immunocompromised patients where early detection is critical. In contrast, the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
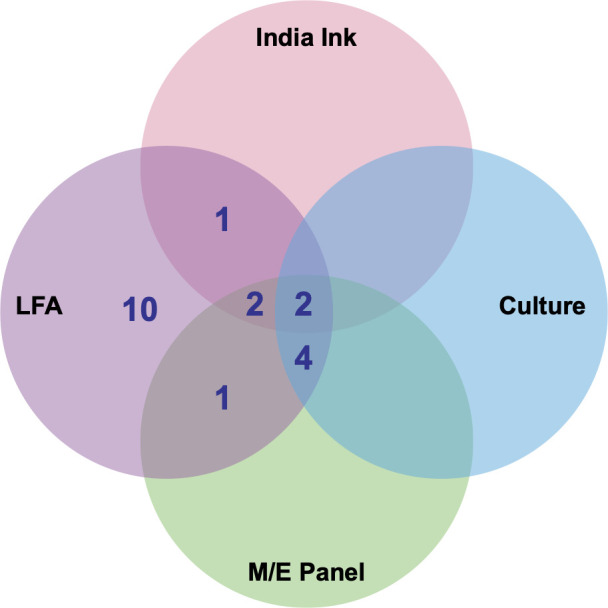 Fig 1
Fig 1| Total number | Culture positive | Culture negative | Sensitivity (%) (95% Cl) | Specificity (%) (95% Cl) | |
|---|---|---|---|---|---|
| India ink positive | 6 | 3 | 3 | 42.8 (15.8%–75.0%) | 99.4 (98.2%–99.8%) |
| India ink negative | 483 | 4 | 479 | ||
| CrAg LFA positive | 26 | 7 | 19 | 100 (64.5%–100.0%) | 94.7 (93.9%–97.6%) |
| CrAg LFA negative | 463 | 0 | 463 | ||
| M/E panel positive | 9 | 6 | 3 | 100 (61%–100.0%) | 99.3 (98.1%–99.8%) |
| M/E panel negative | 448 | 0 | 448 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Nail Diseases and Treatments · Orthopedic Infections and Treatments
OBSERVATION
Cryptococcal meningitis is a serious fungal infection of the central nervous system caused by Cryptococcus neoformans. It carries a high mortality risk, especially in immunocompromised individuals (both HIV and cancer patients) if not promptly diagnosed and treated (1, 2). The use of India ink for the diagnosis of Cryptococcus spp. has long been a standard diagnostic tool in microbiology laboratories (3, 4). However, this method is increasingly being replaced due to advances in diagnostic technology, such as the cryptococcal antigen lateral flow assay (CrAg LFA), and molecular multiplex meningitis/encephalitis (M/E) panels (BioFire). The India ink stain highlights the capsule of Cryptococcus and requires a trained medical laboratory scientist to prepare and interpret the sample, with accuracy heavily dependent on the examiner’s skill and subject to interobserver variability (5). Additionally, the India Ink test typically requires a high fungal burden (>1,000 CFU/mL) for detection, increasing the risk of errors such as false negatives (6, 7). Consequently, the India ink test has relatively low sensitivity, ranging from 50% to 80%, and may fail to detect Cryptococcus infection, especially in cases when the fungal burden is low (8–10). Despite these limitations, India Ink remains in routine use at many institutions, including our own at Memorial Sloan Kettering Cancer Center, and it continues to be featured in proficiency testing challenges by the College of American Pathologists (11).
To better understand the current role of this assay, we evaluated its clinical performance in our laboratory. We evaluated the clinical utility of India ink staining by reviewing its performance in our laboratory between January 2018 and August 2024. During this period, 457 cerebrospinal fluid (CSF) samples from 439 patients were tested for cryptococcal infection using India ink stain, CrAg LFA, fungal culture, and M/E multiplex PCR panel. The CrAg LFA was performed using the IMMY CrAg LFA kit (Immuno-Mycologics, Norman, OK) according to the manufacturer’s instructions. Briefly, CSF specimens were mixed with specimen diluent, and a lateral flow strip was inserted; results were read visually at 10 minutes. Semiquantitative titers were obtained by serial twofold dilutions (up to 1:2,560) as per the package insert (12, 13).
Among the 457 CSF samples reviewed, all positive results were identified by the CrAg LFA (n = 20); of these, 9 were also positive by the M/E panel, 6 by fungal culture, and 5 by India ink stain (Fig. 1). CSF specimens in this study were obtained both at the time of initial diagnosis and, in some cases, during treatment follow-up to monitor response or evaluate ongoing symptoms. Among the nine patients who tested positive by LFA, four contributed a single CSF sample; two contributed two samples each; two contributed three samples each; and one contributed six samples, accounting for the difference between the number of unique patients and the total number of CSF specimens analyzed.
Venn diagram of diagnostic tests positive for Cryptococcus neoformans. A total of 457 samples were tested by all four methods, with 20 samples resulting as positive, including 20 samples positive by the cryptococcal antigen lateral flow assay (LFA), 9 positives by the meningitis/encephalitis (M/E) panel, 6 positives by culture, and 5 positives by India ink.
