Registration and reporting of clinical trials affiliated with California universities and with primary completion date from 2014 to 2017
Mario Malički, Vladislav Nachev, Susanne Wieschowski, Nicole Hildebrand, Stefanie Gestrich, Samruddhi Yerunkar, Emmanuel Zavalis, Benjamin Gregory Carlisle, Delwen L. Franzen, Maia Salholz-Hillel, Steven N. Goodman, Daniel Strech

TL;DR
This study examined how well clinical trials affiliated with California universities reported their results publicly from 2014 to 2017.
Contribution
The study provides empirical data on registration and reporting compliance of clinical trials affiliated with California universities.
Findings
Only 58% of trials reported results within 2 years of completion.
77% of journal publications were open access.
Only 2% of legally required trials were overdue for reporting.
Abstract
Public information on US clinical trials is shared through the ClinicalTrials.gov registry. This study’s goal was to determine prospective registration, results reporting, trial registration number reporting, and publication accessibility status for trials with primary completion dates from 2014 to 2017 affiliated with seven California universities. We identified trials with investigators, sponsors, or responsible parties affiliated with seven California universities and searched for their results publications manually. We then used semi-automatic methods to determine prospective registration, summary results reporting in a registry, publication status, and reporting of registration numbers in the abstract and the full text of manuscripts. We identified 1091 unique trials. Most trials were single-center (n = 752, 69%) and had a median of 50 participants (IQR 21 to 150). Overall, 64%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
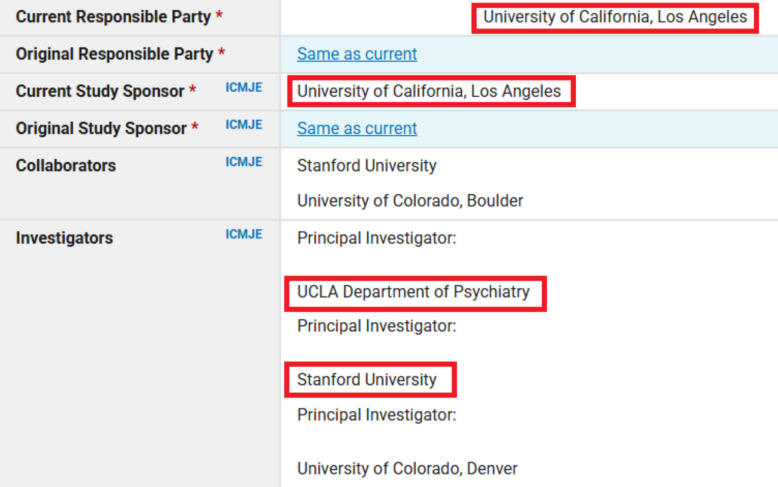 Figure 1
Figure 1- —Carl Erik Levins stiftelse
- —http://dx.doi.org/10.13039/501100017268Berlin Institute of Health
- —http://dx.doi.org/10.13039/100006521School of Medicine, Stanford University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEthics in Clinical Research · Meta-analysis and systematic reviews · Pharmaceutical industry and healthcare
Introduction
For clinical trials to generate useful and unbiased medical knowledge, trials should be registered before they start, and results should be reported after they are completed. These principles have been part of the Declaration of Helsinki since 2008 regarding registration and since 2013 regarding results reporting [1]. More recently, this guidance has become more specific, with recommendations that summary results are reported in a trial registry within 1 year of the trial’s primary completion date, and results being published in peer-reviewed journals within 2 years [2]. These ethical recommendations are relevant regardless of legal requirements, as lack of result reporting may lead to patient distrust in medical research, and biasing of results based on only published (positive) results.
