Anxiety, depression and distress in family members of people who have experienced a critical care admission: a systematic review and Bayesian meta-analysis
P. Hartley, C. Brown, V. Danesh, F. Forsyth, K. Bond, I. Kuhn, M. Shaw, J. McPeake

TL;DR
This study finds that family members of critical care patients often experience anxiety and depression, with about 38% and 20% showing clinically significant levels, respectively.
Contribution
The study uses Bayesian meta-analysis to quantify distress, anxiety, and depression in family members of critical care patients, revealing clinically meaningful proportions.
Findings
38% of family members showed clinically significant anxiety (HADS-A > 7) at 3 months.
20% of family members showed clinically significant depression (HADS-D > 7) at 3 months.
Pooled IES-R score indicated moderate distress levels in family members post-discharge.
Abstract
Family members of adults who experience a critical care admission often experience significant strain and emotional distress following discharge. This meta-analysis aimed to synthesise the levels of distress, anxiety, and depression in family members of people who have experienced a critical care admission. Medline, PsycINFO, Scopus, CINAHL and Web of Science databases were searched for articles (2000–2024) that measured distress using the Impact of Events Scale—Revised (IES-R), or anxiety or depression using the Hospital Anxiety and Depression Scale subscales (HADS-A and HADS-D) 3 months after critical care. Bayesian meta-analyses estimated the pooled average, and meta-regression examined whether the inclusion of bereaved relatives influenced the pooled outcome estimates. Anxiety and depression models estimated the pooled proportion of participants with HADS scores >7. Fifty articles…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