Of the 439 patients from whom CSF was collected, only one was HIV positive and receiving antiretroviral therapy; the remainder were HIV negative, all with underlying malignancies, most commonly hematologic. None had received antifungal therapy prior to CSF collection, ensuring that diagnostic test sensitivity was not confounded by prior treatment. All positive results were confirmed as true cases of cryptococcal infection based on expert chart review by an infectious disease physician (author, S.M.), who assessed clinical presentation, treatment, and response, often in conjunction with infectious disease consultation. Notably, all cases were due to Cryptococcus neoformans; no cases of Cryptococcus gattii were identified.
Using culture as the gold standard, the sensitivity and specificity of India Ink was 42.8% and 99.4%, respectively, compared to 100.0% and 94.7% for the LFA and 100.0% and 99.3% for the M/E panel (Table 1). Notably, the sensitivity of India ink in our cohort was lower than the commonly cited range above. Several factors likely contributed to this reduced sensitivity. Because specimens were centrifuged prior to slide preparation, lack of centrifugation did not account for the diminished yield. Rather, the low fungal burden in many of our patients, particularly those with cancer and without HIV, likely contributed to false-negative India ink results (14–17).
The discrepancy between the cryptococcal antigen LFA and the M/E panel (20 LFA positive versus 9 M/E positive) likely reflects the superior sensitivity of the LFA. In subacute or treated cases, fungal burden may be low and fall below the detection threshold of the M/E panel, whereas the LFA can still reliably detect cryptococcal polysaccharide antigens. Although not the primary focus of this study, these findings underscore an important limitation of molecular testing in certain clinical contexts (1).
Beyond the discrepancy with the M/E panel, a comparable limitation was evident when evaluating culture and India ink against the LFA. In our study, 14 CSF specimens were culture negative but LFA positive, with clinical features consistent with cryptococcal meningitis, underscoring the limitations of culture in early or low-burden disease. Of these, India ink was negative in 11 cases and positive in 3, with the positives occurring only at high antigen titers (≥1:2,560) apart from a single lower-titer sample, highlighting the test’s poor sensitivity and its limited utility compared with antigen-based assays. These findings emphasize that the CrAg LFA is more sensitive than both culture and India ink, particularly when the fungal burden is low (18, 19).
While the CrAg LFA has largely replaced India ink due to its high sensitivity, simplicity, and availability, India ink may retain limited value in high-burden cases or when an LFA post-zone effect is suspected, and in institutions with limited on-site testing, it may serve as a rapid but low-yield adjunct while confirmatory testing is performed off-site (12, 15).
Overall, our results support the use of the CrAg LFA as the preferred frontline diagnostic test for cryptococcal meningitis while recognizing that India ink and culture retain limited utility in specific high-burden or confirmatory contexts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meya DB, Williamson PR. 2024. Cryptococcal disease in diverse hosts. N Engl J Med 390:1597–1610. doi:10.1056/NEJ Mra 231105738692293 · doi ↗ · pubmed ↗
- 2Kwizera R, Akampurira A, Williams D, Boulware DR, Meya DB, ASTRO-CM Study Team. 2017. Acridine orange fluorescent microscopy is more sensitive than India ink light microscopy in the rapid detection of cryptococcosis among Cr Ag positive HIV patients. P Lo S One 12:e 0182108. doi:10.1371/journal.pone.018210828750078 PMC 5531523 · doi ↗ · pubmed ↗
- 3Zhang X, Lin Y, Chen H, Hu J, Zhao H, Yang M, Han D. 2023. Diagnostic performance of metagenomic next-generation sequencing in central nervous system cryptococcosis using cerebrospinal fluid. Infect Drug Resist 16:6175–6183. doi:10.2147/IDR.S 42546337724093 PMC 10505399 · doi ↗ · pubmed ↗
- 4Rajasingham R, Govender NP, Jordan A, Loyse A, Shroufi A, Denning DW, Meya DB, Chiller TM, Boulware DR. 2022. The global burden of HIV-associated cryptococcal infection in adults in 2020: a modelling analysis. Lancet Infect Dis 22:1748–1755. doi:10.1016/S 1473-3099(22)00499-636049486 PMC 9701154 · doi ↗ · pubmed ↗
- 5Website. Casadevall A, Coelho C, Cordero RJB, Dragotakes Q, Jung E, Vij R, Wear MP. 2018. The capsule of Cryptococcus neoformans. Virulence 10:822–831. doi:10.1080/21505594.2018.143108729436899 PMC 6779390 · doi ↗ · pubmed ↗
- 6Abassi M, Boulware DR, Rhein J. 2015. Cryptococcal meningitis: diagnosis and management update. Curr Trop Med Rep 2:90–99. doi:10.1007/s 40475-015-0046-y 26279970 PMC 4535722 · doi ↗ · pubmed ↗
- 7Kwizera R, Kiiza TK, Akampurira A, Kimuda S, Mugabi T, Meya DB. 2024. Evolution of laboratory diagnostics for cryptococcosis and missing links to optimize diagnosis and outcomes in resource-constrained settings. Open Forum Infect Dis 11:ofae 487. doi:10.1093/ofid/ofae 48739282635 PMC 11398909 · doi ↗ · pubmed ↗
- 8Marcos JY, Pincus DH. 2013. Fungal diagnostics: review of commercially available methods. Methods Mol Biol 968:25–54. doi:10.1007/978-1-62703-257-5_223296883 · doi ↗ · pubmed ↗