The ClinicalTrials.gov trial registry was launched in 2000, and in 2008, it expanded to include summary results reporting [3]. The Food and Drug Administration Amendments Act of 2007 (FDAAA), and the later 2016 Final Rule for Clinical Trials Registration and Results Information Submission, applicable to specific US trials of drug, biological, or device products, makes US trial registration mandatory within 21 days of first patient enrollment and summary results reporting within 12 months of trial primary completion date. Similarly, the National Institutes of Health (NIH) 2016 Policy on the Dissemination of NIH-Funded Clinical Trial Information (effective from January 18, 2017) requires the same for clinical trials funded in whole or in part by NIH. Information in the ClinicalTrials.gov registry is self-reported by trial sponsors or investigators through a web-based Protocol Registration and Results System (PRS), with each entry having a set of mandatory data elements that are reviewed by the ClinicalTrials.gov staff. Each entry is also expected to be updated throughout the trial’s life cycle, with all changes made visible through the “History of Changes” links on the registry website [3].
Studies have shown that while trial registries are the only publicly accessible source of results information for thousands of trials [4], many trials are not prospectively registered [5], trials can have discrepancies between outcomes listed in their registration and their peer-reviewed publications, and not all trials have summary results reported [6–8]. Because of the latter, initiatives like the FDAAA TrialsTracker publicly track compliance [9]. In April 2025, according to TrialsTracker, 78% (20,039 of 25,691 trials) reported summary results within 1 year of primary completion [10].
While many universities monitor and enforce compliance of reporting for trials with legal reporting requirements, few monitor registration and results reporting that are not legally required. Furthermore, none to our knowledge monitor the reporting of results of trials with principal investigators from other institutions for which their faculty were co-investigators.
This study’s goal was to determine prospective registration, summary results reporting in the ClinicalTrials.gov registry, publication status, and reporting of trial registration numbers in the abstract and in the full text of publications of trials with a primary completion date from 2014 to 2017 whose investigators, sponsors, or responsible parties were affiliated with seven California universities (in alphabetical order: Stanford University, University of California – Davis, University of California – Irvine, University of California – Los Angeles, University of California – San Diego, University of California – San Francisco, University of Southern California). We chose this period to allow 5-year follow-up for all trials, and to be able to compare the results with those from our previous study about German trials with final completion dates from 2014 to 2017 [11]. We chose these universities, as they have the most published trials in California and would allow us to compare the findings to those previously reported for those universities regarding trials with completion dates from 2007 to 2010 [12].
Methods
Our study was registered with an analysis plan [13] and based on the methodology used in a prior analysis of trials by German University Medical Centers that are registered in ClinicalTrials.gov registry as well as the German Clinical Trials Registry [11, 14]. In short, we identified affiliated trials and obtained their metadata (slightly before the registration); then after study registration, we searched for trial results publications manually. We then used semi-automatic methods to determine the open access (OA) status of journal publications, the time from trial start to its registration and result publication, as well as the reporting of trial registration numbers in the abstract or full text of publications (with details of each method listed below in the following sections). A deviation from our original protocol was the inclusion of two additional data extractors (EZ, NH) who extracted the data for 250 trials, as well as a project supervisor (SM), with all three individuals added as co-authors on this publication.
Another addition was the inclusion of trials from the University of Southern California (USC). USC was not analyzed in a previous publication that reported data for US trials completed from 2007 to 2010, as that study included only universities with more than 40 trials in the time period, and so we did not include it in the protocol [12]. However, we felt that due to the recent number of trials conducted by USC, it should be included. Additionally, while we wanted to showcase trial funding data and explore it as a possible predictor of practices, details of funding were not available through the metadata sources we used. We did not collect this information manually due to time constraints. Furthermore, although originally planned, statistical comparison of our results with those reported for trials from German University Medical Centers [11] was deemed inappropriate due to differences in the selection criteria (primary completion date in our study vs final completion date in German data). We therefore report that comparison only descriptively in our results section.
Outcomes
We aimed to assess (in order presented in the results):
Primary objectives:
- Timing of trial registration (prospective vs retrospective)
- Summary results reporting on ClinicalTrials.gov registry (total, and within 2 and 5 years of trials’ primary completion date)
- Results reporting in publications (peer reviewed publications, abstract or posters, as well as within 2 and 5 years of trials’ primary completion year).