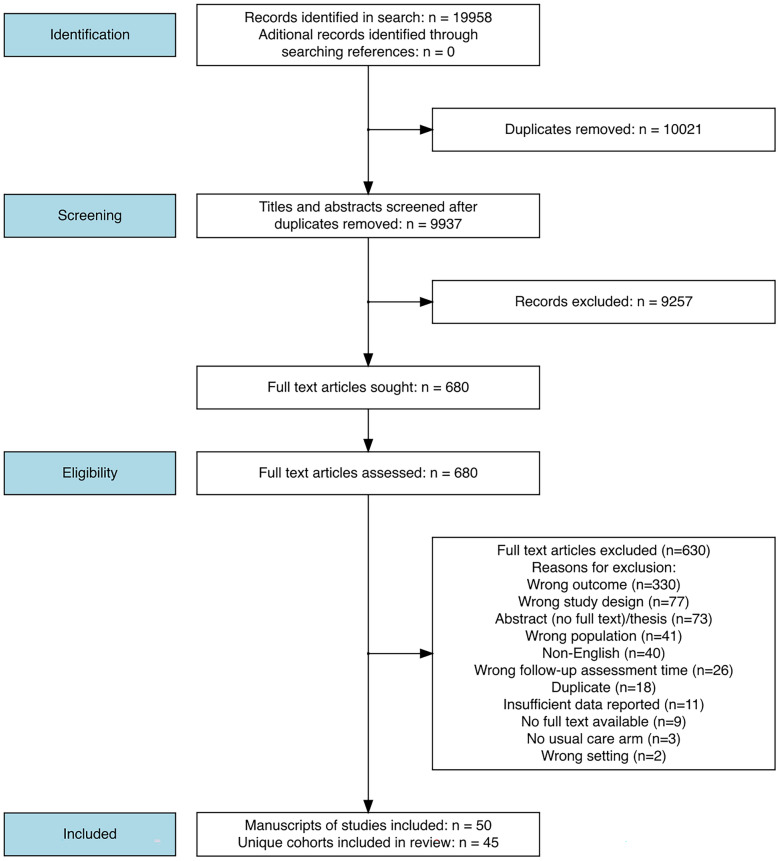 Figure 1
Figure 1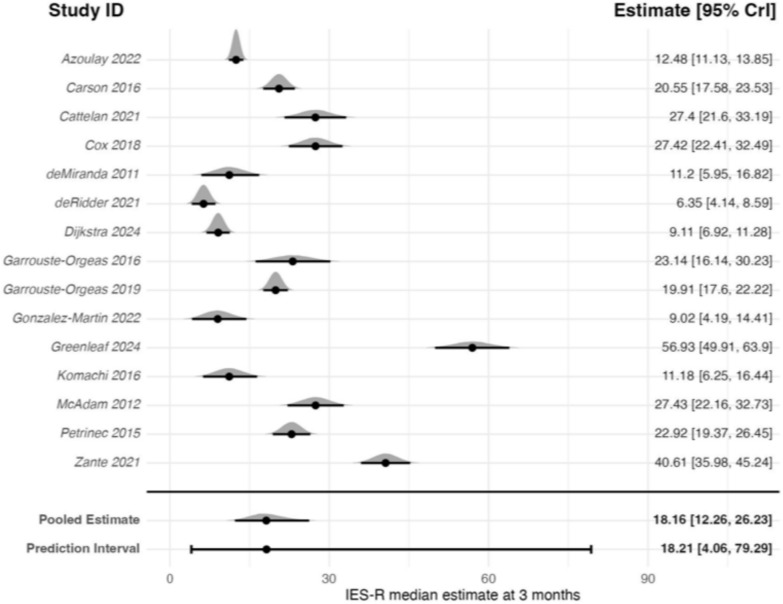 Figure 2
Figure 2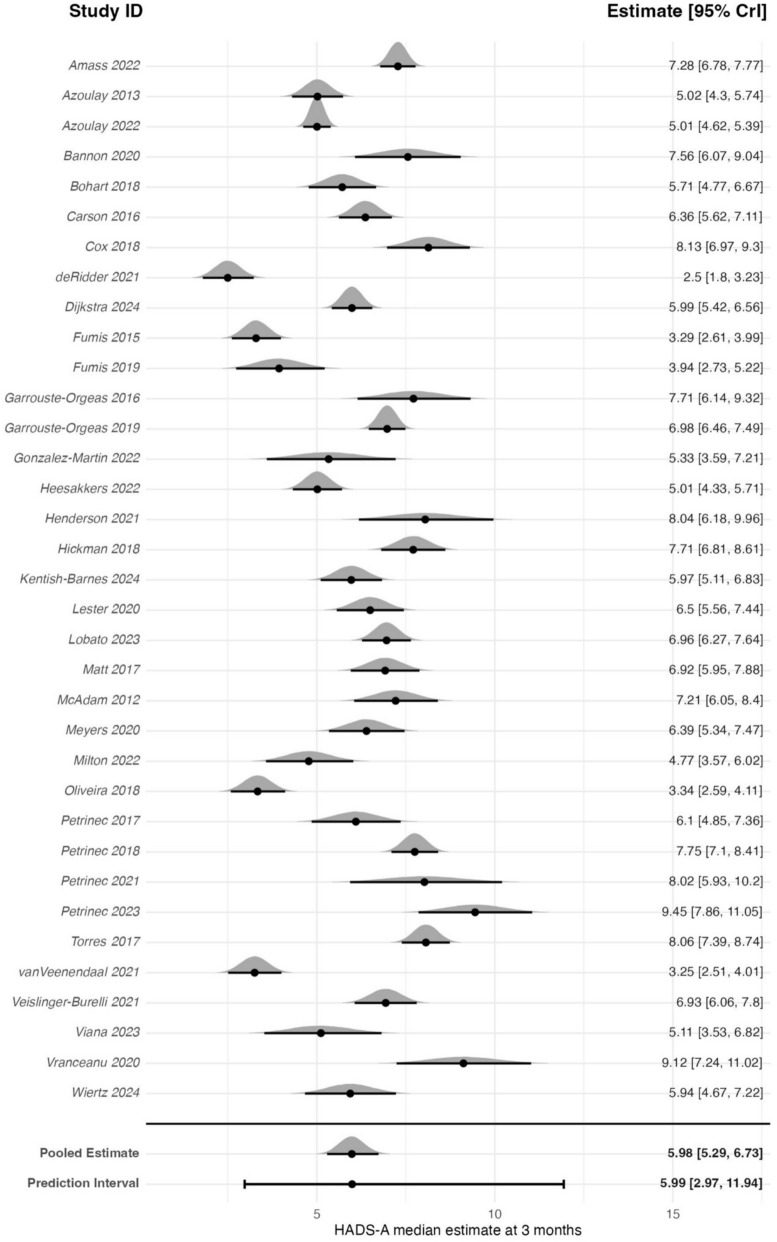 Figure 3
Figure 3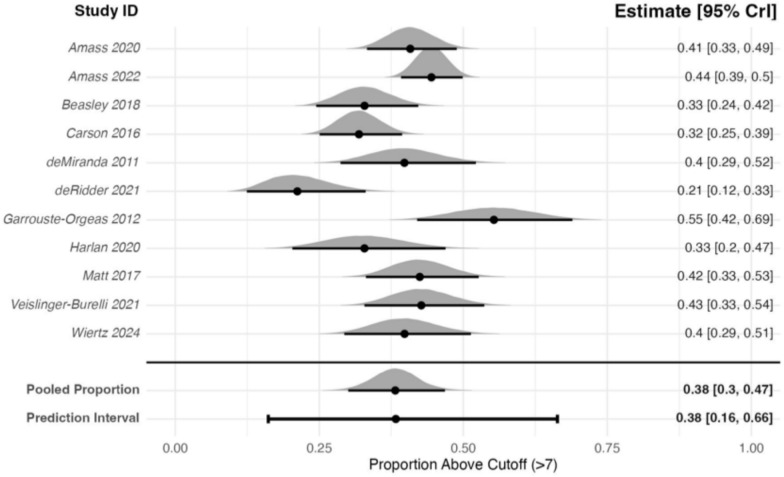 Figure 4
Figure 4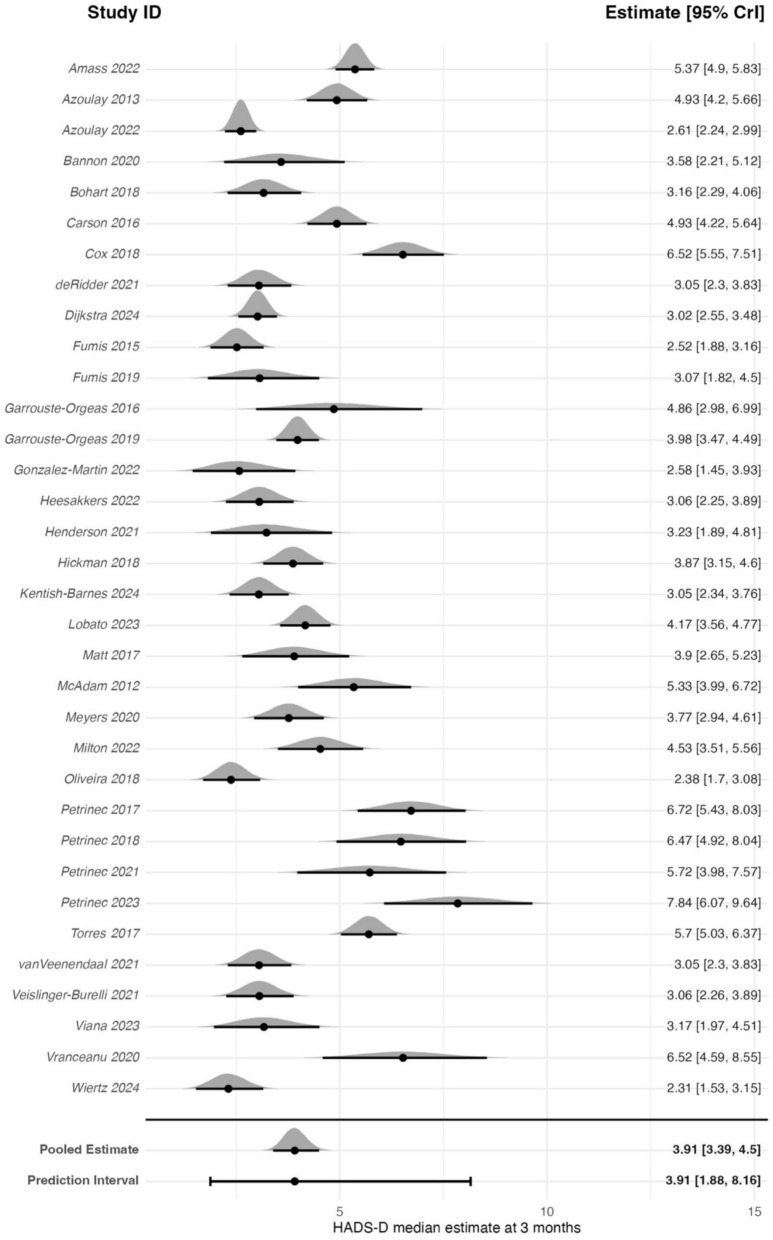 Figure 5
Figure 5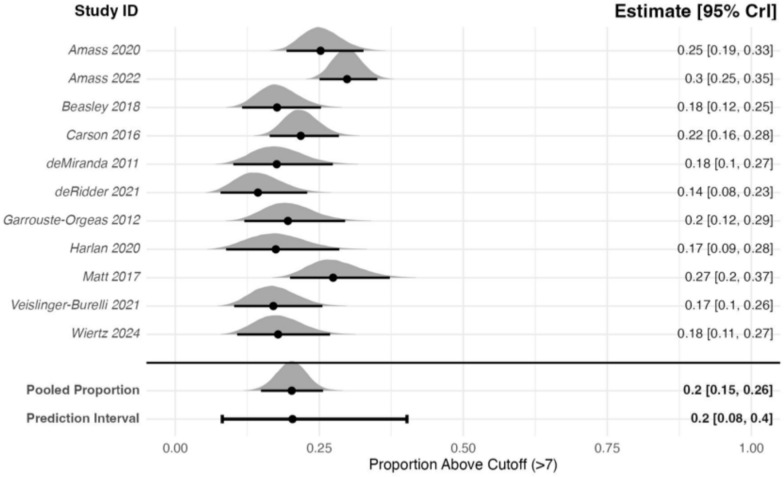 Figure 6
Figure 6- —https://doi.org/10.13039/501100022512THIS Institute, University of Cambridge
- —https://doi.org/10.13039/501100008420Homerton College, University of Cambridge
- —https://doi.org/10.13039/501100018956NIHR Cambridge Biomedical Research Centre
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFamily and Patient Care in Intensive Care Units · Intensive Care Unit Cognitive Disorders · Family Caregiving in Mental Illness
Background
The number of patients surviving an admission to critical care is increasing [1]. As a result, there is greater recognition of the challenges faced by those who have experienced a critical care admission [2]. Following discharge, many experience ongoing physical, emotional, cognitive and social problems [3]. Consequently, many family members adopt the role of informal caregiver [4].
Evidence demonstrates that these family members also experience significant strain and emotional distress following hospital discharge for critical illness [5, 6]. For example, multi-centre data from Canada found that over two-thirds of informal caregivers experienced symptoms of depression in the months following critical care [7]. Similar findings have been reported in the UK, with up to 70% reporting symptoms of anxiety, and 40% experiencing financial strain [8]. Greater caregiver strain in informal caregivers is associated with an increased risk of hospital readmission for the person recovering from the critical care admission [9]. Despite descriptive research examining the outcomes of informal caregivers, there is limited high quality interventional research examining how their outcomes can be improved. Interventions including online resources and telephone support have been evaluated; but none have shown benefit in a randomised control trial (RCT) [10].
Given the pressing need to support family members, a comprehensive understanding of their experiences following a critical care admission is needed. With a substantial body of literature now available [11], this represents a timely opportunity to synthesise the evidence to inform clinical practice and to identify priorities for research, including the development of targeted interventions. Therefore, we conducted a systematic review and meta-analysis which synthesised levels of anxiety, depression, and distress in family members of people who have experienced a critical care admission. To inform clinical care planning and interventional research in this area, we used Bayesian methods to estimate posterior probabilities of the incidence of anxiety, depression and distress in family members.
Methods
Ethical review was not required as this systematic review and meta-analysis only involved reviewing existing literature.
Search strategy
Medline, PsycINFO, Scopus, CINAHL and Web of Science (Core Collection) databases were searched for publications between 2000 and 2024. We chose a start date of 2000 to reflect contemporary research and practice. The full search strategy is provided in the online supplementary materials (e-Tables 1–6), and was developed with an experienced medical librarian.