- Any form of result reporting (i.e., summary results reporting and results publication described above)
- Linking of a results publication in the ClinicalTrials.gov registry
- Trial registration number reporting in the publication abstract and full text
- Open access status of peer reviewed publications
The 2-year and 5-year periods for availability of results were chosen to align with outcomes of our previous study on German trials [11].
Secondary objectives:
- Comparison of results with published data from German trials with final completion dates between 2014 to 2017 [11]
- Comparison of results with published data from US trials with primary completion dates from 2007 to 2010 [12]
Trial identification, inclusion criteria, and reporting
We identified interventional trials by using the Clinical Trials Transformation Initiative’s Aggregate Content of ClinicalTrials.gov (AACT) database (a publicly available relational database that contains all information about the protocol and result data elements about every study in ClinicalTrials.gov registry). We did this via the aactr package (RRID:SCR_026245) and searched “overall officials,” “sponsors,” and “responsible parties” fields using name variants and abbreviations of the seven California universities (“sponsors” field was searched only for the sponsor, not the collaborators’ entries). We then excluded trials with withdrawn status (i.e., those with zero participants recruited, as well as those with unknown status). Trials that were terminated (i.e., stopped recruiting participants), or still active, or suspended (i.e., halted but potentially will resume), were included, as they also have an obligation to report results for all patients enrolled. We downloaded all such trials and filtered that dataset for trials with a primary completion date (defined as the date that the last data point for the primary outcome measure was collected from the last enrolled participant) from 2014 to 2017. All R (RRID:SCR_001905) scripts used to retrieve, combine, and filter the trials, as well as populate metadata about the trials can be found at our project's GitHub (RRID:SCR_002630) repository [15]. We removed duplicates and verified the data with manual checks. In the presentation of summary results, each unique trial was counted only once. In the presentation of trials affiliated with a university, if a trial’s “overall officials,” “sponsors,” or “responsible parties” field had individuals from more than one California University, we counted those trials as affiliated with each of those universities (Fig. 1). Specifically, in our sample there were 1091 unique trials, 1072 (98.3%) were affiliated with only one university, 17 (1.6%) were affiliated with two universities, and 2 (0.1%) were affiliated with three universities.Fig. 1. Example of identification and classification of a trial affiliated with two California universities. Figure legend: The figure is a screenshot from the Clinical Trial Registry record NCT01483391, under the category “Administrative information.” We removed the names of the individuals and added red frames around affiliations to California universities identified by our search strategy that searched for names and acronyms of seven California universities. For summary results reporting, this trial was counted once, and when reporting results for trials affiliated with individual universities, it was counted twice, i.e., it was included in results of trials affiliated with Stanford University and with University of California, Los Angeles
Under FDA and NIH regulations only one university, i.e., commonly the university whose Protocol Registration and Results System (PRS) trial account is used to register the study, holds the legal and contractual responsibility for trial registration and results reporting in the public registry, and is listed as the lead sponsor of the study in ClinicalTrials.gov registry. However, ClinicalTrials.gov registry and the related AACT database do not have fields which indicate what trials fall under FDAAA regulations (i.e., Applicable Clinical Trials) or the NIH mandates, nor does AACT contain a specific PRS Account field, i.e., a field that specifies which entity is responsible for reporting trial results. Therefore, the results presented here should not be interpreted as related to legal or funder mandates. Instead, the results should be viewed in relation to ethical recommendations for all parties involved (e.g., Declaration of Helsinki: “Researchers, authors, sponsors, editors and publishers all have ethical obligations with regard to the publication and dissemination of the results of research”) [1]. Also applicable are the principles of ethical research which specify that the burden on trial participants should be commensurate with a trial’s scientific value, which equals zero if the results are not publicly reported, and are markedly diminished if reporting is not timely [16]. This ethical requirement applies to all trials and trial investigators, not just to the PI, first author, sponsor, or other responsible party.
Results publication search
Data extractors applied a 3-step process for identifying results publications:
- They first manually checked if a publication of results was linked in the ClinicalTrials.gov registry. If multiple publications were linked, the earliest publication in which primary outcomes were reported was chosen.
- If the results publications were not linked in the registry, the clinical trial identifier (NCT ID) was entered in Google search, and the first two pages of search results were checked for possible results publications.
- If results publications were not identified using steps 1 and 2, extractors then used the title of the trial and the name of the principal investigator as a Google search query. When multiple investigators were listed, individual searches were repeated using the trial title and the name of the other investigator(s). The first two pages of results were checked.
When a publication was found, the Digital Object Identifier (DOI) or link and (where available) PMID were extracted for that publication and entered in a database. The date of publication for all trials with a PMID was extracted from PubMed, with detailed steps reported in our Appendix. For those without a PMID, the date of publication was extracted manually. We also extracted data on whether the results were linked in the registry or found through a Google search, and what type of results were reported:
- Summary results only (i.e., in the registry)
- Peer-reviewed article or preprint with results, or
- Other (e.g., conference abstract, poster, or presentation slides)
Data extraction was split among six extractors (in alphabetical order by first name: EZ, MM, NH, SY, SG, SW). Extractors were first trained on 30 trials. Raters, on average, identified correct results reporting for 24 out of 30 trials, reaching the target 80% agreement threshold set in our protocol. Additionally, as stated in our protocol, for each trial without identified reporting of results by one of the extractors, a second extractor repeated the full search process. Any discrepancies were resolved by consensus or through consultation with the data extraction lead (SW).
Determining prospective registration
We used two methods to explore if a trial was prospectively registered:
- Month approach (reported in the main results)—we considered the trial prospectively registered if it was registered before or in the month of the trial start date. This method was used in previous studies [11, 12] and allows leniency, as 84% of trials in our sample lacked information on which day of the month the registration occurred (i.e., only month and year information was available, see Appendix Extraction of Dates).
- Twenty-one-day approach (reported in the Appendix)—we considered the trial to be prospectively registered if it was registered within 21 days of the start date, as mandated by NIH and FDA regulations [17]. For leniency, dates that lacked information on days were transformed to the end of month (see Appendix Extraction of Dates).
Determining the time to publication
Publication dates were extracted from three sources and the earliest of all three times was used. The three sources were: 1) manual extraction during identification of publication; 2) PubMed; and 3) Unpaywall database. The Unpaywall database is a publicly available database that collects data on locations where each scientific publication can be legally accessed from, such as repositories and publisher websites, as well as the accessibility at each location. For dates available through PubMed, we obtained both the publication date and the electronic publication date if it was available (for details see Appendix Extraction of Dates).
Determining open access status
Open accessibility of trials with results published in peer-reviewed publications was assessed using the Unpaywall API (accessed on 2024-02-08) [18], except for two publications which were not in the Unpaywall database and were assessed manually. We counted as openly accessible gold, green, and hybrid publications.
Statistical analysis
Summary trial (meta)data is reported as the number and percentage of unique trials (N = 1091) for all categorical characteristics. Trial recruitment size is shown as median and interquartile range (IQR) due to skewed data distributions. Trials that were affiliated with more than one institution were allocated to each institution. Specifically, 19 (1.7%) trials were affiliated with more than one institution; 17 (1.6%) with two institutions, and 2 (0.1%) with three institutions, making the total sample size N = 1112 for these analyses. Differences in outcomes between the trials affiliated with different universities were compared using a series of chi-squared tests, and differences between trials based on their primary completion year, using a series of chi-squared tests for trend. Comparison with data from the Chen et al. study, covering US trials from 2007 to 2010 [12], was done with chi-squared tests. All data was analyzed using MedCalc v.22.017 (RRID:SCR_015044) or Microsoft Excel v.2211 (RRID:SCR_016137), and statistical program result outputs are available in our project repository.