Eligibility
We included published studies of any design that assessed distress, anxiety, or depression in family members of critically ill patients. Studies used multiple descriptions of informal caregivers, family members and loved ones. For this review, we have included all under the umbrella term of family members. Family members of patients who received care in any critical care setting, including general, neurological, or cardiac critical care units were included.
We excluded studies focused on bereavement of family members of people who died during critical care admission or before the follow-up assessment, but included mixed samples of family members of people who were alive at follow-up and of people who had died during follow-up. We excluded studies, where all participants received an intervention to influence anxiety, distress or depression in family members and retained data from control arms when applicable. Studies published only as abstracts, conference proceedings, theses, or non-English language studies, and those focused on neonatal and paediatric populations were excluded. We also excluded case reports, reviews, letters, and editorials.
Outcomes
Studies that reported the Impact of Events Scale—Revised (IES-R) or the anxiety or depression subscales of the Hospital Anxiety or Depression Scale (HADS) were included. These were chosen as they were the most frequent measures used in studies of family members of adults admitted to critical care [11]. The decision to exclude other measures of distress, anxiety, or depression was made to reduce conceptual and statistical heterogeneity that could potentially be introduced by multiple measures with different properties and which do not necessarily measure the same construct. Given our a priori knowledge of the size of the available data [11], this decision was felt to be justified from a pragmatic stance as striking a balance between the comprehensiveness of the review, and a desire to maximise the coherence through attempting to reduce heterogeneity and optimising comparability and interpretation.
The IES-R consists of 22 items measuring the degree of distress an individual experiences in response to a traumatic event, with 8 items measuring intrusion, 8 items measuring avoidance, and 6 measuring hyperarousal [12]. Each item is rated on a five-point Likert scale from 0 (“not at all”) to 4 (“extremely”), giving a total score between 0 and 88, with higher scores indicating greater symptom severity [12].
The HADS consists of 14 items assessing mood, with 7 items measuring anxiety (HADS-A) and 7 measuring depression (HADS-D) [13]. Each subscale ranges from 0 to 21, with higher scores indicating greater levels of symptom severity. Scores of >7 on either subscale are considered indicative of clinically meaningful symptoms of anxiety or depression, respectively [13].
For the IES-R we excluded studies that only reported the proportion of individuals above or below a threshold on the scale. Although it is an endorsed tool to use in this population [2, 14], the clinical interpretation of a score above or below a threshold is questionable as it does not capture symptom domains necessary for a diagnosis of PTSD according to DSM-5 criteria [15, 16]. For the HADS outcomes we included studies that reported sample averages or proportion of study participants above or below 7 on the subscales (HADS-A or HADS-D).
We only included studies that reported the outcomes at 3 ± 1 months after critical care. As studies’ definitions of follow-up periods and admission durations varied, the timepoints could be 3 ± 1 months from any point between critical care admission and critical care discharge. The follow-up window of 3 ± 1 months was chosen as this was the most frequent assessment timepoint in the scoping review by Brown et al. [11] of all outcomes of family members of critically ill patients.
Selection of studies
Two reviewers independently examined all titles and abstracts using predefined eligibility criteria. If a reason for exclusion from reading the title or abstract was not evident the article proceeded to full-text screening and the full manuscript was obtained. Full-text screening was also undertaken independently by two reviewers, with disagreements resolved by a third author.
Data extraction
For interventional studies, only control group data were extracted. Relevant data were extracted by one reviewer and checked by a second reviewer. Data extracted included, study design, country, critical care unit type or patient condition, sample size, outcome measures, and follow-up assessment timepoints.
Risk-of-bias assessments
Risk of bias was assessed with the quantitative section of the mixed-methods appraisal tool [17]. While this tool was originally designed for mixed-methods reviews, the tool is designed to be used to appraise the quality of purely quantitative studies (as well as other non-mixed-methods designs) [17]. The tool was felt to be proportionate and in line with the scope of this review. All assessments were checked by a second reviewer.
Data synthesis
Analysis was conducted using R (version 4.3.2) [18]. Certain missing data were imputed using the following approaches. Where studies reported only medians, we used these as estimates of the mean. Interquartile ranges (IQRs) were converted to estimates of the standard deviations (SDs) by dividing the IQR by 1.35, and SDs were derived from related statistics when necessary, using established methods [19].
Where the IES-R was presented as the mean score per item (with SD), the overall mean was calculated by multiplying by 22 (items in IES-R). SDs were not derived from the domain-level SDs due to concerns of inter-domain correlation leading to underestimating the true variation. Instead, pooled SDs from studies reporting total IES-R scores were used.
All synthesis was undertaken using Bayesian random-effects models using the R brms package [20]. The planned analysis included three distinct models. The primary model estimated the weighted average of each outcome (distress, anxiety, and depression). The second model employed meta-regression to examine whether the inclusion of bereaved relatives influenced the pooled outcome estimates. The final model (anxiety and depression only) estimated the pooled proportion of participants with HADS scores >7. Model specifications are described in e-Table 7.
We calculated credible intervals (CrIs) and prediction intervals (PrIs) to describe the models. CrIs describe the uncertainty in the estimate of the pooled average (or proportion) given the data and priors. They can be interpreted as the range within which there is a 95% probability that the true pooled average (or proportion) lies. PrIs describe the expected range of estimates (averages or proportions) that might be observed in future studies, given the parameter uncertainty and between-study heterogeneity. Larger between-study heterogeneity will result in wider PrIs.