Results
Trial characteristics
We identified 1091 unique trials affiliated with seven California universities registered on the ClinicalTrials.gov trial registry that had a primary completion date between 2014 and 2017 (Table 1). All trials were interventional; the majority were no-phase (e.g., studies of devices or behavioral interventions, n = 589, 54%), followed by phase 2 studies (n = 159, 15%, Appendix Table 1). Most trials were single-center (n = 752, 69%) and had a median recruitment size of 50 participants (IQR 21 to 150). The majority had the status completed (n = 921, 84%), followed by terminated (n = 154, 14%), active–not recruiting (n = 11, 1%), and suspended (n = 5, 0%). Table 1. Prospective registration, (summary) results reporting and open accessibility of results for clinical trials with primary completion year from 2014 to 2017 affiliated with seven California universitiesInvestigator, sponsor or responsible party affiliation (n, %)(Affiliation does not reflect legal responsibility)^a^Prospectively registeredSummary results in ClinicalTrials.govJournal publicationAbstract/posterOpen access^c^Stanford University (N = 266)162 (61)160 (60)173 (65)4 (2)120 (69)UC Davis (N = 110)60 (55)37 (34)82 (75)4 (4)61 (74)UC Irvine (N = 41)12 (29)25 (61)23 (56)3 (7)15 (65)UC Los Angeles (N = 188)136 (72)74 (39)128 (68)2 (1)107 (84)UC San Diego (N = 127)85 (67)68 (54)83 (65)5 (4)68 (82)UC San Francisco (N = 299)220 (74)117 (39)228 (76)13 (4)190 (83)University of Southern California (N = 81)40 (49)28 (35)52 (64)5 (6)35 (67)Total (N = 1112)^b^715 (64)509 (46)769 (69)36 (3)596 (78)^a^We defined a trial as affiliated with a university if the university or one of its investigators was mentioned in one of the following fields of the ClinicalTrials.gov registry entries “Overall Official,” “Responsible Parties,” or “Sponsors.” See the “Methods” section for more details^b^Trials affiliated with more than one university were counted for each university (i.e., there were 1091 unique trials, of which 1072 were classified as affiliated with 1 California university, 17 with two California universities, and 2 with 3 California universities)^c^Counted for open access are gold, green, and hybrid versions of journal publications. Denominator for this column was the number of trials with journal publications, while for all other columns the total number of trials
Trial registration
Overall, 64% of trials (n = 698) were prospectively registered. Prospective registration statistically differed between trials affiliated with different universities (P < 0.0001, chi-square test, Table 1), and per trial primary completion year, increasing from 52% for trials with primary completion in 2014 to 71% for those with primary completion date in 2017 (P < 0.0001, chi-square for trend). Additional details on prospective trial registration are presented in the Appendix Trial Registration section.
Summary results reporting in the ClinicalTrials.gov registry
Summary results were reported on ClinicalTrials.gov registry for 29% of trials (n = 313) within 2 years of their primary completion date, and for 44% of trials (n = 475) within 5 years. This increased to 46% (n = 500) of all trials in a period of more than 5 years after completion (Appendix Table 2). Summary results reporting statistically differed among trials affiliated with different universities (P < 0.0001, chi-square test, Table 1), and per trial primary completion year (i.e., 2014 to 2017, P = 0.0097, chi-square for trend).
Results reported in publications
For 46% (n = 507) of trials, publication (e.g., article, abstract or poster) occurred within 2 years of the primary completion date, and for 69% (n = 754) within 5 years (Appendix Table 3). This increased to 72% (n = 786) in more than 5 years after completion, with 69% (n = 750) of trials published as journal peer-reviewed articles, and an additional 3% (n = 36) as only abstracts or posters. Publication rates statistically differed among trials affiliated with different universities (P = 0.0026, chi-square test, Table 1), with no statistically significant differences per primary completion year (P = 0.6929 chi-square test for trend).