The primary analyses estimated the weighted averages and 95% CrI for each of the three outcome measures at 3 ± 1 months following critical care. A log-normal model was used to account for potential positive skew and the bounded nature of all three outcomes, as previous research of both family members and people who have experienced critical care admissions have estimated averages closer to 0 than the maximum values on the scales [21–24]. To inform future research and clinical practice, for both HADS anxiety and depression, the probability of a future study in this population reporting clinically relevant average scores (HADS > 7) was estimated.
Meta-regression models assessing the impact of including bereaved relatives were restricted to studies that reported whether bereaved relatives were included in the 3-month follow-up assessment. Meta-regression was only performed when the model included at least 10 studies, and when there were at least 3 studies in each group (i.e., those that did and did not include bereaved participants) [25]. These models included a binary covariate indicating whether bereaved family members were included (yes/no) to examine its association with outcome estimates. Apart from this addition, model specifications and priors matched those in the primary analyses.
The final models estimated the pooled proportion of participants with clinically relevant HADS scores (HADS > 7) [13]. Proportions from individual studies were converted to log-odds of proportions using the R metafor package [26], and synthesised in a Bayesian meta-analysis.
Sensitivity analyses
Sensitivity analyses assessed the robustness of the primary analyses (weighted averages) and the HADS threshold models to prior specification by specifying more conservative priors for the pooled average (see e-Table 7).
Further sensitivity analyses assessed the impact of removing (the control arms) or randomised controlled trials, and separate sensitivity analyses assessed the impact of removing studies with higher than 20% non-response at 3-month follow-up.
All results were back transformed to aid interpretation. We assessed convergence using the potential scale reduction statistic ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\hat{R}$$\end{document} ) and effective sample size (ESS).
Results
Our search returned 9937 unique articles, of which 50 articles met the inclusion criteria (Fig. 1). Following the identification of duplicate cohorts, 45 unique family member cohorts were included in this analysis. Study characteristics are presented in Table 1 [10, 27–74, 78], all 50 studies are referenced (in later figures, the study ID refers to the first instance, where the data plotted were reported). Studies were conducted in 15 countries, with 16 cohorts from the USA.Fig. 1. Study flow diagramTable 1Description of included studiesStudy ID(s)CountryDesignPopulation typeN careers at baselineIncludes bereaved careersOutcomes relevant to this reviewAmass et al. [27]USA and ItalyNon-randomised experimental studyMixed ICU (general/surgical)226YesHADS-A and HADS-DAmass et al. [28]NorwayCohort/cross-sectional studyCOVID-19330YesHADS-A and HADS-DAzoulay et al. [29]France and BelgiumCohort/cross-sectional studyMixed ICU (general/surgical)421YesHADS-A and HADS-DAzoulay et al. [30]FranceCohort/cross-sectional studyARDS602YesIES-R, HADS-A and HADS-DBannon et al. [31]USARandomised controlled trialNeuro (surgical/trauma)10Not statedHADS-A and HADS-DBeesley et al. [32, 33] and Harris et al. [34]USACohort/cross-sectional studyMixed ICU (general/surgical)99YesHADS-A and HADS-DBohart et al. [35]DenmarkRandomised controlled trialMixed ICU (general/surgical)94NoHADS-A and HADS-DCarson et al. [36]USARandomised controlled trialMixed ICU (general/surgical)181YesIES-R, HADS-A and HADS-DCattelan et al. [37]FranceCohort/cross-sectional studyCOVID-1988YesIES-RCox et al. [10, 38]USARandomised controlled trialMixed ICU (general/surgical)47YesIES-R, HADS-A and HADS-Dde Miranda et al. [39]FranceCohort/cross-sectional studyOther: COPD102Not statedIES-R, HADS-A and HADS-Dde Ridder et al. [40]NetherlandsCohort/cross-sectional studyMixed ICU (general/surgical)86YesIES-R, HADS-A and HADS-DDijkstra et al. [41]NetherlandsRandomised controlled trialMixed ICU (general/surgical)233Not statedIES-R^a^, HADS-A and HADS-DFumis et al. [42]BrazilCohort/cross-sectional studyMixed ICU (general/surgical)184YesHADS-A and HADS-DFumis et al. [43]BrazilCohort/cross-sectional studyMixed ICU (general/surgical)186YesHADS-A and HADS-DGarrouste-Orgeas et al. [44]FranceCohort/cross-sectional studyMixed ICU (general/surgical)48YesHADS-A and HADS-DGarrouste-Orgeas et al. [45]FranceRandomised controlled trialMixed ICU (general/surgical)50YesIES-R, HADS-A and HADS-DGarrouste-Orgeas et al. [46]FranceRandomised controlled trialMixed ICU (general/surgical)325YesIES-R, HADS-A and HADS-DGonzalez-Martin et al. [47]SpainRandomised controlled trialCardio-thoracic critical care19NoIES-R, HADS-A and HADS-DGreenleaf et al. [48]USACohort/cross-sectional studyMixed ICU (general/surgical)45YesIES-RHarlan et al. [49]USAOther: mixed methodsMixed ICU (general/surgical)40YesHADS-A and HADS-DHeesakkers et al. [50]NetherlandsCohort/cross-sectional studyCOVID-19197NoHADS-A and HADS-DHenderson et al. [51]ScotlandQuality improvementCardio-thoracic critical care20NoHADS-A and HADS-DHickman et al. [52]USACohort/cross-sectional studyMixed ICU (general/surgical); Neuro (surgical/trauma)101Not statedHADS-A and HADS-DKentish-Barnes et al. [53]FranceRandomised controlled trialMixed ICU (general/surgical)189NoHADS-A and HADS-DKomachi and Kamibeppu [54]JapanCohort/cross-sectional studyMixed ICU (general/surgical)26Not statedIES-RLester et al. [55]USACohort/cross-sectional studyNeuro (surgical/trauma)96YesHADS-ALobato et al. [78]PortugalCohort/cross-sectional studyMixed ICU (general/surgical)246NoHADS-A and HADS-DMatt et al. [56]GermanyCohort/cross-sectional studySepsis143Only extracted data of non-bereavedHADS-A and HADS-DMcAdam et al. [57]USACohort/cross-sectional studyMixed ICU (general/surgical)41YesIES-R^a^, HADS-A and HADS-DMeyers et al. [58–60]USACohort/cross-sectional studyNeuro (surgical/trauma)103Not statedHADS-A and HADS-DMilton et al. [61]SwedenCohort/cross-sectional studyMixed ICU (general/surgical)62NoHADS-A and HADS-DOliveira and Fumis [62]BrazilCohort/cross-sectional studyMixed ICU (general/surgical)118YesHADS-A and HADS-DPetrinec et al. [63]USACohort/cross-sectional studyMixed ICU (general/surgical)112YesIES-RPetrinec [64]USACohort/cross-sectional studyMixed ICU (general/surgical)30YesHADS-A and HADS-DPetrinec and Martin [65]USACohort/cross-sectional studyMixed ICU (general/surgical)48YesHADS-A and HADS-DPetrinec et al. [66]USARandomised controlled trialMixed ICU (general/surgical)25YesHADS-A and HADS-DPetrinec et al. [67]USARandomised controlled trialMixed ICU (general/surgical)30YesHADS-A and HADS-DTorres et al. [68]PortugalCohort/cross-sectional studyMixed ICU (general/surgical)168NoHADS-A and HADS-Dvan Veenendaal et al. [69]NetherlandsCohort/cross-sectional studyCOVID-19102NoHADS-A and HADS-DVeislinger-Burelli et al. [70]FranceNon-randomised experimental studyMixed ICU (general/surgical)77Not statedHADS-A and HADS-DViana et al. [71]BrazilCohort/cross-sectional studyMixed ICU (general/surgical)73Only extracted data of non-bereavedHADS-A and HADS-DVranceanu et al. [72]USARandomised controlled trialNeuro (surgical/trauma)29Not statedHADS-A and HADS-DWiertz et al. [73]NetherlandsCohort/cross-sectional studyCOVID-1957Not statedHADS-A and HADS-DZante et al. [74]SwitzerlandCohort/cross-sectional studyMixed ICU (general/surgical)72YesIES-RARDS acute respiratory distress syndrome, IES-R the Impact of Event Scale—Revised, HADS-A Hospital Anxiety and Depression Scale—Anxiety, HADS-D Hospital Anxiety and Depression—Depression^a^IES-R was presented as the mean score per domain, calculation of overall mean and imputation of SD described in “Methods” section
Twelve were randomised controlled studies, from which control arm data were extracted. The median sample size at baseline assessment was 94.0 (IQR: 47.0–181.0). Five studies were specific to COVID-19-related critical illness, and four included patients with COVID-19 as part of their cohort.
Risk of bias
The risk of bias assessment highlighted risk of non-response bias in many studies (see e-Tables 8–10). We defined risk of non-response bias as having data for <80% of the recruited participants at the 3 ± 1-month assessments. Risk of non-response bias was identified in 16 (40.0%) studies measuring HADS-A, 16 (41.0%) studies measuring HADS-D and 5 (33.3%) studies measuring IES-R. Median follow-up rates at 3 ± 1 months were 86.1% for IES-R, 83.9% for HADS-A, and 83.5% for HADS-D.
Overview of Bayesian approach
All models showed good convergence (all potential scale reduction statistics ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\hat{R}$$\end{document} ) = 1.00; effective sample size (ESS) > 5000), e-Table 11 provides further details of Markov chain Monte Carlo (MCMC) chain convergence and resolution. Posterior predictive checks are presented in e-Figure A.
IES-R
The primary analysis (weighted average) meta-analysis of 15 studies (1640 participants) estimated a back transformed pooled estimate of 18.16 (95% CrI: 12.26–26.23) on the IES-R scale (0–88) (Fig. 2). Between-study heterogeneity was high (τ = 1.97), with a pooled 95% PrI of 4.06–79.29 points, indicating substantial variability in expected study-level effects.Fig. 2. Forest plot of IES-R estimates for family members 3 ± 1-month post-critical care
Sensitivity analysis with a prior assuming a mean of 0, did not meaningfully change the results (pooled estimate: 18.02; 95% CrI: 12.19–26.16). Only one study included only non-bereaved relatives at 3-month follow-up; therefore, no meta-regression analysis was conducted. In further sensitivity analyses, neither removing the RCTs, or studies with high non-response (>20%) meaningfully changed the results as indicated by the inclusive CrIs and high heterogeneity. The non-RCTs sensitivity analysis of 9 studies (878 participants) estimated a back transformed pooled estimate of 19.24 (95% CrI: 10.14–36.05; τ = 2.29). The sensitivity analysis removing studies with high non-response of 10 studies (1447 participants) estimated a back transformed pooled estimate of 16.77, (95% CrI: 10.08–27.12; τ = 2.29).