Any form of results reporting
Primary results were reported in any form within 2 years of trials’ primary completion date for 58% (n = 637) of trials, and for 81% (n = 888) of trials within 5 years. This increased to 84% (n = 919) in a period of more than 5 years after completion. Publication rates did not statistically differ among trials affiliated with different universities (P = 0.1146, chi-square test, Appendix Table 4), nor per primary completion year (P = 0.0773 chi-square test for trend). For the 14% (n = 154) of trials listed as terminated early, 49% (n = 76) had results disseminated within 2 years, and 68% (n = 105) within 5 years.
Linked publications and reporting of trial registration numbers
Only 58% (n = 438) of the 750 trials with results published as peer-reviewed journal articles linked to the article in the trial registry. Linking to the articles in the registry did not statistically differ among trials affiliated with different universities (P = 0.5188, chi-square test, Appendix Table 5), nor per study primary completion year (P = 0.900, chi-square test for trend).
The trial registration number was listed in the abstract of the associated results publication in 37% (n = 276) of articles, and in the manuscript (or declarations) in 45% (n = 336) of articles. Trial registration number reporting in abstracts statistically differed among trials affiliated with different universities (P = 0.0027, chi-square test) and per study primary completion year (P = 0.0401 chi-square test for trend).
Trial registration number reporting in manuscripts did not statistically differ among trials affiliated with different universities (P = 0.2399, chi-square test), nor per study primary completion year (P = 0.2695, chi-square test for trend).
Open access status of results publications
Out of the 750 trials with results published as peer-reviewed journal articles, 77% (n = 579) were published in open access journals, of which 48% (n = 360) were green open access, 22% (n = 163) gold, and 7% (n = 56) hybrid. Open access rates statistically differed among trials affiliated with different universities (P = 0.0025, chi-square test, Table 1), and per primary completion year (P = 0.0397, chi-square test for trend).
Comparison with German trials from 2014 to 2017
In Table 2, we display our data with those from German University Medical Centers. As the present sample included trials with primary completion dates (last day of data collection for primary study outcomes) from 2014 to 2017, while the German sample included trials from ClinicalTrials.gov registry and German Clinical Trial Registry that had final completion dates (last day of data collection for all study outcomes) from 2014 to 2017, no statistical comparisons were made. Table 2. Comparison with German trials registered in ClinicalTrials.govTrials (n, %)Prospectively registeredSummary results in ClinicalTrials.govJournal publicationOpen accessaGermany (2014 to 2017, N = 1213)681 (56)^a^93 (8)794 (65)454 (59)^b^California (2014 to 2017, N = 1091)698 (64)500 (46)750 (69)579 (77)^a^Sample 1211—two trials had no start date in the database^b^Sample denominator was 765, as those publications had Unpaywall information
Comparison within USA
Chen et al. included data from California trials with primary completion dates from October 2007 to September 2010 that were affiliated with academic medical centers that in that period had more than 40 trials (14). Results were searched from January to July 2014. Overall, 2892 (67%) of the 4347 clinical trials had been published or reported results as of July 2014, of which 1560 (36%) trials had been disseminated within 24 months. Direct comparisons of data from California universities are shown in Table 3 for summary results reporting in the registry within 2 years, in Table 4 for results reported in publications within 2 years, and in Table 5 for any form of results reporting (note: University of Southern California was not analyzed in Chen et al. due to having less than 40 trials at the time). Table 3. Comparison of summary results reported in ClinicalTrials.gov within 2 years for trials with primary completion year between 2007 and 2010 and those between 2014 and 2017UniversityPercentage (n/N) of trials with summary results reported inPChen et al. study (2007 