HADS-anxiety
The meta-analysis of 35 studies (3606 participants) estimated a back transformed pooled estimate of 5.98 (95% CrI: 5.29–6.73) on the HADS-A scale (0–21) (Fig. 3). Between-study heterogeneity was high (τ = 1.47) resulting in a pooled 95% PrI of 2.97–11.94. The estimated probability that a future study will report an average HADS-A score exceeding the clinically meaningful threshold of seven was 37%.Fig. 3. Forest plot of HADS-A estimates for family members 3 ± 1-month post-critical care
Sensitivity analysis with a prior assuming a mean of 0, did not meaningfully change the results (pooled estimate: 5.98; 95% CrI: 5.28–6.74). A sub-analysis was conducted of studies reporting the inclusion of bereaved family members at the 3-month follow-up assessment. In the meta-regression of 28 studies (3036 participants), 11 studies (976 participants) only included family members of survivors. The model included a binary covariate indicating whether bereaved family members were included (yes/no). The model estimated a pooled estimate of 5.73 (95% CrI: 4.72–6.92) on the HADS-A scale. Including non-bereaved participants only was associated with a 1% lower HADS-A score (coefficient estimate on the log scale: −0.01; 95% CrI: −0.32 to 0.30), suggesting similar levels of anxiety in studies that did and did not include bereaved relatives. By calculating Bayesian R^2^ it was estimated that the survival variable explained 0.00% of the observed between-study heterogeneity. In further sensitivity analyses, neither removing the RCTs, or studies with high non-response (>20%) meaningfully changed the results. The non-RCTs sensitivity analysis of 23 studies (2544 participants) estimated a back transformed pooled estimate of 5.43 (95% CrI: 4.56–6.42; τ = 1.46). The sensitivity analysis removing studies with high non-response of 22 studies (2430 participants) estimated a back transformed pooled estimate of 6.59 (95% CrI: 5.74–7.56; τ = 1.35).
The meta-analysis of 11 studies (1066 participants) that reported proportions of participants with HADS-A scores of more than 7 at 3 months after critical care admission estimated a pooled proportion of 0.38 (95% CrI: 0.30–0.47) (Fig. 4). Between-study heterogeneity was high (τ = 0.54), resulting in a pooled 95% PrI of 0.16–0.66. A sensitivity analysis using a prior centred on a mean proportion of 0, did not meaningfully change the results (pooled estimate: 0.38; 95% CrI: 0.29–0.46), indicating that the results were robust to prior specification. In further sensitivity analyses, neither removing the RCTs, or studies with high non-response (>20%) meaningfully changed the results. The non-RCTs sensitivity analysis of 9 studies (852 participants) estimated a pooled proportion of 0.38 (95% CrI: 0.29–0.46; τ = 0.58). The sensitivity analysis removing studies with high non-response of 7 studies (806 participants) estimated a pooled proportion of 0.33, (95% CrI: 0.24–0.54; τ = 0.70).Fig. 4. Forest plot of family members with HADS-A scores ≥8 at 3 ± 1-month post-critical care
HADS-depression
The meta-analysis of 34 studies (3522 participants) estimated a back transformed pooled estimate of 3.91 (95% CrI: 3.39–4.50) on the HADS-D scale (0–21) (Fig. 5). Between-study heterogeneity was high (τ = 1.46) resulting in a pooled 95% PrI of 1.88–8.16. The estimated probability that a future study will report an average HADS-D score exceeding the clinically meaningful threshold of seven was 6.97%.Fig. 5. Forest plot of HADS-D estimates for family members at 3 ± 1-month post-critical care
Sensitivity analysis with a prior assuming a mean of 0, did not meaningfully change the results (pooled estimate: 3.91; 95% CrI: 3.38–4.48). A sub-analysis was conducted of studies that reported whether they included bereaved family members at the 3-month follow-up assessment. In the meta-regression of 26 studies (2800 participants), 8 studies (635 participants) only included family members of survivors. The model included a binary covariate indicating whether bereaved family members were included (yes/no). The model estimated a pooled estimate of 4.21 (95% CrI: 3.42–5.15) on the HADS-D scale. Including non-bereaved participants only was associated with a 23% lower HADS-D score (coefficient estimate on the log scale: −0.26; 95% CrI: −0.64 to 0.11), indicating no clear evidence of a difference associated with excluding bereaved family members. Bayesian R^2^ showed a negligible change (−0.71%) when including the survival variable, indicating it explained virtually none of the observed between-study heterogeneity. In further sensitivity analyses, neither removing the RCTs, or studies with high non-response (>20%) meaningfully changed the results. The non-RCTs sensitivity analysis of 22 studies (2460 participants) estimated a back transformed pooled estimate of 3.68 (95% CrI: 3.07–4.35; τ = 1.44). The sensitivity analysis removing studies with high non-response of 21 studies (2346 participants) estimated a back transformed pooled estimate of 4.26, (95% CrI: 3.49–5.15; τ = 1.51).