to 2010)**This study (2014 to 2017)**Stanford University3 (4/131)39 (104/266) < 0.0001UC Davis2 (1/64)22 (24/110)0.0002UC Irvine31 (13/42)41 (17/41)0.3219UC Los Angeles6 (6/95)30 (57/188) < 0.0001UC San Diego11 (8/75)24 (31/127)0.0171UC San Francisco16 (21/133)22 (65/299)0.1533Chi-squared testTable 4Comparison of results reported in publications within 2 years for trials with primary completion year between 2007 and 2010 and those between 2014 and 2017UniversityPercentage (n/N) of trials with publications reported inP**Chen et al. study (2007 to 2010)**This study (2014 to 2017)**Stanford University26 (34/131)44 (116/266)0.0007UC Davis34 (22/64)52 (57/110)0.0263UC Irvine29 (12/42)37 (15/41)0.4387UC Los Angeles31 (29/95)44 (83/188)0.0272UC San Diego35 (26/75)44 (56/127)0.1885UC San Francisco30 (40/133)51 (152/299)0.0001Chi-squared testTable 5Comparison of any form of results reporting for trials with primary completion year between 2017 and 2010 and those between 2014 to 2017UniversityPercentage (n/N) of trials with any form of results reporting reported inP***Chen et al. study (2007 to 2010)***This study (2014 to 2017)**Stanford University54 (71/131)85 (227/266) < 0.0001UC Davis69 (44/64)84 (92/110)0.0223UC Irvine62 (26/42)88 (36/41)0.0070UC Los Angeles68 (65/95)78 (147/188)0.0739UC San Diego63 (47/75)86 (109/127)0.0002UC San Francisco74 (99/133)88 (263/299)0.0004Chi-squared test
Discussion
Our study has shown that about one fifth (19%) of 1091 trials with investigators, sponsors, or responsible parties affiliated with seven California universities with primary completion dates from 2014 to 2017 lacked any kind of results dissemination (e.g., summary results in registry, journal article, poster or abstract) 5 years after their primary completion date. While 58% of trials had results disseminated within 2 years, less than half (46%) reported summary results on ClinicalTrials.gov registry. These results are similar to those recently published for a random sample of 400 US trials initiated after 2015 with primary completion dates prior to 2018, for which 48% reported summary results [19]. While summary results reporting in our sample increased compared to the period from 2007 to 2010 [12], and was higher than that reported for Canadian [20], German [11], or Polish trials [21] registered on ClinicalTrials.gov registry, they are still lower than for trials covered by the FDAAA (or NIH) mandates (77% reporting of summary results in the registry) [10], indicating that such mandates, even when not imposing or enforcing financial penalties for non-reporting, seem to increase trial summary results reporting.
Furthermore, our findings of clinical trial registration numbers being reported in 37% of publication abstracts, and in 45% of manuscripts, is slightly lower than that reported for German trials (38% and 60%, respectively) [14], and in a random sample of 200 USA trials, where trial number linkage in the abstract was present for 55% of trials with results publications [22]. The open access status of publications in our study was 77%, which was higher than 59% of German trials (though that also included bronze as open access) [23].
International guidelines such as the Declaration of Helsinki [1] and WHO Joint Statement [2] provide clear ethical recommendations for prospective trial registration and results reporting, with WHO specifying timely dissemination as summary results reporting within 12 months and journal publication within 24 months after completion. However, legal and institutional requirements around the world vary as to whether and how they regulate or enforce these recommendations. To ensure compliance with both ethical principles and regulatory requirements, universities need effective monitoring and support systems. Especially, when it seems unlikely that the legal requirements will in the future also cover these past trials. And with the passing of time, it will become difficult, if not impossible, to retroactively update the results for these trials, and fulfill the ethical obligations to the patients enrolled in them. Possible approaches include creating dashboards similar to FDAAA Trials Tracker [10], checklists [24], or report cards [25], and having dedicated support staff to help with the monitoring and reporting of results [26].