The meta-analysis of 11 studies (1092 participants) that reported proportions of participants with HADS-D scores of >7 at 3 months after critical care admission estimated a pooled proportion of 0.20 (95% CrI: 0.15–0.26), see Fig. 6. Between-study heterogeneity was high (τ = 0.41), resulting in a pooled 95% PrI of 0.08–0.40. A sensitivity analysis using a prior centred on a mean proportion of 0, did not meaningfully change the results (pooled proportion: 0.20; 95% CrI: 0.15–0.25). In further sensitivity analyses, neither removing the RCTs, or studies with high non-response (>20%) meaningfully changed the results. The non-RCTs sensitivity analysis of 10 studies (943 participants) estimated a pooled proportion of 0.19 (95% CrI: 0.14–0.26; τ = 0.46). The sensitivity analysis removing studies with high non-response of 7 studies (805 participants) estimated a pooled proportion of 0.25, (95% CrI: 0.12–0.27; τ = 0.46).Fig. 6. Forest plot of family members with HADS-D scores ≥8 at 3 ± 1-month post-critical care
Discussion
This systematic review and Bayesian meta-analysis which included 45 unique family cohorts, shows that family members of people who have experienced a critical care admission have clinically important levels of distress, anxiety and depression in the months following exposure to critical illness. It provides estimates of these important outcomes to inform future research. Interestingly, it has demonstrated that those who have not experienced bereavement have similar rates of depression, anxiety and distress to those who have. Future research in this area is urgently needed to ensure that the entire family unit is supported following a critical care admission.
The findings relating to anxiety may be better contextualised by considering the proportion of family members with clinically relevant levels of anxiety. In this analysis, the estimated probability that a future study will report an average HADS-A score of >7 at 3 months, was 37%, and proportion of family members with anxiety was estimated at 38%. Previous patient cohorts have estimated anxiety prevalence to be 32%, 2–3 months following hospital discharge [24]. Although methods differ, these findings suggest that family members have similar rates of anxiety. While the mechanisms which drive anxiety in patients and family members are likely to differ, this evidence is important to optimise outcomes for people who have experienced a critical care admission. Future research should explicitly include family members in recovery programmes and consider the entire social unit during recovery.
The primary motivation for employing Bayesian methods in this review was to estimate the probability that future studies would report average HADS scores exceeding clinically meaningful thresholds. Unlike traditional frequentist approaches, Bayesian methods provide direct, interpretable probability estimates, which are particularly valuable for informing future research and developing targeted interventions.
Although the IES-R is recommended by expert consensus groups as an outcome measure for people who have a critical care admission [2, 14], it is a screening tool for acute stress disorder (<30 days of symptoms) and post-traumatic stress disorder (30 days or longer), and does not capture DSM-5 diagnostic criteria for PTSD. Its interpretation is further limited by various proposed cutoff thresholds [15, 16]. In this study, pooled IES-R scores of family members were comparable to those reported in a meta-analysis of patients 1–6 months after critical care (20; 95% CI 17–24; 6 studies, I^2^ = 78%) [21]. This suggests family members may experience similar levels of distress to the people who have had a critical care admission. These findings reinforce the importance of developing interventions to support family members of people who survive a critical care admission.
There is limited evidence to guide the implementation of interventions to support family members of survivors, though information provision and enhanced family communication have shown benefits for palliative and bereavement care [75]. Recent quality improvement research has shown that the inclusion of family members in ICU recovery programmes is feasible and may improve outcomes such as depression for family members [5]. Although combining interventions for family members and survivors is acceptable, evidence has also shown that trajectories of symptoms such as anxiety and depression for family members and patients differ over the 12 months after discharge [76]. Future research should examine both the effectiveness of interventions to support family members and the longitudinal pathway of these emotional issues to ensure sustained clinical impact.
While supporting family members (and caregivers) might seem outside the remit of critical care clinicians or the acute hospital system, it is important to recognise the potential impact of not supporting this cohort. Research has demonstrated patients whose family members are ‘strained’ are more likely to be readmitted within 12 months of discharge [9]. Supporting this vulnerable cohort is, therefore, likely to benefit patients, family members and the healthcare system.
Limitations
This systematic review and meta-analysis has limitations. All analyses had high heterogeneity. We have included prediction intervals to support interpretation of our findings within the context of this heterogeneity. Prediction intervals should be interpreted as the expected range in which future studies may estimate the outcome [77]. As evident from the prediction intervals there is large uncertainty as to the likely findings of future studies. We hypothesised that some of the heterogeneity would be explained by the use of a dichotomous variable indicating whether studies included bereaved relatives. However, this variable accounted for little to no between-study variation. Had the included studies provided more consistent reporting on bereavement status, it may have been possible to construct a continuous variable representing the proportion of bereaved relatives per study, which might have explained more heterogeneity. Similarly, removing RCTs or studies with high non-response at 3-month follow-up (>20%) in sensitivity analyses did not provide meaningfully different interpretations of results. Variation in critical care unit types (e.g., general critical care units, and neuro-critical care units) may also contribute to heterogeneity. However, international differences in unit organisation, and because similar patient populations such as those with brain injury may be treated across different unit types, means restricting by unit type could mislead interpretations without addressing the source of the heterogeneity. We also restricted the outcome measures included in the review in an effort to reduce heterogeneity, this decision likely reduced the comprehensiveness of the review. Similarly, by limiting to English language publications we may further have reduced the comprehensiveness of the review. Finally, while we endeavoured to conduct a comprehensive search of the literature, it is possible that including extra databases such as Embase or the Cochrane Central Register of Controlled Trials we would have found additional papers to include.
Conclusion
This systematic review and meta-analysis has demonstrated that many family members of people who have experienced a critical care admission have clinically important levels of anxiety and depression in the months following exposure to critical illness. The Bayesian methods offer direct interpretable probability estimates that future studies could report average scores exceeding clinically meaningful thresholds using the predominant screening tools for anxiety and depression (HADS). To ensure optimal outcomes, future research in this area is urgently needed to ensure that the entire family unit is supported following a critical care admission.
Supplementary Information
Additional file 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cox CE, Hough CL, Carson SS, et al. Can coping-skills training help patients who have received intensive hospital care to cope with depression and anxiety? Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2018. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 591018/37079709 · pubmed ↗