This study has several limitations and important caveats. First, as we employed manual and semi-automatic searches and did not contact principal investigators directly, it is possible that some results reporting was missed or that we did not pick the earliest results reporting study. In a follow-up of the German study, 6% of trial publications were either not identified or wrongly identified based on the PI feedback. This did not affect the 2-year and 5-year publication rates in that sample [27].
Second, we included all trials in results reporting, even those with terminated status, as 33% of those in our sample reported results. Some terminated trials may not have recruited any participants or updated their registrations to a withdrawn status. Other terminated trials may have recruited so few participants that results would be uninformative, although the results reporting rate of such trials was only modestly lower than for other trials.
Third, while we examined differences between the California universities, and between trials with different primary completion years, any difference among them may be due to trial characteristics that were not captured in our study, such as characteristics of researchers.
Fourth, as we used Google for our searches, publication status results are not reproducible due to continual changes with Google’s indexing processes.
Finally, we repeat the caveat that these results should not be interpreted as related to legal or funder mandates, because analysis of legal liability was not our objective. Our study included trials with primary completion dates between 2014 and 2017, while the FDAAA 2007 Final Rule came into force in January 2017. According to the FDAAA Trials Tracker, only 92 (8%) of trials in our study are subject to the FDAAA mandate. Of these 92, 65 (71%) were reported late, and 9 (10%) were still overdue to report their results in January 2025. Of the 9 overdues, only 2 have California universities as the PRS account holders, i.e., as responsible parties for reporting of results. So, of those trials that were legally required to report results, only 2.1% (2/92) were overdue and the primary responsibility of a California university to report.
In conclusion, our study has shown that timely results reporting may be improving, but for studies completed in 2014–2017, most of which were not subject to FDA or NIH reporting requirements and mandates, 2-year results are suboptimal, and even 5-year results reporting has substantial room for improvement.
Supplementary Information
Supplementary Material 1. Appendix.Supplementary Material 2. STROBE checklist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WMA - The World Medical Association-Declaration of Helsinki. Available from: https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/. Cited 2024 Oct 24.
- 2Joint statement on public disclosure of results from clinical trials. Available from: https://www.who.int/news/item/18-05-2017-joint-statement-on-registration. Cited 2024 Oct 24.
- 3History, Policies, and Laws - Clinical Trials.gov. Available from: https://clinicaltrials.gov/ct 2/about-site/history#Final Rule FDAAA 801. Cited 2023 Mar 14.
- 4Zarin DA, Fain KM, Dobbins HD, Tse T, Williams RJ. 10-Year Update on Study Results Submitted to Clinical Trials.gov. N Engl J Med. 2019;381(20):1966–74.10.1056/NEJ Msr 1907644 PMC 859166631722160 · doi ↗ · pubmed ↗
- 5Holst MR, Carlisle BG. Trials that turn from retrospectively registered to prospectively registered: A cohort study of ‘retroactively prospective’ clinical trial registration using history data. med Rxiv. 2022:2022.10.25.22281505. Available from: https://www.medrxiv.org/content/10.1101/2022.10.25.22281505 v 1. Cited 2023 Mar 15.10.1186/s 13063-024-08029-5PMC 1093867738486299 · doi ↗ · pubmed ↗
- 6Who’s sharing their clinical trial results?. Available from: https://fdaaa.trialstracker.net/. Cited 2025 Apr 1.
- 7Wieschowski S, Strech D, Franzen D, Salholz-Hillel M, Carlisle BG, Malički M, et al. CONTRAST – Calif Or Nia T Ri Al S Transparency. 2022. Available from: https://osf.io/u 9d 5c/. Cited 2023 Apr 21.
- 8Federal Register. 2016. Clinical Trials Registration and Results Information Submission. Available from: https://www.federalregister.gov/documents/2016/09/21/2016-22129/clinical-trials-registration-and-results-information-submission. Cited 2024 Feb 8.27658315 · pubmed ↗